


Abstract
Cancer and chronic fatigue syndrome (CFS) are both characterised by fatigue and severe disability. Besides fatigue, certain aspects of immune dysfunctions appear to be present in both illnesses. In this regard, a literature review of overlapping immune dysfunctions in CFS and cancer is provided. Special emphasis is given to the relationship between immune dysfunctions and fatigue. Abnormalities in ribonuclease (RNase) L and hyperactivation of nuclear factor kappa beta (NF-κB) are present in CFS and in prostate cancer. Malfunctioning of natural killer (NK) cells has long been recognised as an important factor in the development and reoccurrence of cancer, and has been documented repeatedly in CFS patients. The dysregulation of the RNase L pathway, hyperactive NF-κB leading to disturbed apoptotic mechanisms and oxidative stress or excessive nitric oxide, and low NK activity may play a role in the two diseases and in the physiopathology of the common symptom fatigue. However, in cancer the relation between the immune dysfunctions and fatigue has been poorly studied. Immunological abnormalities to such as a dysregulated RNase L pathway, hyperactive NF-κB, increased oxidative stress and reduced NK cytotoxicity, among others, are present in both diseases. These anomalies may be part of the physiopathology of some of the common complaints, such as fatigue. Further studies to confirm the hypotheses given here are warranted.
- Fatigue
- RNase L
- nitric oxide
- protein kinase R
- nuclear factor kappa beta
- NF-κB
- intracellular immune dysfunction
- natural killer cell
- oxidative stress
- exercise
- review
Cancer and chronic fatigue syndrome (CFS) are both characterised by fatigue and severe disability. Fatigue is the hallmark of CFS, and is also a common symptom experienced during and after treatment for cancer. Fatigue may not be the only link between the two pathologies. A body of literature describing immune abnormalities in both cancer and CFS is currently available. Comparing the two pathologies might result in more insight into the nature of common complaints such as fatigue. Therefore, the two diseases are here set side by side regarding fatigue and immune dysfunctions. An in-depth review of the scientific literature fuels the comparison of immune dysfunctions in cancer and CFS. In the discussion, the hypothesized relation between fatigue and immune dysfunctions is presented and discussed in relation to the available evidence.
Fatigue
Chronic fatigue syndrome. The most commonly used diagnostic criteria and definition of CFS for research and clinical purposes were published by the United States Centers for Disease Control and Prevention (CDCP). The CDCP definition of CFS requires two criteria be fulfilled (1): i. A new onset (not lifelong) of unexplained, persistent fatigue unrelated to exertion and not substantially relieved by rest, which causes a significant reduction in previous activity levels. ii. Four or more of the following symptoms that last six months or longer: impaired memory or concentration; post-exertional malaise, where physical or mental exertions bring on “extreme, prolonged exhaustion and sickness”; unrefreshing sleep; muscle pain; pain in multiple joints; headaches of a new kind or greater severity; sore throat; tender lymph nodes (cervical or axillary).
When symptoms are attributable to other conditions, the diagnosis of CFS is excluded. The CDCP specifically refers to several illnesses with symptoms resembling those of CFS (1), for example primary sleep disorders, severe obesity, major depressive disorders or cancer. The fatigue in CFS is very disabling, causing substantial reductions in premorbid activity levels, unexplained and not improved by rest (1). The cause may yet not be clear, but fatigue is the hallmark of CFS. Several hypotheses as to the cause of the fatigue have been proposed in the literature. Most rely on a biopsychosocial model with possible contributing factors such as neuroendocrine abnormalities, neuropsychological dysfunctions, autonomic dysregulations, environmental factors, psychological processes and personality traits, abnormal exercise response, overactive or passive lifestyle, infections and immune dysfunctions. Many reviews are available on these possible contributing or predisposing factors. But then again, CFS, with the hallmark fatigue, can only be diagnosed in the absence of a clear medical cause for the fatigue.
Cancer patients. Although fatigue arouses less interest in cancer, it is one of the most common side-effects of cancer and its treatment. The fact that less emphasis is put on fatigue in cancer than in CFS may be explained by the presence of other underlying symptoms and the high mortality rates of cancer. Doctors are still struggling with high mortality rates for cancer and therefore survival would be the main treatment objective, regardless of possible side-effects.
