


Abstract
There have been many discrepant observations on the serum levels of cytokines in cancer patients and their prognostic value. The purpose of this study was to determine the plasma levels of pro- and anti-inflammatory cytokines and their clinical significance in a large group of patients with gastric carcinoma. The levels of tumour necrosis factor alpha (TNF α), interleukin-12p40 (IL-12p40), IL-12p70, IL-18, IL-10 and soluble TNF receptors I and II sTNF-Rs were investigated in the plasma of 136 consecutive patients with biopsy proven gastric cancer using specific enzyme-linked immunoabsorbent assays (ELISA). Survival curves were estimated using the method of Kaplan and Meier and the differences in the survival rates were tested by the log-rank test. For multivariate analysis of prognostic factors, the Cox proportional hazard model was used. Proinflammatory cytokines and sTNF-Rs were higher in the whole group of patients in comparison to healthy volunteers. IL-10 was elevated mostly in advanced disease. The increased levels of IL-10 (>10 pg/ml) were associated with significantly poorer survival of patients, while the levels of the other cytokines and sTNF-Rs showed no correlation with prognosis. The increased level of IL-10 is an independent unfavorable prognostic factor in patients with gastric cancer.
Abbreviations: CEA: Carcino-embryonic antigen; ELISA: enzyme-linked immunoabsorbent assay; IL: interleukin; PBMC: peripheral blood mononuclear cells; sTNF-R: soluble tumour necrosis factor receptor; TNF: tumour necrosis factor.
It is generally assumed that the immune response in malignant disease is impaired and is thus associated with a poor prognosis. Clinically detectable dysfunction of the immune system is generally observed in cases of disseminated disease. Therefore research studies are focused on subclinical measurements of cell function, inflammatory mediators, cytokines and growth factors. There is no common pattern of the immune dysfunction observed. It probably depends on the tumour-host reaction, tumour site and stage of the disease.
Cytokines have been investigated in numerous studies as tumour markers, a prognostic tools for staging and survival and prognostic factors of postoperative complications. Proinflammatory cytokines were reported to play a role in cancer cachexia and metastasis promotion while antiinflammatory cytokines (interleukin (IL)-10, IL-4) have mainly been described as markers of more advanced disease (1-3).
It has been reported that the serum level of the proinflammatory cytokine IL-18 is elevated in patients with stage II and III gastric cancer and associated with poor survival (4). Significant discrepancies have been reported on the serum levels of proinflammatory cytokines in patients with cancer. Thus, in gastric cancer tumour necrosis factor (TNF) was elevated (>10 pg/ml) in 7.7 or 26.0% of patients in two different studies (5, 6) and it was neither related to the stage of disease nor prognosis, while in another study elevated levels of TNF were observed in advanced gastric cancer and were associated with a poor prognosis (7). On the other hand, low serum levels of IL-12 have been associated with more advanced stages of gastric and colorectal carcinomas and tended to be associated with lymph node metastasis and carcinoembryonic antigen (CEA) positive tumours greater than 5 cm in diameter, but this was based on a small group of patients (8). Another small study has indicated that elevated serum IL-12 was associated with prolonged survival of patients with metastatic lung and gastrointestinal cancer (9). Data concerning the level of anti-inflammatory cytokine IL-10 in gastric cancer patients display discrepancies. A study performed on 68 patients showed no correlation between serum IL-10 level and the clinical course of disease (10). On the other hand, the serum level of this cytokine did correlate with the progression of breast cancer (11). In an experimental model, high intraperitoneal concentrations of IL-10 prevented peritoneal dissemination of gastric cancer (12). Preoperative serum levels of IL-10 in patients with colon cancer have been shown to be useful markers for predicting both the likelihood of curative surgery being performed and, in combination with the 16th postoperative day serum levels, tumour recurrence (13).
These discrepant observations prompted the present systemic studies on the occurrence and clinical significance of proinflammatory (TNF, IL-12 and IL-18) and anti-inflammatory (IL-10) cytokines in the plasma of a large group of patients with different stages of gastric cancer.
Patients and Methods
Patients. A total of 136 consecutive patients with biopsy-proven gastric carcinoma treated at a single institution between 1997 and 2007 were investigated. All the patients underwent radical (n= 92) or palliative (n=44) gastric resection.
