


Abstract
This retrospective analysis was designed to confirm the predictive role of urokinase-type plasminogen activator (uPA) and plasminogen activator inhibitor type I (PAI-1) in the outcome of early stage, node-negative breast cancer patients. Patients and Methods: Node-negative patients having not received adjuvant chemotherapy, and for whom frozen samples were available, were selected. Results: Among the 169 patients included, 56.8% presented with uPA >3 ng/mg of proteins and/or PAI-1 >14 ng/mg of proteins. The median follow-up was 73 months. Significant correlations were found between uPA and disease-free survival (p [univariate]=0.003; p [multivariate]=0.01), and between uPA, PAI-1, and uPA plus PAI-1 and distant relapses (p=0.002). No significant correlation was found between uPA/PAI-1 and the risk of locoregional recurrence. Conclusion: This study demonstrated that uPA and PAI-1 are useful predictors of distant metastases in a subset of early stage, node-negative breast cancer patients.
- Node-negative breast cancer
- urokinase-type plasminogen activator
- plasminogen activator inhibitor type I
- prognostic factor
- distant metastases
- local recurrence
Currently, the incidence of newly diagnosed breast cancer is increasing with a stable mortality (1). Mammography screening and therapeutic improvement explain part of this change. In Europe, nearly 90% of breast cancers are non-metastatic at diagnosis, and more than 60% are node-negative (2). Therefore, node-negative breast cancer patients represent the majority of patients, requiring a suitable management. If these patients seem to have a better prognosis, the incidence of relapse remains an issue. A prospective analysis in patients not receiving adjuvant therapy showed that except for a small favourable subgroup, the rate of 10-year metastatic relapse ranged from 15% to 35% (3). A major concern is the screening of node-negative patients eligible for adjuvant treatment, especially for chemotherapy. The Early Breast Cancer Trialists' Collaborative Group overview demonstrated a significant advantage of polychemotherapy versus no adjuvant treatment, irrespective of lymph node involvement (1). Two consensus statements (National Institutes of Health, St. Gallen) defined patients eligible for adjuvant therapy according to the classical prognostic factors (4, 5). Although their conclusions differed regarding patients who could benefit from adjuvant treatment, up to 90% of node-negative patients would be candidates for adjuvant chemotherapy, when only about 30% of patients would relapse. This discrepancy highlights a need for additional prognostic markers.
To date, the most conclusive monogenic markers are the urokinase-type plasminogen activator (uPA) and plasminogen activator inhibitor type I (PAI-1) system (6-9). The fibrinolytic system is not only involved in the intravascular dissolution of fibrin, but it also plays a vital role in normal physiologic reproduction, wound repair, angiogenesis and tissue remodelling. Fibrinolysis is also a vital component in the pathogenesis of neoplastic disease. It is essential in releasing cells from their primary site of origin, providing nutrition for neoplastic cell growth and promoting cell mobility and motility (10). It was shown that the uPA/PAI-1 system played an important role in tumour invasion and metastasis (11-13), interacting with the matrix metalloproteases system (14). A German team was the first to demonstrate that tumour concentrations of uPA and PAI-1 were a prognostic factor for lymph-node positive and negative breast cancer patients (6-9). This has been confirmed by a pooled analysis performed by the European Organization for Research and Treatment of Cancer-Receptor and Biomarker Group (EORTC-RBG) involving 8377 patients of 18 datasets (15).
The purpose of this single-institution retrospective analysis was to determine if the prognostic role of uPA/PAI-1 remained relevant in a population of patients with early stage breast cancer, as previous clinical trials were conducted in poor-prognosis disease. Consecutive node-negative patients who did not receive adjuvant chemotherapy, and for whom frozen samples were available, were selected.
Patients and Methods
Study population. From January 1st 1996 to December 31st 1998, 720 consecutive primary operable, invasive, node-negative early breast cancer patients were selected from the breast cancer data base (Institut Curie, Paris, France) for a retrospective analysis. In 203 patients, frozen cytosols extracted from tumour tissues in liquid nitrogen, which remained available after routine estrogen- (ER) and progesterone receptors (PgR) analysis, as previously described (16), allowed a retrospective measurement of uPA and PAI-1. To be eligible for the analysis, patients were not to have received adjuvant chemotherapy. The final population included 169 patients treated exclusively by initial surgery and radiotherapy, with or without adjuvant hormonotherapy. The characteristics of patients for whom frozen samples were available (n=169) and for patients for whom they were not (n=551) were compared, ensuring the absence of bias in the selection of patients.
