


Abstract
Background: Claudins are essential tight junctional proteins between adjacent epithelial, mesothelial or endothelial cells, and are responsible for the permeability of the paracellular space. The expression of claudin-5 and its correlation to ovarian cancer behavior was investigasted. Materials and Methods: A total of 85 serous ovarian cancer tissue samples were analyzed using immunohistochemical staining. Results: An association between claudin-5 expression and cancer grade (p=0.016) and advanced stage (p=0.022), strongest claudin-5 expression was found in advanced stage and high-grade carcinomas. An association between claudin-5 expression and cancer-specific (p=0.032) and overall survival (p=0.026) was also found. Only 25-30% of claudin-5-positive patients, but 60% of claudin-5-negative patiens were alive at the 5-years follow-up. Conclusion: Increased claudin-5 expression is associated with aggressive behavior in serous ovarian adenocarcinoma.
Ovarian cancer is the fourth most frequent cause of death by cancer in women and the most fatal of gynecological tumors in Finland (1, 2). Less than 30% of women with advanced stage disease have long-term survival. When diagnosed at an early stage (International Federation of Gynecology and Obstetrics, FIGO), most patients can be cured with conventional surgery and chemotherapy. At present, only 25% of ovarian carcinomas are detected in stage I due, in part, to the absence of specific symptoms and to the lack of an effective screening strategy (3). Most of the malignant ovarian neoplasms are epithelial tumors: 25-35% serous, 15-20% endometrioid and 5-10% mucinous tumors (4).
Claudins are essential tight junctional proteins between adjacent epithelial, mesothelial or endothelial cells, and they are responsible for sealing of the paracellular pathway (5). There are at least 24 claudins known so far. They participate in regulation of epithelial cell permeability and take part in forming different barriers (6). Claudin-5 is expressed mainly in endothelial cells and is involved in the formation of the blood-brain barrier (7, 8). It is highly expressed in vascular endothelial cells (6, 9) and in vascular tumors (9, 10). Our preliminary study showed that claudin-5 overexpression was present in ovarian epithelial tumors and its expression appeared to be induced in malignant epithelial tumors such as serous cystadenocarcinomas, mucinous cystadenocarcinomas and endometrioid adenocarcinomas (11).
Considering the fact that the expression of claudin-5 has been found to be stronger in malignant ovarian epithelial tumors than benign ones (11), the aim of this study was to further evaluate claudin-5 expression, its correlation to clinical conventional parameters and its prognostic meaning in serous ovarian cancer. In the literature no studies have reported about claudin-5 correlation to conventional prognostic factors in ovarian cancer.
Materials and Methods
Patients and tissue samples. The study population consisted of 85 serous ovarian cancer patients treated in the Department of Obstetrics and Gynecology, Oulu University Hospital. Histological material was collected from the files of the Department of Pathology, University of Oulu. The tissue samples had been collected from the primary tumors. All the samples had been fixed in 10% buffered formalin and embedded in paraffin. Clinical and follow-up information including age, height, weight, survival status (alive/dead of ovarian cancer/dead of other disease), overall survival, relapse free survival, histology, FIGO stage, grade, presence of ascites, size of residual tumor, peritoneal fluid or ascites cytology, CA 12-5 level and chemotherapy was collected.
The median age of the serous ovarian adenocarcinoma patients was 59 (37-81) years and the median body mass index (BMI) was 25 kg/m2 (range 18-38). There were 11 well- (grade 1), 28 moderately (grade 2) and 46 poorly (grade 3) differentiated tumors. Six out of the 85 ovarian carcinomas were detected at stage I, four at stage II, 55 at stage III and 20 at stage IV. Ascites was present in 67 (79%) cases. After the primary operation no residual tumor remained in 24 out of the 85 (28%, 1 missing) patients. Most of the patients (82 out of the 85, one missing) received cisplatin-based chemotherapy after surgery.