The postsurgical clinicopathological staging system of the International Union against Cancer (UICC) TNM Classification of Malignant Tumors (5th edition) was used for classification of the disease (14). The patient group consisted of 52 women and 84 men, with a mean age 61.5±11.9 years, range 28 to 83 years. At the time of final follow-up, 86 out of the 136 patients (63%) had died, and the median follow-up for the surviving individuals was 82.6 months. Table I shows the clinicopathological characteristics of the patients. Blood was taken preoperatively and plasma samples were stored at −80°C. The plasma levels of proinflammatory (TNF, IL-12p40, IL-12p70, and IL-18) and antiinflammatory (IL-10) cytokines were determined. None of the patients had received chemotherapy or radiotherapy before surgery and did not show clinical symptoms of inflammatory disorders. The Ethical Committee of the Jagiellonian University approved the study. Informed consent was obtained from the patients. The control group consisted of 42 healthy volunteers (M/F: 25/12, age: 46.5±12.8).
Determination of cytokine levels. Cytokine levels were determined by specific enzyme-linked immunoabsorbent assay (ELISA) using commercially available kits: TNF (EASIA Biosource, Nivelles, Belgium), IL-12p40, IL-12p70 and IL-10 (PharMingen, San Diego, CA, USA), IL-18 (MBL, Nagoya, Japan), soluble TNF receptor (sTNF-R) and R-II (R & D Systems, MN, USA). The cut-off levels of each assay were as follows: TNF: 15.6 pg/ml, IL-10, IL-12p40 and IL-12p70: 7.8 pg/ml; IL-18: 12.5 pg/ml, sTNF-RI and R-II −7.8 pg/ml.
Statistical analysis. The differences between the levels of cytokines in the patients groups were analysed using Student's t-test. All the quantitative variables were described as medians and their 95% confidence intervals (95% CI). The Mann—Whitney U-test and the Chi-square test, were used where appropriate to compare the distribution of individual variables between groups. Survival data were analyzed according to the Kaplan-Meier method and included postoperative mortality. The log-rank test was used to detect differences between groups in the univariate analysis of potential prognostic factors. Multivariate analysis was performed using a Cox proportional hazards model with a backward stepwise selection procedure. Variables in the Cox proportional hazards model included: age, degree of differentiation, tumour location, lymph node status, distant metastases, splenectomy and IL-10 level. Age, degree of differentiation, tumour localisation, and splenectomy were withdrawn using a backward stepwise selection procedure. The probability for entering the model was 0.05 and for removal from the model 0.100. A significance level (p) <0.05 was considered statistically significant. Statistical analysis was performed using the SPSS v.14 (SPSS Inc., Chicago, IL, USA) software package and GraphPad Prism (San Diego, CA, USA) software.
Demographical and clinicopathological characteristics of patients with gastric cancer.
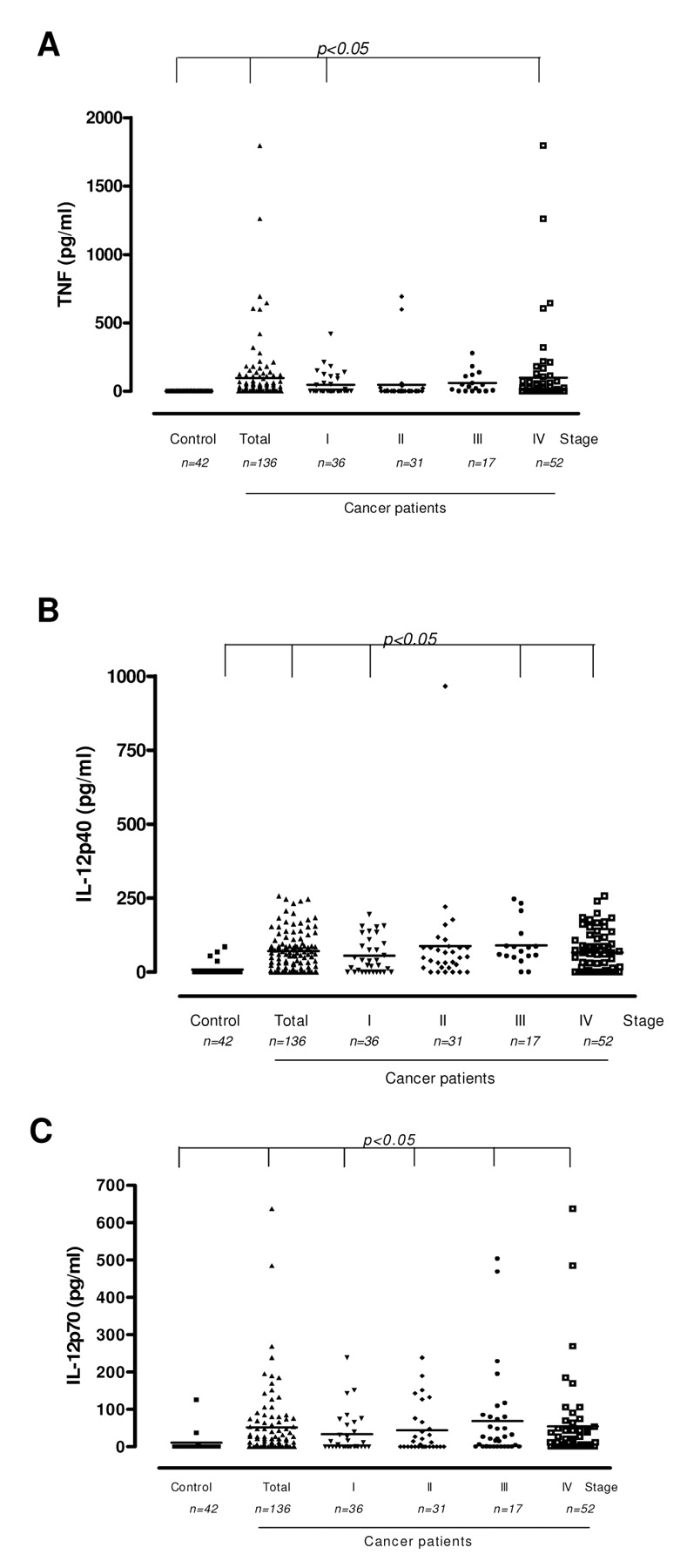
Preoperative plasma levels of TNF (A), IL-12p40 (B) and IL-12p70 (C) in patients with gastric cancer. P<0.05 compared to control.
Results