Most of the research on fatigue in people with cancer has been conducted on samples of people undergoing cancer treatment. Cancer-related fatigue is reported by 60% to 99% of cancer patients and has been described as one of the most significant quality-of-life issues in cancer care (see for example 2, 3-8). The fatigue experienced as a side-effect of cancer treatment differs from the fatigue experienced by healthy people in their daily lives. Cancer patients describe their fatigue as chronic, more severe, intense, energy draining, unrelenting, and rapid in onset (9).
Over the past decade, the medical community has recognised fatigue as a debilitating symptom also in people who have been treated successfully for cancer. Between 19% and 39% of cancer survivors experience severe fatigue up to 9 years after cancer treatment has terminated and long after they were categorised as ‘cured’ of cancer (10-12). There is evidence that fatigue significantly affects the quality of life of cancer survivors. The experience of fatigue in cancer survivors is quite similar to the experience of patients with CFS in the general medical setting. The fatigue is often accompanied by other symptoms such as concentration difficulties, emotional problems, functional restrictions and reduced physical activity (13). Clinical experience seems to suggest that fatigue complaints continue to decrease during the first 3-4 years after curative treatment. For about a quarter of cancer survivors, fatigue remains a continuous problem, with detrimental consequences on the functional status and quality of life (10, 14).
While the exact cause of the fatigue in CFS remains unclear, several contributing factors have been identified in (post-)cancer fatigue. Some of these are typical for cancer patients or survivors, other are also applicable to other chronic syndromes, such as CFS. The contributing factors are extensively reviewed and can be categorized as treatment-related, disease-related, physical symptoms, psychological symptoms and coping strategies (4, 5, 15).
Treatment-related factors. The association of fatigue with the major cancer treatment modalities of surgery, chemotherapy, radiation therapy and biological response-modifying therapy fuelled the speculation that fatigue resulted from tissue damage or accumulation of products of cell death (16). Nevertheless, different studies have refuted this hypothesis because they were unable to find associations between fatigue severity and length, dosage or type of treatment (e.g. 11-13).
Moreover some side-effects of therapy, such as nausea and vomiting, can trigger fatigue (17, 18). In addition, concurrent medications such as analgesics, hypnotics, antidepressants and steroids may sedate the central nervous system, contributing to the problem of fatigue.
Disease-related factors and physical symptoms. Evidence suggests that anaemia (related to the disease itself or the therapy) may be a major factor in cancer-related fatigue (CRF) and quality of life in cancer patients (6), while anaemia cannot be retained as an etiological factor in the fatigue of CFS.
Besides anaemia, several metabolic and endocrine alterations may cause fatigue. Malnutrition is particularly identified as an important factor contributing to fatigue by causing an imbalance between energy supply and energy requirements. Malnutrition may be the consequence of alteration in the body's ability to process nutrients efficiently (impaired metabolism), an increase in the body's energy requirements (tumour consumption, infections, fever, etc.) and a decrease in intake of energy sources (anorexia, vomiting, etc.). In advanced cancer, cachexia often occurs. This is a pathological state characterized by anorexia and metabolic abnormalities such as glucose intolerance, fat depletion and muscle protein catabolism, generating a high degree of energetic inefficiency that results in early satiety, impaired immune response, weight loss, fatigue and a considerable loss of muscle and, therefore, asthenia among others (19). Insomnia and inactivity are also mentioned as possible contributing factors (5). The literature is not consistent regarding the influence of tumour stage, size or type (e.g. reviewed in 4, 15).
Psychological symptoms and coping strategies. The diagnosis of cancer, the often demolishing treatment and the life-threatening situation unavoidably bring along fears, doubts, depression, negative self-efficacy (self-efficacy is the belief that one is capable of performing in a certain manner to attain certain goals), distress, problems with accepting etc. Emotional vulnerability and the endurance of heavy stress over prolonged periods of time may trigger fatigue. In several studies, the intensity of fatigue showed a strong correlation with indicators of psychological distress such as depression, somatization, catastrophizing and anxiety (e.g. 10, 20-23). Coping strategies are also related to fatigue levels (12, 20).
The latter category of contributing factors could also hold true for CFS patients. CFS patients and cancer patients or survivors seem to differ on, for example, self-efficacy (13), CFS patients tend to focus more on their fatigue and experience fatigue more negatively. A possible explanation may be the fact that for CFS patients there is no distinct cause, while cancer patients tend to attribute their fatigue to their specific disease.