The ovarian cancer samples consisted of 38 serous adenocarcinomas, 27 serous cystadenocarcinomas, 19 serous papillare cystadenocarcinomas and 1 serous papillare adenocarcinoma.
Immunohistochemistry. Before the application of primary antibody, the sections were heated in a microwave oven in 10mmol/l citrate buffer, pH 6.0, for 10 minutes. After a 60-minute incubation with the primary antibody (mouse anti-claudin 5, clone 4C3C2, dilution 1:50; Zymed Laboratories Inc, South San Francisco, CA, USA), a biotinylated secondary anti-rabbit antibody and a Histostain-SP kit (Zymed Laboratories Inc.) were used. The primary antibody has been previously characterized (12, 13). The color was developed by diaminobenzidine, whereafter the sections were lightly counterstained with hemotoxylin and mounted with Eukitt (Kindler, Freiburg, Germany). Negative control stainings were carried out by substaining non-immune mouse serum and phosphate-buffered saline for the primary antibody. Only membrane-bound immunoreactivity was considered significant. The immunostaining was assessed as follows: −=no immunostaining present; +=less than 25% of cells positive; ++=25%-50% of cells positive; +++=50%-75% of cells positive; ++++=75%-100% of cells positive.
Statistical analyses. Statistical analyses were performed using the SPSS program (v. 16.0). The material was divided into negative and positive groups for statistical analyses; samples with 0% positive stained cells were regarded as negative, all others as positive. The Pearson Chi-square test was used for the contingency tables of the discrete variables. When analyzing continuous data, the Mann-Whitney U-test was used. Survival analyses were performed according to the Kaplan-Meier method. The analyses were carried out using the log-rank test. The multivariate analysis of survival was performed using the Cox proportional hazard technique with a backward stepwise procedure. The variables tested in the multivariate analysis included FIGO stage (I+II vs. III-IV), grade (1 vs. 2 vs. 3), and claudin-5 (negative vs. positive). Survival was calculated from the date of surgery to the date of death or to the closing date of this study. A p-value <0.05 was considered statistically significant.