Cytokine levels in plasma of patients with gastric cancer. TNF was detected in 52% of the patients and, in comparison to the control group, its level was significantly higher in the whole patient group and in stage I and IV the disease. There were no significant differences in the mean levels between the stages (Figure 1A). IL-12p40 and IL-12p70 were significantly elevated in all the stages (Figure 1B and 1C). IL-18 was elevated in the whole group of patients and in stages II and IV compared to the control (Figure 2A). IL-10 was significantly elevated in the whole group of patients compared to the control mostly due to an increase observed in stage IV disease (Figure 2B). Apparently, there was no clear association of the elevated levels of any of the studied cytokines with the histopathological type of tumour according to Lauren's classification (data not shown). Subanalysis of the cytokine levels with other prognostic factors revealed significantly higher levels of TNF and IL-18 in N patients with N(−) vs. N(+) status, while IL-12p40 was elevated in those with T1/2 vs. T3/4 tumours. There was no association of IL-10 mean levels with T, N or M status (Table II).
Pathological parameters of the tumour and cytokine levels.
The levels of sTNF-RI and R-II were also determined in 60 randomly chosen cancer patients. Both sTNF-Rs were significantly higher in the total group of patients and in the patients with stage III and IV disease (Figure 3). The sTNF-RI and R-II increase was associated with tumour depth and N status (Table III). Regression analysis revealed no correlation between the levels of sTNF-Rs and TNF (data not shown).
The impact of increased plasma levels of cytokines on prognosis. Univariate analysis of prognostic factors in this group of patients revealed that T, N, M status, radicality of resection, splenectomy and the level of IL-10 had a significant influence on survival. No such relationship was observed for the level of proinflammatory cytokines and sTNF-Rs (data not shown). Multivariate analysis performed on the set of factors selected via the univariate method confirmed that a level of IL-10> 10 pg/ml was an independent prognostic factor (Table IV).
When the clinicopathological variables of the groups of patients with IL-10 levels above and below the cut-off point were compared, no significant differences were found (Table V). The cumulative survival of these two groups of patients (Figure 4) indicated that the 5-year survival of patients with preoperative elevated levels of IL-10 was significantly shorter (p<0.002). This was also true when the survival of patients without distant metastasis (n=122) was analysed (data not shown).

Preoperative plasma levels of IL-18 (A) and IL-10 (B) in patients with gastric cancer. P<0.05 compared to control.
Discussion
The present study showed that proinflammatory cytokine levels increased in the plasma of some gastric cancer patients. TNF was significantly increased in 52% patients with gastric cancer in comparison to healthy volunteers, but no clear association with the stage of disease was observed. Increased values of TNF were also found in patients with colorectal cancer (15), hepatocellular carcinoma and metastatic liver carcinoma (16, 17). On the other hand, TNF was undetectable in the serum of patients with metastatic breast carcinoma (18) and patients with gastrointestinal cancer-associated cachexia (19-21). The present data showed that TNF was higher in stages I and IV of the disease. These observations taken together may suggest that TNF has no role in cancer-related cachexia in man, at least in some types of cancer, but may play a significant role in the regulation of the inflammatory host response to the growing tumour (22) which is in keeping with our previous observations (21, 23).