All patients were examined routinely every 6 months during the first 5 years of follow-up and yearly thereafter, according to institutional guidelines. The data reviewed, recorded in the hospital files, were baseline clinical and pathological data, the occurrence of events (local relapse, regional relapse, distant relapse, contralateral breast cancer and second malignancy), and death. The extraction of data was performed in October 2004, corresponding to the cut-off date for analysis.
The protocol was approved by the Institutional Committee of Clinical Research.
Laboratory assays. The uPA and PAI-1 protein concentrations were determined in breast tumour cytosols with commercially available ELISA kits (Immubind uPA and Immubind PAI-1; American Diagnostica, Greenwich, CT, USA) as previously described (17), and following the manufacturer instructions. The antigen concentrations for uPA and PAI-1 were expressed as ng/mg of proteins. The threshold of uPA was 3 ng/mg of proteins and PAI-1 was 14 ng/mg of proteins, according to the cut-off values previously described in the literature (8,15). To enable the assessment of between-assays coefficient of variations (CV), an aliquot of a pooled breast cancer sample cytosol was analysed in each assay. All samples were analysed in independent duplicates. The CVs of samples measured in duplicate were all lower than 5% .
Statistical analysis. The study sample consisted of 169 patients. Qualitative data were presented as a percentage of sample size, and quantitative data were described using mean, standard deviation, median and range.
In the univariate model, correlations between quantitative data were estimated using the Pearson coefficient and compared by the Pearson test. If the data were not normally distributed, Spearman coefficient and test were used. Means were compared using an analysis of variance or a Kruskal-Wallis test in the absence of variance equal terms, confirmed by a Bartlett test. The chi-square test was used to compare proportions, and replaced by Fisher exact test if the expected frequency in any cells of the contingency table was less than five.
Analysed events were local relapses, regional relapses, distant metastases and death. Computerized survival data were defined as the time from diagnosis until the occurrence of event, namely disease-free survival (DFS) including locoregional and distant relapses, distant disease-free survival (D-DFS), locoregional disease-free survival (L-DFS) and overall survival (OS). Relapse-free and alive patients were censored at the date of their last known contact. The DFS, D-DFS, L-DFS and OS rates were calculated by the Kaplan-Meier method and groups were compared using a log-rank test.
To obtain two groups of uPA and PAI-1 concentrations, the determination of a cut-off value by successive cutting out was computed using a Cox proportional risks model. A Wald test was used to evaluate the prognostic value of this variable on events.
The effect of covariates on survival parameters was also assessed through Cox models. When step-wise regression techniques were used to identify the most significant covariates, the significance level for a variable to be entered into a model or to be removed from a model was 0.20. Presented data included percentage of sample size, survival rate, adjusted and non-adjusted hazard ratio (HR) with a 95% confidence interval (95% CI), at 2, 4 and 6 years of follow-up. All the analyses were performed using S-Plus 2000 software (MathSoft Inc., Seattle, WA, USA).
This analysis has been conducted according to REMARK guidelines for tumour markers reported by the Statistics Subcommittee of the NCI-EORTC Working Group on Cancer Diagnostics (18).
Results
Patient characteristics. The baseline characteristics of patients who were selected based on available frozen samples did not differ from those of patients for which frozen samples were not available (data not shown). The main characteristics of the 169 selected patients are summarised in Table I. All patients had a breast-conserving surgery followed by a whole breast irradiation (median dose 50 Gy; range, 45 to 58 Gy). An additional dose was delivered to the tumour bed (median dose 15 Gy; range, 10 to 24 Gy) in 130 patients (77%). The median total dose delivered was 65 Gy (range, 48 to 73 Gy). Thirty patients (18%) received adjuvant tamoxifen.
Among the 169 patients, 56.8% of the patients presented with a high concentration of uPA (>3 ng/mg of proteins) and/or PAI-1 (>14 ng/mg of proteins). The mean value of uPA was 2.7 ng/mg of proteins (median=2.1; range, 0.3 to 13.7), and the mean value of PAI-1 was 18.5 ng/mg of proteins (median=13.8; range, 4.6 to 75.5).
Patient and tumour characteristics of the 169 analysed patients.