Results
Seventy-five out of the 85 (88%) samples were claudin-5 positive (Figure 1). There was a significant difference in claudin-5 expression between claudin-positive and -negative samples according to cancer grade (p=0.016) (Figure 2). Claudin-5 expression was detected in 92% of the grade 2 and grade 3 carcinomas, but only in 64% of the grade 1 carcinomas. Strong intensity of staining, i.e. 50-100% of the cells positive, was found in 39% of the grade 3 and in 39% of grade 2 carcinomas. The corresponding figure for the grade 1 tumors was 18% (Table I).
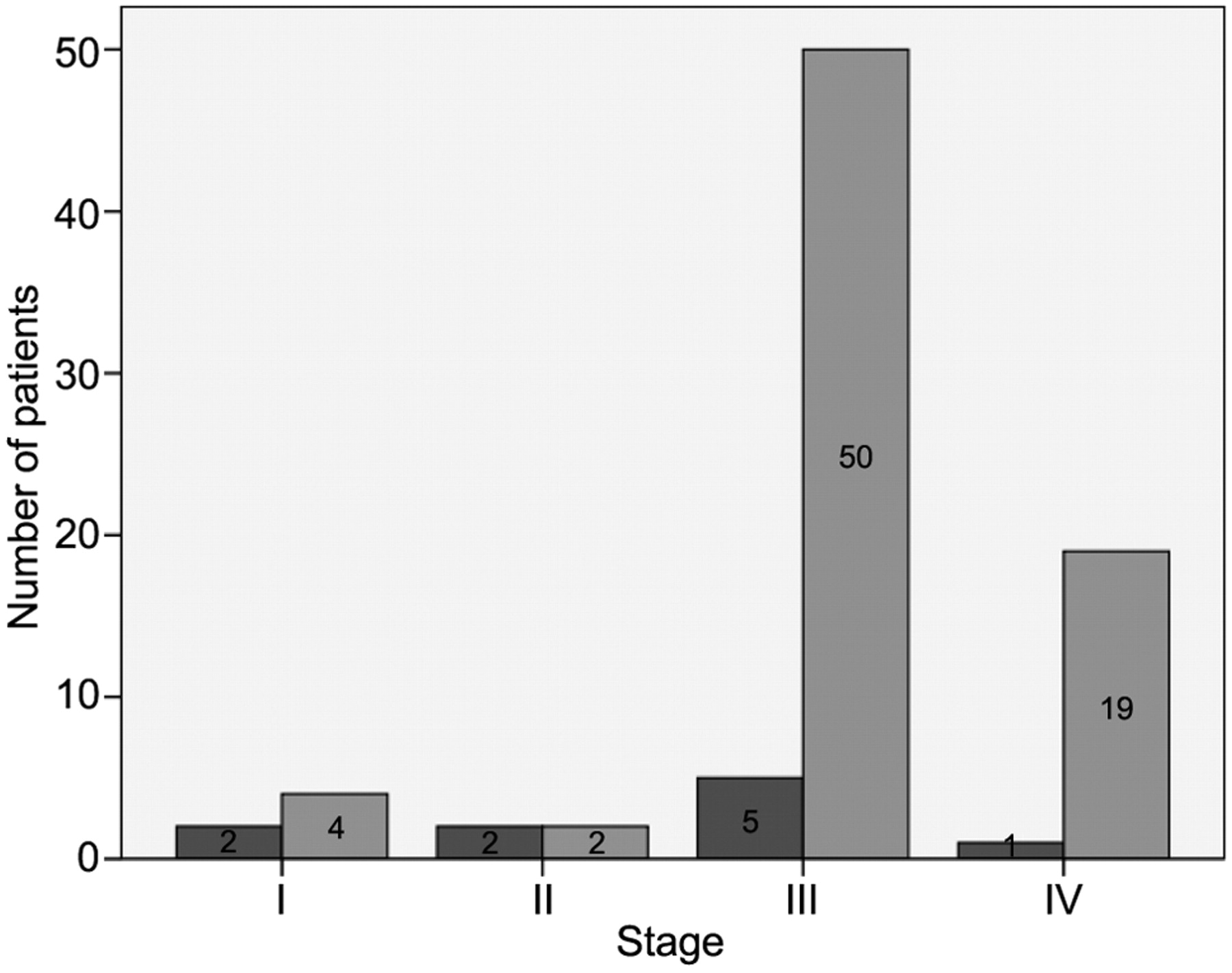
The difference between claudin-5 positive and claudin-5 negative samples was also significant according cancer stage (p=0.022) (Figure 3). Some 92% of the advanced stage (stage III and stage IV) and 60% of the early stage (stage I and stage II) carcinomas showed claudin-5 expression. Strong immunostaining, i.e. 50-100% of the cells positive, was found in 37% of the advanced stage and in 30% of the early stage carcinomas.
Claudin-5 immunostaining of serous ovarian cancer patients.
The median of preoperative CA-125 was 815 (16-14,754) IU/ml. There was no significant difference in CA-125 expression between the claudin-5-negative and claudin-5-positive samples.
The median relapse-free survival time was 12 months (relapse-free survival time was missing in 2 cases) and the median overall survival time was 30 months. The number of patients who died of serous ovarian cancer was 52 out of the 85 (61%). At the end of follow-up, 30 out of the 85 patients (35%) were alive. The median follow-up time was 30 (0-120) months. In the Kaplan-Meier survival analyses, claudin-5 positivity indicated shorter cancer-specific (p=0.032) and overall survival (p=0.026) than claudin negativity. Only 25-30% of the claudin-5-positive but 60% of the claudin-5-negative patients were alive at the 5-year follow-up (Figure 4). In the multivariate analysis, FIGO stage was the only prognostic variable remaining in the equation (p=0.021, Exp(B)=0.295 (0.104-0.835)).