Pathological parameters of the tumour according to sTNF-RI and R-II levels.
Multivariate analysis of prognostic factors for survival (Cox proportional hazard model).
Demographical and clinicopathological characteristics of patients with gastric cancer according to level of IL-10.
It appears that TNF is produced mainly by peripheral blood mononuclear cells (PBMCs), but not locally, in the primary tumour or in the regional lymph nodes of gastric cancer patients (5). Our previous observations indicated that PBMCs isolated from gastric cancer patients do not release TNF spontaneously in vitro, however they do produce TNF, IL-12p40 and IL-10 upon stimulation with cancer cells (24). Under such circumstances monocytes are the main source of cytokines and the question arises as to whether tumour infiltrating macrophages (TIM) may be responsible for the production of these cytokines. Abundant TNF mRNA was demonstrated in TIM infiltrating colorectal cancer (25). However, TIM may produce TNF in some, but not other, types of tumours (26). Elevated serum levels of sTNF-RI and R-II were observed in ovarian, endometrial and cervical carcinomas, and correlated with worse clinical outcome (27-29). Serum levels of sTNF-RI were also elevated in gastric cancer, especially in patients with stage IV disease with cachexia (30). However, in other studies, low serum levels of sTNF-RII in cervical cancer were detected and seemed to be a poor prognostic factor (31). In the present investigations, circulating sTNF-Rs were increased mostly in advanced gastric cancer (stages III and IV). However, they were not related to prognosis and showed no reverse correlation with TNF levels. The meaning of these findings is unclear as TNF is biologically active when bound to sTNF-Rs (32).

Plasma levels of sTNF-RI and R-II in patients with gastric cancer. P<0.05 compared to control.
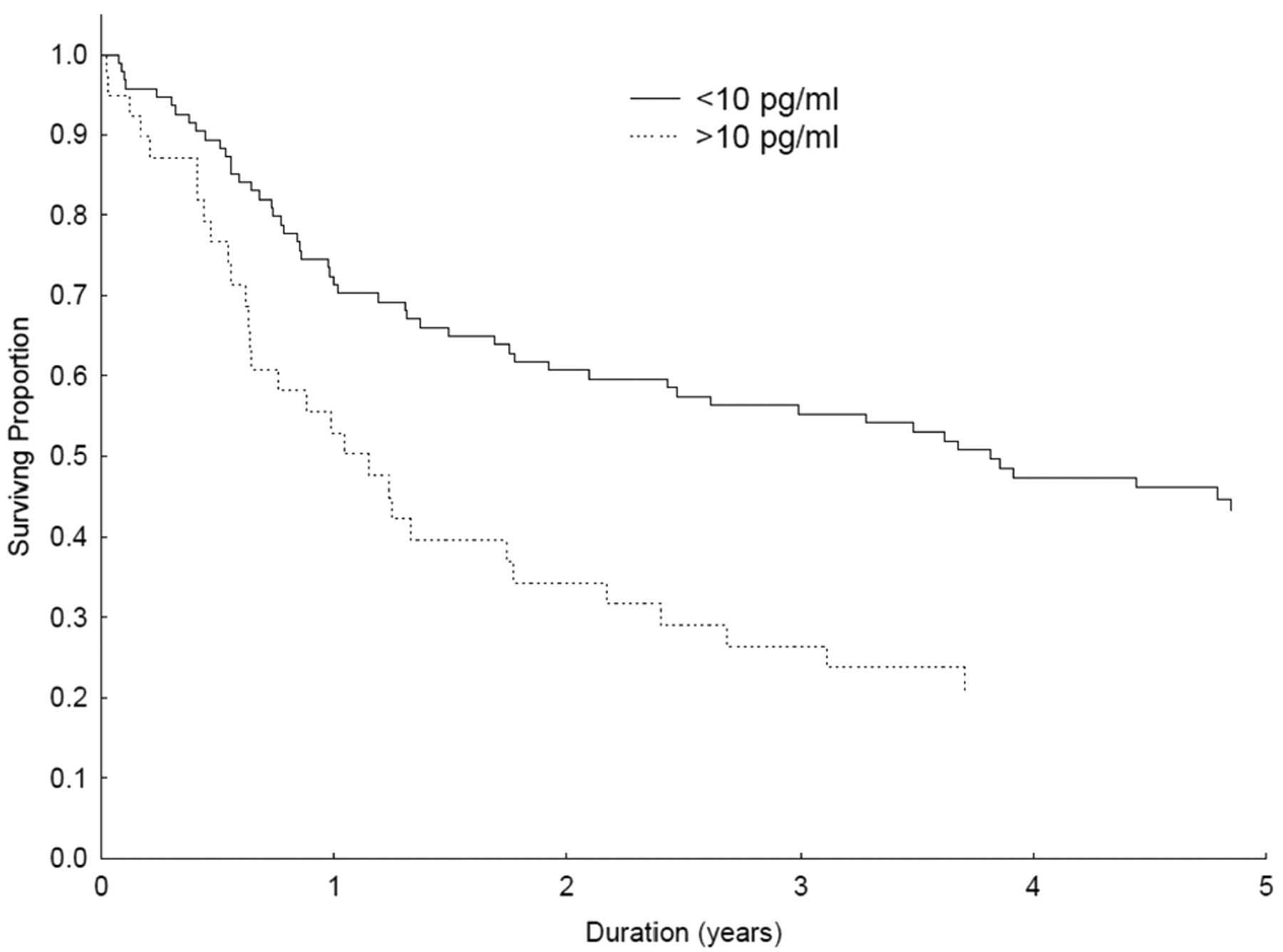
Survival curves of patients with gastric cancer, in relation to plasma level of IL-10.
In contrast to other studies, the present results clearly indicated increased levels of IL-12p40 and bioactive IL-12p70 in the plasma of the patients in all stages of gastric cancer. Elevated IL-18 was observed mainly in stages II and III, but less in stage IV gastric cancer (22) and in bladder cancer and interestingly more in Ta than T1-T4 and in G1 than G2/3 tumours (33). The present findings showed increased levels of IL-18 in the whole group of patients and in stages II and IV.