Correlation between uPA/PAI-1, baseline characteristics and disease outcome: univariate analysis. The uPA and PAI levels were significantly correlated (r=0.72; p<0.001). A level of uPA >3 ng/mg of proteins was significantly correlated with a ductal histological subtype, peritumoral invasion, a PAI-1 value >14 ng/mg of proteins and to the delivery of an additional irradiation dose (Table II). The mean total radiation doses delivered were 61.0 Gy when uPA ≤3 ng/mg proteins and 63.7 Gy when uPA >3 ng/mg proteins (p=0.04). When PAI-1 >14 ng/mg of proteins, patients were more likely to have a ductal carcinoma, a Scarff-Bloom Richardson (SBR) histological grade II-III, a negative ER status and an uPA value >3 ng/mg of proteins. The combined concentrations of uPA and PAI-1 were significantly correlated with histological feature, SBR histological grade, ER and an additional boost of radiotherapy (Table II). When uPA and/or PAI-1 concentrations were high, patients were more likely to have a ductal carcinoma, a SBR histological grade II-III, a negative ER status and to have received an additional boost of radiotherapy. No correlations were found with age and tumour size.
The median follow-up was 73 months (range 3 to 102 months). The DFS rates were 95%, 88% and 82% at 2, 4 and 6 years, respectively. The pattern of events are summarised in Table III. The relative risk (RR) of relapse was significantly higher in patients having an uPA level >3 ng/mg of proteins (RR=2.76; 95% CI, 1.37 to 5.56; p=0.003), whereas PAI-1 and the combination of uPA and PAI-1 were not associated with a higher risk of relapse (p=0.28 and p=0.15, respectively) (Figure 1). The other prognostic factors significantly associated with the risk of relapse were age ≤ 50 years (p=0.004), premenopausal status (p=0.01), tumour size > 20 mm (p=0.003) and SBR histological grade II-III (p=0.004). No significant correlation was found between uPA/PAI-1 and the risk of locoregional relapse, even when adjusted to radiation doses. On the other hand, a significant correlation was found between the risk of distant relapse and uPA (RR=6.08; 95% CI, 1.64 to 22.50; p=0.002), PAI-1 (RR=11.2; 95% CI, 1.45 to 86.92; p=0.002) and the combination of uPA and PAI-1 (p=0.002) for which the RR was not assessable because no event occurred in the low concentration group (Figure 2).
Correlation between uPA/PAI-1 and disease outcome: multivariate analysis. The initial model included variables for which the level of significance in the univariate analysis was lower than 20% . The selected variables were age, menopausal status, tumour size, SBR histological grade, ER status, uPA and PAI-1.
The Cox regression analysis demonstrated that age, tumour size, SBR histological grade and uPA were significantly associated with the DFS (Table IV). Furthermore, uPA, PAI-1 and combined markers were significantly associated with the risk of distant relapse (p=0.002), but not with the risk or locoregional recurrence.
Significant correlations between uPA/PAI-1 and baseline characteristics: univariate analysis.
Crude rates of first events.
Discussion
This retrospective analysis was designed to study the prognostic role of uPA and PAI-1 in a subset of patients who had an early stage, node-negative breast cancer. In these patients who were not suitable for adjuvant chemotherapy according to standard practices during the recruitment period, the baseline characteristics were of favourable prognosis according to classical prognostic factors, as 66% of the patients had a tumour size ≤20 mm, a SBR histological grade I in 40% of them and an ER-positive status in 90% . In spite of these characteristics, an elevated level of uPA and/or PAI-1 was found in more half of the population. The uPA and PAI-1 levels were significantly correlated and a high level of uPA and/or PAI-1 was significantly correlated with ductal carcinoma, peritumoral invasion, SBR histological grade II-III, ER-negative status and radiation dose to the tumour bed. After a median follow-up of 73 months, uPA >3 ng/mg of proteins was associated with the risk of relapse and both markers were correlated with the risk of distant relapse, whereas no correlation was found between high levels and locoregional relapse.
Prognostic factors of disease-free survival: Cox regression analysis.