Discussion
The expression of claudin-5 was high in the serous cancer tissues in the present study and a correlation between claudin-5 expression and grade, stage, cancer-specific survival and overall survival was found. The highest intensity of claudin-5 positive samples was detected in the high grade and advanced stage carcinomas. These results indicated that claudin-5 positivity was associated with aggressive behavior in serous ovarian carcinomas.
Claudins are tight junctional proteins. Other proteins located at tight junctions are occluding, junctional adhesion molecules (JAMs) and tight junctional proteins ZO1, ZO2 and ZO3. Claudin gene expression is frequently altered in various neoplasms (14, 15). In particular alterations have been found concerning claudin 1, 3, 4, 5, 7, 10 and 16. Most claudin proteins appear to be decreased in carcinomas, while claudin 3,4 and 7 are elevated in several malignancies such as those originating from the pancreas, bladder, thyroid, fallopian tubes, ovary, stomach, colon, breast, uterus and the prostate (6). Claudin-3 and claudin-4 have been found to be among the most highly overexpressed genes in ovarian serous papillary carcinoma (16). Compared with other soft tissue tumors, claudin-5 has been seen only in vascular tumors and thus it is a candidate as a marker of vascular differentiation (10). Claudin-5 can be used to differentiate adenomatoid tumors from vascular lesions.

Claudin-5 expression in a moderately-differentiated serous papillary adenocarcinoma of the ovary. Membrane-bound staining for claudin-5 can be seen in tumor cells. Notice also positive staining in blood vessels in the stromal compartment (a). Another case of a serous ovarian adenocarcinoma showing positivity for claudin-5 in tumor cells. Two psammomatous bodies can be seen in the tumor tissue (b).