While treatment-related factors are fairly specific for cancer patients, some of the disease-related factors are also applicable to CFS patients. For example, physical inactivity (24, 25) and pain (26, 27) are frequently reported in CFS patients and could also be related to their fatigue. However, of all the body systems affected by cancer and CFS, the immune system has shown the most important and partly overlapping changes in both illnesses.
Intracellular Immunity: Ribonuclease L (RNase L)
CFS patients. One of the major intracellular immune dysfunctions in CFS is the dysregulation of the RNase L antiviral pathway. RNase L is the effector of the major 2-5-oligoadenylate synthetase/ribonuclease L (2-5A/RNase L) antiviral system. It is one of the intracellular proteins activated by type I interferons (IFN) and is cardinal to the cellular defence mechanisms. By regulating viral and cellular RNA expression, RNase L plays an important role in the antiviral and antiproliferative activities of IFN and contributes to innate immunity and cell metabolism. Activation of the endoribonuclease RNase L produces small RNA cleavage products not only from viral RNA but from self-RNA as well. In consequence, the 2-5A/RNase L pathway is implicated in mediating apoptosis in response to viral infections and to several types of external stimuli. The effects of the 2-5A synthetase/RNase L pathway extend beyond initially infected cells to support a broader antiviral state in the organism (28, 29).
After its discovery by Suhadolnik and colleagues (30, 31), hyperactivation of the 2-5 A synthetase/RNase L antiviral pathway and the abnormal low molecular weight (LMW) RNase L (37 kDa) in a subset of CFS patients has been reported at length in the scientific literature (e.g. 32, 33-35).
The LMW RNase L hydrolyses RNA three times faster than the native RNase L (36). Moreover, the 37 kDa RNase L binds its activator, 2-5A, with an affinity six-fold tighter than does the 83 kDa RNase L. The higher affinity of LMW RNase L for 2-5A suggests that LMW RNase L is activated preferentially over the HMW RNase L and thus contributes more than the 83 kDa RNase L to the up regulated RNase L activity (32). In consequence, the LMW RNase L fragments in CFS patients are responsible for the uncontrolled degradation of ribosomal and mitochondrial RNA, leading to apoptosis. Apoptosis triggers the production of elastase and calpain (37), which are, in turn, considered to be responsible for the proteolytic cleavage of a number of structurally and functionally vital proteins, including the authentic RNase L (35), leading to an apoptopic vicious circle (37). In addition, the LMW RNase L may disturb proper ion flux through cell membranes by binding to the ion channels. The subsequent channelopathy causes inefficient ion transport, possibly leading to several of the CFS symptoms (38).
The LMW RNase L variant is specific for CFS and even considered as a potential biological marker, since the presence of the 37 kDa RNase L in extracts of peripheral blood mononuclear cells may distinguish patients with CFS from healthy individuals and those suffering from other diseases (39). But in cancer patients, abnormalities in the RNase L pathway are also documented.
Cancer patients. Besides antiviral activity, RNase L has been suggested to function as a tumour suppressor based on its roles in mediating apoptosis and antiproliferative activity of IFN (40). RNase L is able to inhibit tumour formation/growth in vivo (41, 42).
In addition, the evidence of a tumour suppressor function of RNase L has emerged from studies on the genetics of hereditary prostate cancer (HPC). HPC genetics is complex with many genes proposed as susceptibility factors in this syndrome, among them the RNASEL gene. Several variants in these genes have been observed among HPC cases (reviewed in 40).
The R462Q variant of RNASEL, having about 3-fold reduced catalytic activity in vitro, is the most prevalent genetic marker for prostate cancer. RNase L may directly or at least indirectly suppress one or more steps in prostate tumourigenesis and/or metastasis (40). The RNase L(R462Q) is deficient in causing apoptosis in response to 2-5A, consistent with its possible role in prostate cancer development. RNASEL mutations and some variants allow tumour cells to escape a potent apoptotic pathway (43). Individuals heterozygous for these mutations exhibit a 150% increased risk of prostate cancer, and homozygotes have a greater than double risk, underscoring the importance of inactivating RNASEL in the aetiology of prostate cancer (44, 45). The association of mutations in RNASEL with prostate cancer cases further suggests a relationship between innate immunity and tumour suppression. It is proposed here that RNase L functions in counteracting prostate cancer by virtue of its ability to degrade RNA, thus initiating a cellular stress response that leads to apoptosis (40).