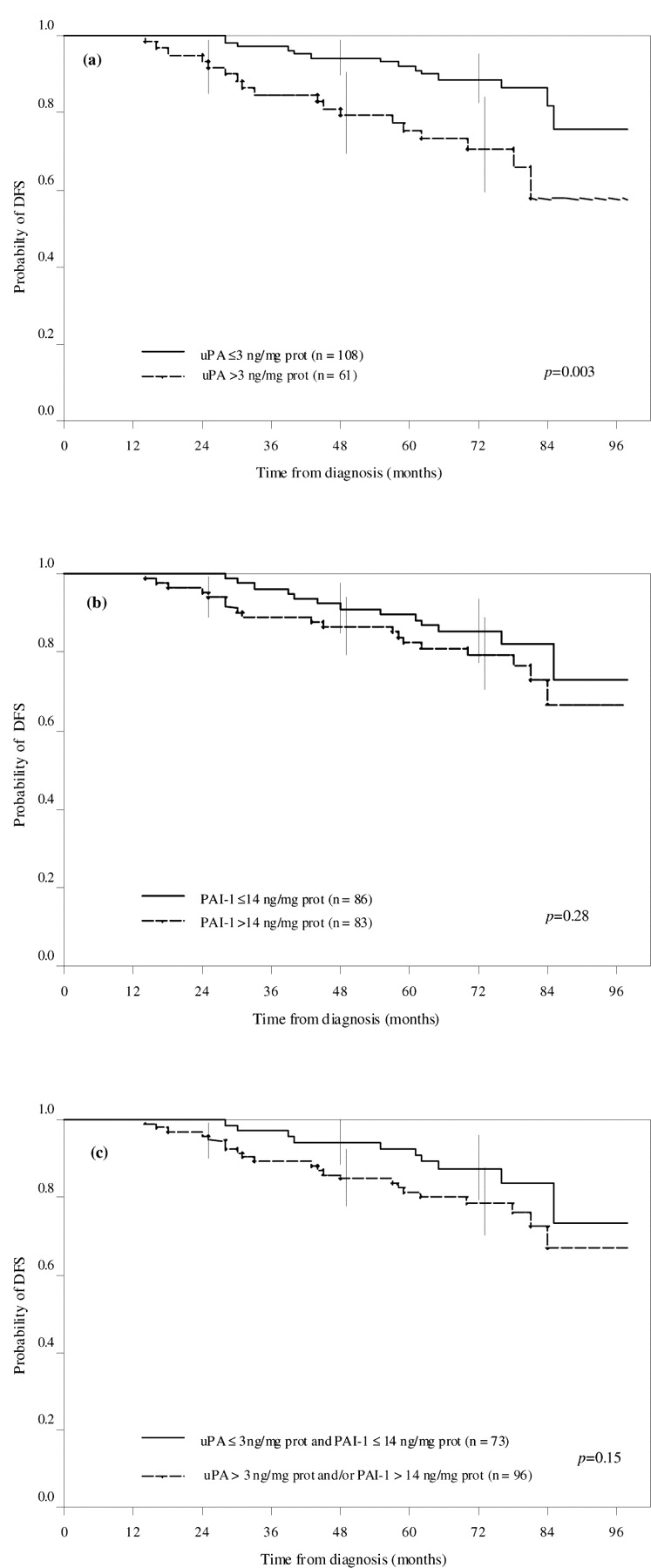
Probability of disease-free survival according to the level of uPA (a), PAI-1 (b) and uPA/PAI-1 (c).

Probability of distant disease-free survival according to the level of uPA (a), PAI-1 (b) and uPA/PAI-1 (c).
There is a strong rational to use uPA and PAI-1 as biomarkers of tumour aggressiveness. uPA is causally involved in cancer invasion and metastasis (19), explained by its ability to stimulate angiogenesis, mitogenesis and cell migration, and to modulate cell adhesion (11). More recently, uPA was also shown to prevent apoptosis (20). Because PAI-1 is an inhibitor of uPA, it might be expected to prevent invasion and metastasis. In breast cancer, the prognostic information provided by uPA was independent of the conventional prognostic factors, and importantly, was prognostic in node-negative patients (12, 21).
