


Abstract
Pseudoprogression (PsPD) is a pathological feature recently reported by some authors in malignant glioma patients treated with radiotherapy in combination with temozolomide. In radiological imaging, it is shown as an increase in the size of the tumor lesion and contrast enhancement occurring within a few months from the completion of radio-chemotherapy without worsening of the neurological signs and symptoms. In 21%-50% of the patients, the same lesion disappears a few months after its appearance. In 12 glioblastoma patients treated with radio-chemotherapy, 4 cases of early radiological progression without discontinuation of temozolomide treatment are reported. At the sunsequent tumor assessment, 2 cases (13%) were revealed to be PsPD. The two patients who experienced PsPD had the longest progression and survival times of all patients. In both patients with PsPD, the O6-methylguanine-DNA methyltransferase (MGMT) promoter was found to be methylated. The PsPD phenomenon opens the prospect of a new era for the management of glioblastoma patients undergoing radio-chemotherapy.
Pseudoprogression (PsPD) is a recent finding reported in newly diagnosed, malignant glioma patients treated with radiotherapy and concomitant chemotherapy with the alkylating agent temozolomide (1, 2). The radiological imaging performed within 3-6 months of completion of the combined treatment shows an increase both in tumor size and contrast enhancement without worsening of the neurological signs and symptoms of the patient. Notwithstanding this evidence, in 21%-50% of patients the disappearance of the lesion is documented a few months after its appearance (1, 2). The causes of this phenomenon are not completely understood. One possible explanation is that the activity of temozolomide in association with radiation therapy could be capable of killing the cancer cells with secondary tissue reactions such as edema and permeation of the vascular endothelia in the tumor area. The highest incidence of PsPD has been shown for patients with methylation of the O6-methylguanine-DNA methyltransferase (MGMT) promoter (2), confirming, probably, greater activity of the combined treatment in this subset of patients. The improvement of survival in the patients who demonstrated PsPD and MGMT methylation is an important finding in clinical practice (2), but it must be confirmed by further experience. The present report supports the evidence of PsPD in glioblastoma patients submitted to radio-chemotherapy and underlines that the subset of patients with MGMT promoter methylation experiencing PsPD have improved time to progression and survival. The management of PsPD in clinical practice is also discussed, focusing attention on the evaluation of the rise of this phenomenon after radiotherapy combined with temozolomide and with maintenance temozolomide.
Case Report
Between November 2006 and April 2008, twelve patients with newly diagnosed gliobastoma were treated at our institution with radiotherapy combined with temozolomide. Table I shows the patient characteristics.
Radiotherapy consisted of involved-field irradiation at a dose of 2.0 Gy per fraction given once daily for 5 days (Monday to Friday), over a period of 6 weeks, for a total of 60 Gy. The radiotherapy was administered using a linear accelerator with 6 to 15 MV photons and using a highly conformal three-dimensional-radiotherapy (3D-RT) technique. Concomitantly to radiation therapy, the patients received temozolomide 75 mg/m2/d for six weeks, followed by temozolomide 200 mg/m2/d for 5 days, every 28 days until disease progression (3). The patients started radio-chemotherapy within 40 days after the surgical procedures. Also within 40 days from surgery up to 7 days before radio-chemotherapy, 40 days after the end of treatment and then every 2-3 months, magnetic resonance imaging (MRI) of the brain was performed with a superconductive machine before and after contrast medium infusion (gadolinium-DTPA 0.2 mmol/kg). The radiological response was assessed according to the criteria of Macdonald et al. (4).
Magnetic resonance imaging (MRI) assessment, outcome of disease and correlation with MGMT promoter status.