It remains to be seen if mutated RNASEL predisposes to any other forms of cancer. Bartsch and colleagues (46) showed that the RNASEL R462Q variant might be associated with an increased risk for sporadic pancreas cancer and with more aggressive tumours in familial pancreatic cancer. Furthermore, the occurrence of elevated levels of RNase L seems to be an early event in colorectal tumourigenesis, suggesting that control of RNA turnover is an important step in tumour progression (47).
Intracellular Immunity: Nuclear Factor Kappa Beta (NF-κB)
Besides activating the RNase L system, IFN also activates another intracellular double-stranded RNA-detecting system, namely protein kinase R (PKR). PKR will, once activated, stimulate nuclear factor kappa beta (NF-κB), a group of transcriptional regulators which modulate cellular responses to environmental stimuli and cytokines. NF-κB is the major upstream, intracellular mechanism which regulates inflammatory and oxidative stress mediators. NF-κB would, for instance, trigger inducible nitric oxide synthetase expression. Inducible nitric oxide synthetase generates increased production of nitric oxide (NO) by monocytes/macrophages (48, 49).
CFS patients. NF-κB, as well as inducible nitric oxide synthetase and NO have been shown to be increased in CFS (50-52). The production of NF-κB is significantly correlated to the severity of illness and symptoms, such as fatigue and pain. These correlations suggest that the symptoms of CFS, such as fatigue, pain, muscular tension and depressive symptoms reflect a genuine inflammatory response in those patients (50).
The produced NO, in turn, has an immunological function: it is cytotoxic by inhibiting the mitochondrial electron transport and the DNA synthesis and by influencing iron metabolism (important for the proliferation of viruses) (49, 53). Excessive or persistent NO production as reported in CFS (52), is, however, detrimental for physiological functions, as explained in earlier studies on intracellular immune dysfunctions in CFS (34, 54, 55).
Cancer patients. Aberrant activation of NF-κB has been observed in many cancer types (56-58). NF-κB activation occurs in cells (premalignant cells) that are destined to undergo malignant conversion and in cells (microenvironment cells) that are recruited to the tumour microenvironment and produce cytokines, growth and angiogenic factors, and proteases that degrade the extracellular matrix to support cancer development and progression (59).
Many reviews have already focused on the relation between NF-κB activation and the carcinogenesis process, as well as tumour progression and metastatogenesis (e.g. 57, 60, 61). Based on the evidence describing the role of NF-κB, it is evident that NF-κB plays a pivotal role in suppression of apoptosis, promotion of cell proliferation and inflammation, and is closely associated with cancer development (61).
Cellular Immunity: Natural Killer Cell Functioning
Natural killer (NK) cells are an important part of the non-specific immune system. Malfunctioning of NK cells (i.e. decreased NK cell cytotoxicity) has long been recognised as an important factor in the development and reoccurrence of cancer (62), and has been documented repeatedly in people with CFS (63).
CFS patients. Concerning the number of NK cells in CFS patients, the literature is inconsistent. Some authors report decreased numbers (64), some approximately normal (65). About the activity or cytotoxicity of the NK cells there is less controversy: the cytotoxicity is reduced in a subgroup of patients (62, 65). In the study of Whiteside and Friburg (62), 25% of the CFS patients presented lower NK activity, although the quantity of cells was not different from healthy individuals. Curiously, the low NK syndrome itself is characterized by an uncomfortable chronic fatigue, malaise and reduced interest in physical or mental activities. In addition, long-lasting low-grade fever is often reported and most of the sufferers are disabled or even bedridden. These symptoms are almost identical to those associated with CFS (66). Observations suggest that individuals with chronically low NK activity may be genetically predisposed to the development of CFS (65).
Cancer patients. Natural cytotoxic receptors (e.g. NKp46, NKp44, NKp30) are displayed on the surface of NK cells and trigger NK cytotoxicity against tumour cells (67). Tumour cells appear continuously, but in healthy people they are cleared by NK cells. This is accomplished by perforins, stored in the cytoplasm of NK cells and capable of destroying the cell membrane of tumour cells (67). Alternatively, activated NK cells produce tumour necrosis factor α, which in turn initiates tumour cell apoptosis (68). In families with cancer, particularly with familial melanoma or breast cancer, low NK activity has been observed in family members with no evidence of cancer (69-71), suggesting that the low NK activity may be evidence of susceptibility to a future malignancy. The decreased cytotoxicity of the NK cells is directly related to the development and the reoccurrence of cancer (62), since NK cells act antitumourally.