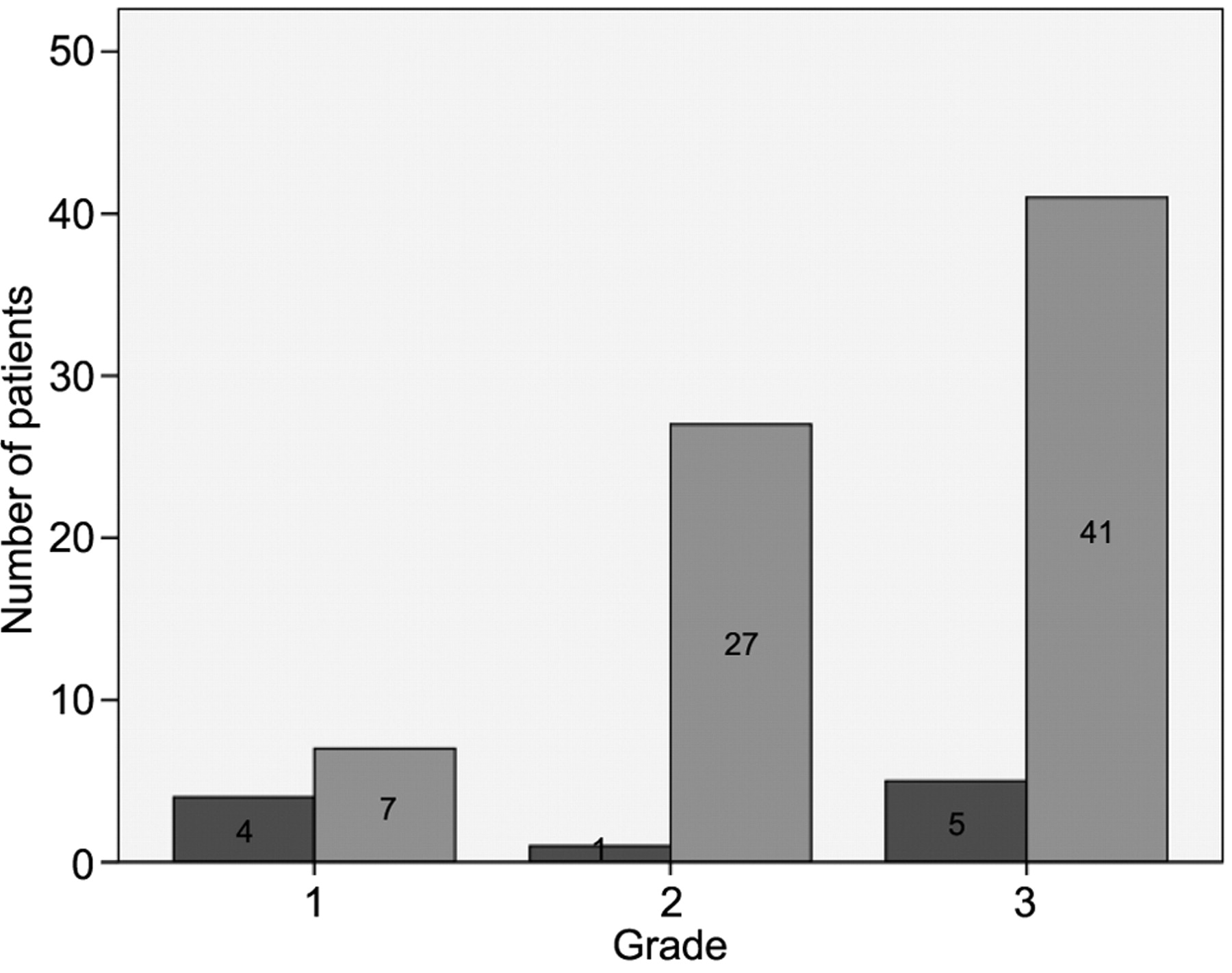
Claudin-5 expression in serous ovarian adenocarcinomas by grade ( claudin-5-negative,
claudin-5-negative,  claudin-5-positive).
claudin-5-positive).
The increased expression of claudin-5 seems likely to be involved in cancer behavior in ovarian serous adenocarcinomas. This may be due to the fact that claudin-5 is able to activate matrix metalloproteinases (MMP), such as MMP2 and MMP9 (17). Expression of MMPs has been found in ovarian cancer, and their activation has been associated with malignant behavior of the tumors and poor survival (18, 19). In agreement with this, claudin-5 overexpression correlated with advanced stage, high grade, cancer-specific survival and overall survival, which may have some clinical relevance. Claudins are cell membrane proteins and therefore may serve as potential targets for antibody-mediated cancer therapy. Serous ovarian cancer patients with claudin-5 positivity may need more aggressive treatment for the cancer than claudin-5 negative patients. If chemotherapy for claudin-5-positive serous ovarian carcinomas were combined with antibody-mediated claudin-5 suppressive treatment, survival might improve. Hewitt et al. (6) suggested claudin-5 as a new target for antiangiogenic therapy especially if compounds that cannot cross the blood-brain barrier were being used. Other studies suggested that claudins may be involved in the survival or invasion of different cancer cells. In serous ovarian adenocarcinomas, for instance, claudin-3 overexpression, using overall expression (both membrane-bound and cytoplasmic staining) can be used as a prognostic indicator. Patients with high claudin-3 expression had shorter survival compared to patients with low claudin-3 expression at 3-year follow-up (20).