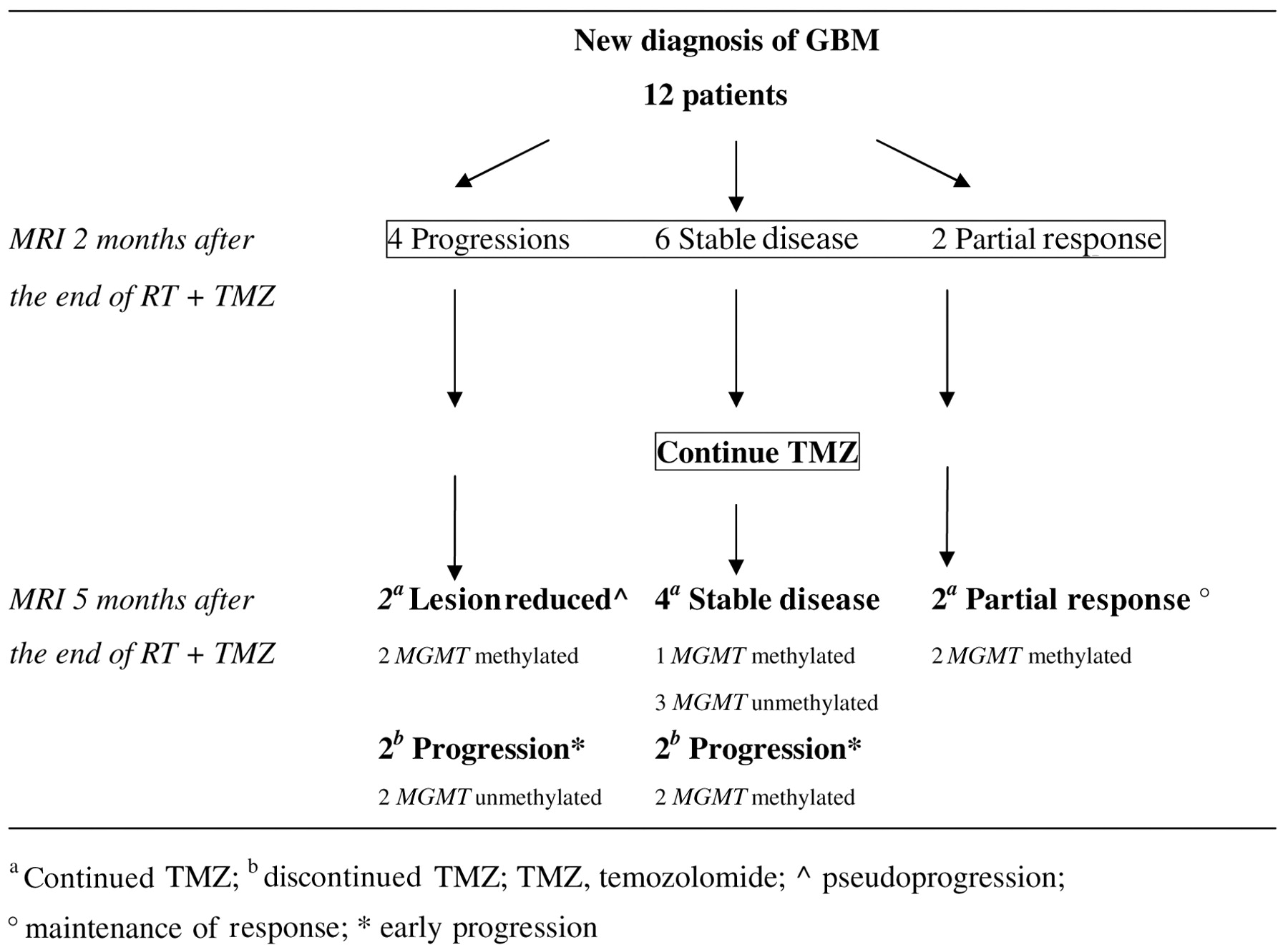
The MRI assessment and outcome of disease are shown in Figure 1. Two months after the end of radio-chemotherapy 4 progressive disease, 6 stabilizations and 2 partial responses were observed. Treatment was continued in all the patients, including those with evidence of an increase in the tumor lesion. Five months after the end of radio-chemotherapy, MRI showed complete disappearance of tumor in 2 of the 4 progressive patients. Figure 2 shows one of the two cases in which PsPD was documented. The two patients with PsPD were 63 and 65 years old and received the same dose of radiotherapy (total dose 60 Gy) and temozolomide (200 mg/m2/d for 5 days, every 4 weeks). In both patients, no significant worsening of the neurological signs and symptoms was observed during the combined therapy and following temozolomide alone; the time to progression was 7.6 and 9.1 months, survival was 20.5 and 24.8 months, respectively, and the MGMT promoter was methylated in both cases. In contrast, the remaining two patients with evidence of progression at the first MRI after radio-chemotherapy underwent further progression of disease. Their time to progression and survival were 4.5, 4.8 months and 12.3 and 12.2 months, respectively; the MGMT promoter was unmethylated in both cases.