Fatigue and immune dysfunctions observed in chronic fatigue syndrome and cancer patients.
The exact cause of the decreased NK activity is however unclear. It has been hypothesised that basically there could be a genetic predisposition. Observations suggest that individuals with chronically low NK activity may be genetically predisposed to the development of CFS (65) and might also be prone to the development of malignancy. These studies suggest that genetically determined defects in NK activity may contribute to the initiation of human cancer (72) and perhaps even of CFS. In general, the level of NK activity is a stable individual trait, which fluctuates within a low, middle, or high normal range characteristic for each individual. Therefore it is not surprising that both CFS and cancer often occur in the same family (65).
Besides genetic predisposition, and RNase L dysregulation (38), low NK activity could be the result of impaired NO-mediated activation of NK cells in CFS patients (50). It is known that more NO is released in the peripheral circulation of CFS patients and NO itself is known to be toxic to NK cells (73). NO is also suggested as having both a dual pro- and antitumour action within the multistage model of carcinogenesis (74, 75). Serum NO levels were found to be much higher in lung cancer patients (76) and since serum NO levels tend to increase further after chemotherapy (77), NO might play an important role in the impaired NK activity in cancer patients too. NO is also related to the prognosis of cancer patients (76).
Physical activity (i.e. aerobic exercise) is known to have positive effects on the number and cytotoxicity of natural killer cells in healthy humans (78-80), but this interaction is currently unexplored in people with cancer or CFS. Exercise triggers the release of pro-inflammatory cytokines (e.g. interleukin-1β and tumour necrosis factor-α), which in turn activate NK cells (80). In addition, catecholamines such as epinephrine are released during exercise and are capable of stimulating NK cells: NK cells display a high density of β2-adrenergic receptors capable of binding epinephrine (79). Still, the exact mechanisms as to how exercise alters immune function remain to be revealed (79), but this line of thinking may also be interesting since both patient groups are less active than healthy controls, as mentioned above.
Finally, increased oxidative stress, apparent in CFS patients (as reviewed in 81) and also in cancer survivors due to the aftercare (82), can reduce NK cytotoxicity (reviewed in 83) and cause fatigue (82).
Before discussing the link between the fatigue and the immune dysfunctions in both diseases, an overview of the immune dysfunctions observed in (subsets of) cancer patients and CFS patients is given in Table I.
Fatigue and Immunity
The question remains as to whether the immune dysfunctions observed could be related to the fatigue experienced in both diseases.
CFS patients. In CFS patients, RNase L dysfunctions already seem related to self-reported measures of physical functioning and to exercise capacity (55, 84-86). Physical functioning and exercise capacity can be seen as a physical component of fatigue. In addition, RNase L cleavage is weakly correlated to the Multidimensional Fatigue Inventory score (87). Furthermore, it is hypothesized that the channelopathy caused by LMW RNase L could be responsible for fatigue due to abnormal ion flux throughout cell membranes. Depending on the type of channel that is dysregulated, the transport of potassium, calcium, sodium, magnesium, etc. could become dysregulated, leading to central fatigue, sympathetic hyperactivity, muscle weakness, reduced aerobic power, sleep disturbances, etc. (38).

Relation between immune dysfunctions and fatigue.
The low NK syndrome, as observed in a subset of CFS patients, is characterized by a triad of symptoms, namely fatigue, malaise and reduced interest in physical or mental activities (66). In the study of Siegel et al. (63), 65.7% of the included CFS patients were actually correctly be classified as CFS patients with normal NK activity or CFS patients with reduced NK activity based on vigour and fatigue severity scores. These authors hypothesize that the fatigue may be the consequence of a chronic inflammatory response due to reduced NK activity.
Concerning the role of NF-κB in the fatigue of CFS patients, we already mentioned the study of Maes et al. (50) in which significant positive correlations were observed between the production of NF-κB and the severity of illness as measured with the FibroFatigue scale and with symptoms such as aches and pain, muscular tension, fatigue, irritability, sadness, and the subjective feeling of infection. Furthermore, the subsequent excessive NO production would also be related to fatigue (51). Excessive NO could lead to fatigue by disturbing iron metabolism (88), mitochondrial respiration (89), etc.