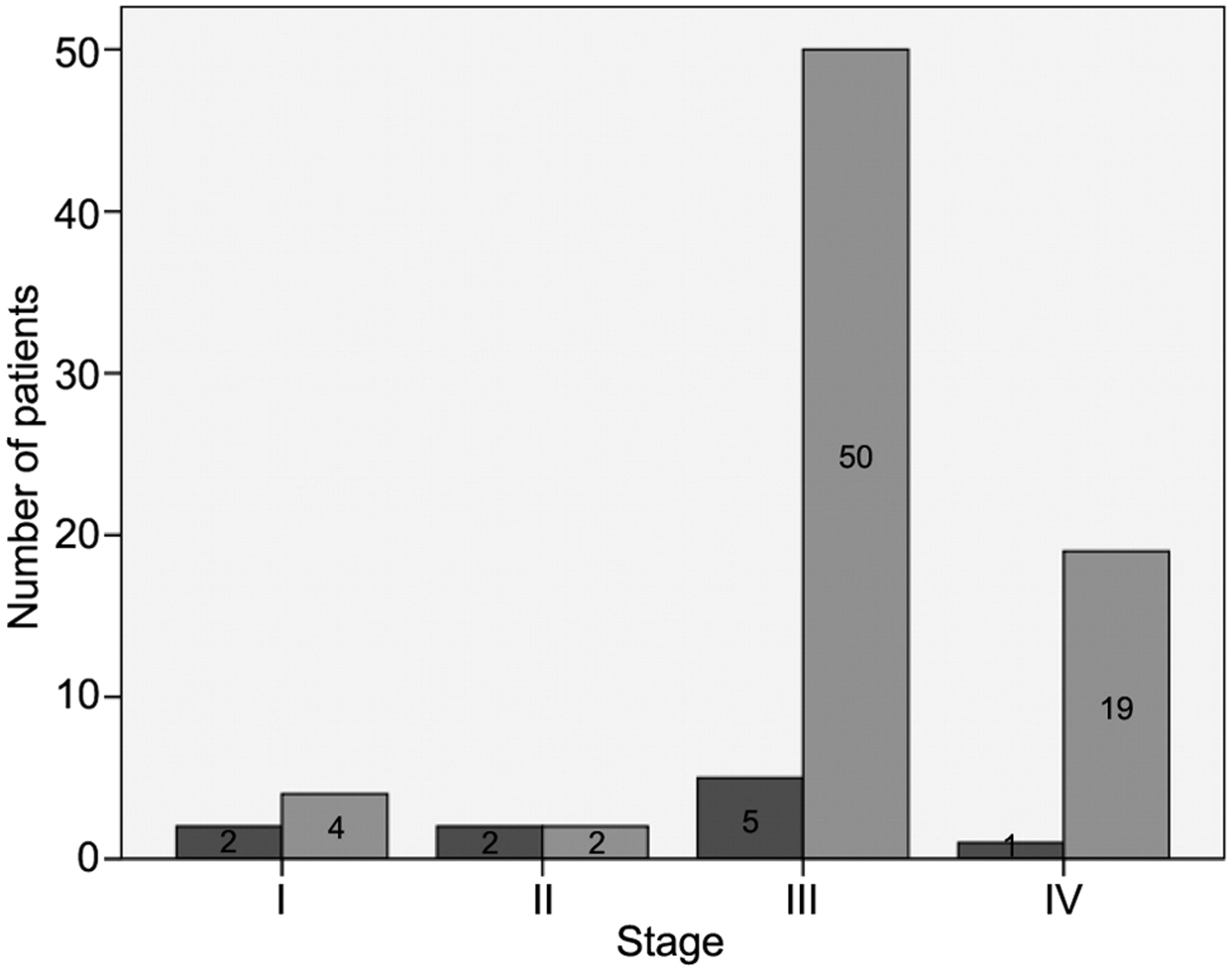
Claudin-5 expression in serous ovarian adenocarcinomas by stage ( claudin-5-negative,
claudin-5-negative,  claudin-5-positive).
claudin-5-positive).

Cancer-specific survival in serous ovarian carcinomas. Claudin-5-positive ovarian cancer patients had a shorter survival compared with claudin-5-negative patients (p=0.032).
In summary, claudin-5 positivity is associated with aggressive behavior of serous ovarian cancer and is associated with increased grade, advanced stage and poor survival of serous ovarian cancer patients. There is a need to further examine serous carcinomas with a larger number of patients and also other histopathological ovarian neoplasms. In the future, antibody-mediated claudin-5 suppressive treatment could be a new approach to cancer therapy.
- Received June 29, 2009.
- Revision received October 19, 2009.
- Accepted October 22, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}