Demographic characteristics.

Case of a glioblastoma patient with PsPD during maintenance temozolomide. MRI SE T1 sequences after Gd-DTPA infusion. A: presurgical evaluation; tumor in the right temporal lobe; B-C: 40 days after radiotherapy combined with temozolomide treatment; no tumor lesion shown. D-E: 2 months after radio-chemotherapy; MRI shows a nodular area of enhancement after contrast medium infusion at the site of surgery and in the medial right temporal lobe (arrows). Both areas were included in the field of radiation therapy. F-G: 5 months after radio-chemotheapy; no enhancement after contrast medium infusion in the right temporal lobe.
The patients with PsPD continued chemotherapy with temozolomide until disease progression (total cycles 9 and 10, respectively), while those with progression were switched to second-line chemotherapy.
Discussion
Among the patients with newly diagnosed glioblastoma, the subgroup with MGMT promoter methylation of the tumor appears to benefit the most from the addition of temozolomide to radiotherapy (5). This enzyme repairs the DNA damage caused by alkylating agents such as temozolomide and this injury to DNA culminates in apoptotic cell death. Methylation of the promoter of MGMT turns off transcription of the gene, reducing the intracellular level of MGMT and inhibiting the repair mechanism. The study by Stupp et al. demonstrated that the prognosis was better for the glioblastoma patients receiving radio-chemotherapy including temozolomide, in which there was methylation of the MGMT promoter, than for those without the methylation (3). The recent article by Brandes et al. demonstrated that PsPD correlated significantly with methylation of the MGMT promoter in patients undergoing concurrent radiotherapy plus daily temozolamide followed by maintenance temozolomide (2). The patients with methylated MGMT promoter had a higher probability of PsPD (91.3%) as opposed to those with unmethylated MGMT promoter (41%) (2).
Importantly, PsPD lesions usually occur within six months from the completion of radiotherapy (1), as was the case of our two patients with PsPD. This early onset might help differentiate PsPD from radionecrosis which has similar radiological findings to PsPD but a rather late emergence (6, 7).
The present cases confirm that patients with PsPD are more likely to have methylation of the MGMT promoter, also confirming that PsPD patients have a longer time to progression and survival than those with confirmed disease progression. These data could be related either to an intrinsic better outcome for patients with tumors with MGMT methylation or a better response to radio-chemotherapy in patients with PsPD.
From the histopathological features, PsPD represents a continuum between the subacute radiotherapy reaction and treatment-related necrosis including edema, gliosis, endothelial-cell apoptosis, fibrinoid deposition, hyalinization, thrombosis and finally vessel occlusion, causing increased contrast enhancement by neuroimaging. In particular, the endothelial-cell apoptosis induced by the radiation is mainly membrane-damage dependent and it is a process related to various intracellular molecular pathways (phosphokinase proteins, caspase) (8). Temozolomide-induced DNA damage associated with radiotherapy-induced DNA/membrane damage might activate the molecular pathways leading to an increase of endothelial-cell death; these events could explain the higher incidence of PsPD in patients treated with temozolomide radio-chemotherapy.
The appearance of radiological abnormalities, such as PsPD, might prompt a change in clinical practice, as they could be mistaken as being the result of inefficient treatment. In glioblastoma patients who have MGMT promoter methylation and who show radiological progression, the ongoing treatment should not be modified, since the response could be due to an early-delayed reaction to radiotherapy. Like the legend of the mythological three-headed dog Cerberus, the MGMT status is, from now, a marker for glioblastoma, able not only to predict the outcome of disease and the response to temozolomide treatment, but also to better address the diagnostic and therapeutic choices some months after the end of radio-chemotherapy. Neverthless, in the absence of prospective studies, it is reasonable to continue maintenance temozolomide in patients without methylation who have radiological evidence of disease progression and no worsening of the neurological signs and symptoms. However, this last group of patients should be subjected to a closer clinical-instrumental follow-up to identify those individuals whose progression is real as early as possible.
For this reason, additional prospective studies are still necessary to determine the degree of correlation between MGMT status and PsPD incidence in newly diagnosed glioblastoma patients following radiotherapy concomitant with temozolomide treatment.
- Received January 27, 2009.
- Revision received April 14, 2009.
- Accepted May 5, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.