Elevated serum levels of IL-10 in patients with resectable hepatocellular carcinoma and advanced gastrointestinal malignances were observed and appeared to be an independent adverse prognostic factor (34, 35). Elevated concentrations of IL-10 in the ascitic fluid of gastric cancer patients also correlated with an unfavorable outcome (36), but a lack of differences in the production of IL-10 by PBMCs of gastric cancer patients of different clinical stages were observed (24, 37). The present study showed elevated plasma IL-10 in the patients and overall in stage IV, but no clear association with other clinicopathological parameters (TNM).
Observations on the association of serum levels of different cytokines and prognosis in cancer patients are also contradictory. As elevated TNF was associated with disease progression and malnutrition in hepatocellular carcinoma, it was assumed to be a poor prognostic indicator (17, 19). However, the present data on gastric cancer do not support this conclusion as the increased plasma TNF had no association with survival. Apparently, the same was also true for IL-12p40, which is not in keeping with the observation of Lissoni et al. that high IL-12 levels (unspecified form) were associated with longer survival in patients with different types of solid tumours (9). As far as IL-18 is concerned, the present observations differ from the report of Kawabata et al. (4) showing that preoperatively increased IL-18 was a poor prognostic marker in patients with gastric cancer. In the present study, IL-18 levels were not associated with prognosis.
The only association of cytokine level with prognosis in the present study was the significantly shortened overall survival of the patients with elevated IL-10. This was in keeping with observations that serum IL-10 is an adverse prognostic factor in patients with different types of advanced solid tumours (34) and in unresectable hepatocellular carcinoma (35), but in contrast to other recent data showing no impact on the clinical course of gastric cancer (10). The present data, based on a large group of gastric cancer patients indicated that increased plasma IL-10 was associated with significantly shortened 5-year survival. However, the very recent report of Ikeguchi et al. (38) shows that a high levels of serum IL-10 is associated with a worse prognosis in gastric cancer patients, which is in keeping with present data.
In summary, proinflammatory cytokines (TNF, IL-12, IL-18) are increased in the plasma of about half of gastric cancer patients but show no association with prognosis. Among the cytokines only immunosuppressive IL-10 has an influence on prognosis, its elevation is associated with shortened survival and it is an independent prognostic factor.
Acknowledgements
This work was supported by a grant from the State Committee for Scientific Research (grant no. 091/P05/2003/53 and grant no. 3 P05C 032 22, 2P05C 001 29).
- Received May 13, 2009.
- Revision received November 2, 2009.
- Accepted November 11, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}