Clinical validation should be carried out using a level-1 evidence study with either a large randomised prospective trial in which evaluation of the marker is the primary objective, or a meta-analysis/pooled analysis of small-scale prospective or retrospective trials (22). As regards uPA and PAI-1, both of these requirements have now been met (8, 15). In the prospective randomised trial conducted in Germany, involving 556 node-negative breast cancer, patients having low concentrations of both markers had a 3-year relapse rate of 6.7%, whereas those having high concentrations of uPA and/or PAI-1 had a relapse rate of 14.7% (p=0.006) (8). After a median follow-up of 79 months, the pooled analysis, involving 8377 patients of 18 datasets, showed that both uPA and PAI-1 were independent prognostic factors, and predicted outcome in the subgroup of node-negative patients that did not receive any adjuvant treatment (15). The patients selected in the present analysis have a better prognosis profile than those included in previous studies. In spite of this, it was found that uPA and PAI-1 kept their prognostic impact, essentially to predict the risk of distant recurrences. In this series, age, node involvement and SBR histological grade were the factors associated with the risk of local recurrence, as previously described (23-25). To date, no other level 1 validated biological factors have been identified. Some hypotheses arise, such as a low level of phosphorylated insulin-like growth factor 1-receptor in unselected breast tumours, requiring confirmations (26).
These additional findings raise the question of whether adjuvant chemotherapy should not be given to patients with low concentrations of these markers, and which type of chemotherapy would be most appropriate in patients with high concentrations. One large prospective trial (NNBC-3) is currently ongoing, stratifying the treatment of node-negative patients according to their risk of relapse (27). A high risk of relapse was defined according to either St. Gallen criteria, which have evolved since the onset of the study, or high concentrations of uPA/PAI-1 plus SBR histological grade II-III. Those patients were randomised between 6 cycles of FEC 100 or 3 cycles of FEC 100 followed by 3 cycles of docetaxel as in PACS 01 trial conducted in node-positive patients (28). The aim of this trial was to determine the benefit of a sequential anthracycline-docetaxel regimen in high-risk, node-negative breast cancer patients compared to a current standard anthracycline-based chemotherapy.
No study has evaluated the impact of radiotherapy on the risk of local recurrence in high-risk patients as determined by UPA and/or PAI-1 levels. This series of patients had consecutive registrations for dose and irradiated sites. No significant correlation was found between uPA/PAI-1 and the risk of locoregional relapse, even when adjusted to the irradiation dose.
Technical issues were not to be considered as a limiting factor in this study, as the commercially available ELISA kits used had been validated in multicentre studies (8, 15, 29, 30), with external quality assurance as a result of the work from the EORTC/RBG group (31). Robustness and high sensitivity of these assays were assessed, even in small tumour specimens (32). Furthermore, all well-conducted clinical trials and retrospective analyses (8, 15, 29, 30), including this one, have found homogeneous cut-off values for both uPA and PAI-1 at 3 and 14 ng/mg of proteins, respectively. Other assays, including quantitative RT-PCR for the determination of uPA and PAI-1 in tumours mRNA were not accurately correlated with protein expression and could not be substituted for antigen determination (33). However, in this population of early breast cancer, few events are recorded that can decrease the statistical power of the analysis, but its accuracy is given by the homogeneity of the group of patients, both in clinical feature and treatment.
To date, uPA and PAI-1 are among the first tumour markers that have their clinical value confirmed in level-1 evidence studies. Their usefulness is clearly higher in the subset of node-negative disease, and they have the potential to individualise treatment strategies. The current limitation of their use in routine practice is a poor diffusion of the ELISA kit as well as the availability of frozen materials mandatory to perform the analysis, which deserves to be improved. New techniques of gene profiling emerge, requiring more complex methods, and comparisons between uPA/PAI-1 and the 70- or 21-genes signature should be explored (34, 35).
In conclusion, uPA and PAI are powerful prognostic markers, which, in combination with standard clinical and pathological factors, could help to discriminate patients on whom, in this favourable node-negative subset of patients with small breast cancer, chemotherapy may be avoided.
Acknowledgements
We thank Chantal Gauthier and Yann de Rycke for providing their assistance in the selection of patients. We thank Evelyne Boudou, Martine Thioux, Catherine Barbaroux, Carine Tran-Perennou for their technical assistance.
Members of the Breast Cancer Study Group in addition to co-authors: Bernard Asselain, Alain Aurias, Emmanuel Barillot, François Campana, Paul-Henri Cottu, Jean-Yves Pierga, Marie-France Poupon, Dominique Stoppa-Lyonnet, Anne Tardivon, Fabienne Thibaut, Pascale This. Isabelle Chapelle-Marcillac provided writing assistance in the preparation of the manuscript.
- Received December 3, 2008.
- Revision received January 23, 2009.
- Accepted February 12, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}