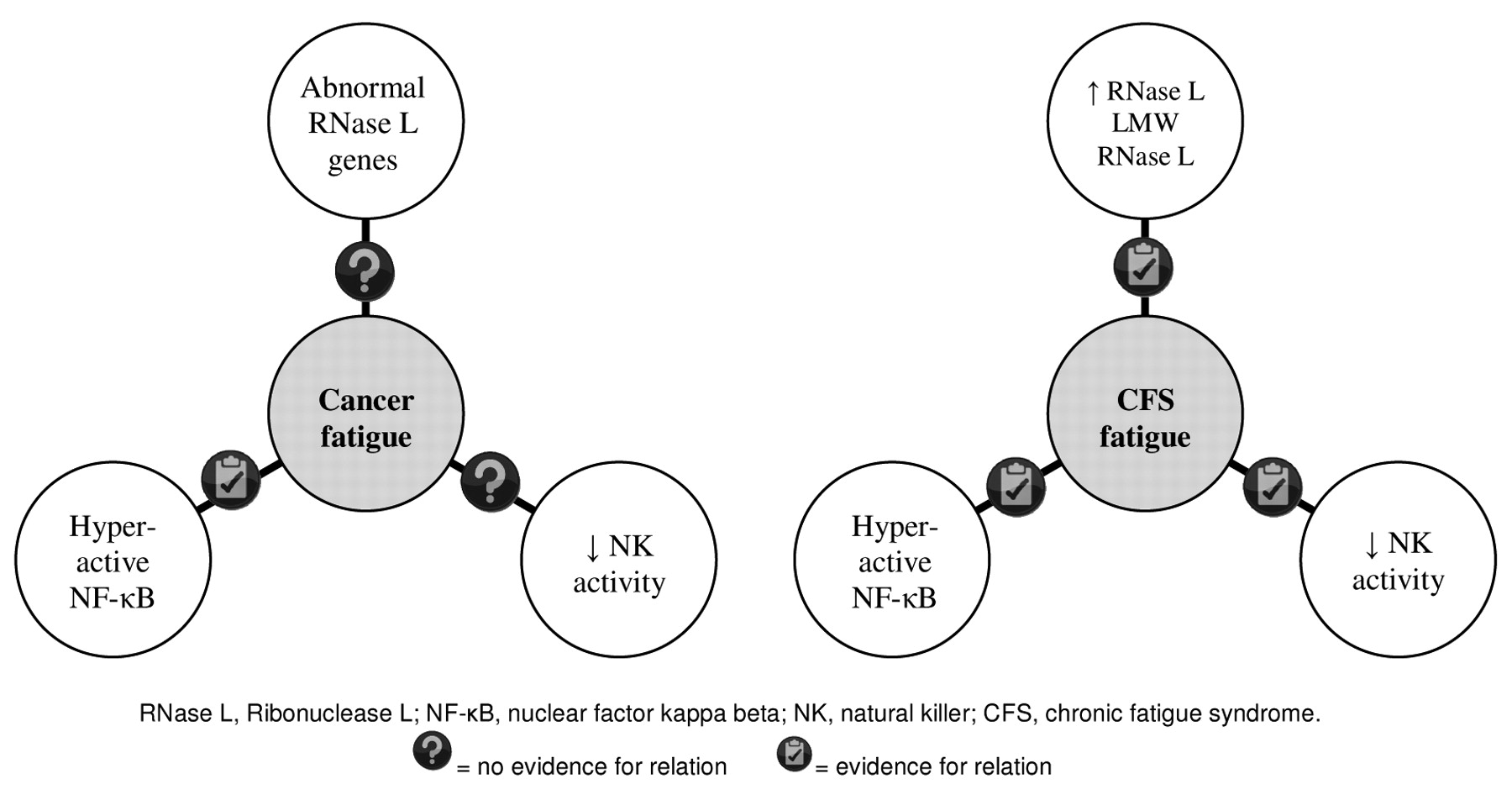
Cancer patients. Given the established role of immune dysfunctions in the fatigue experienced by CFS patients and the overlap in immune dysfunctions between CFS and cancer, we hypothesize that the 2-5A synthetase/RNase L pathway is impaired in fatigued cancer patients compared to non-fatigued patients and healthy controls. Likewise, it is hypothesised that NK cell functioning is decreased in fatigued cancer patients compared to the non-fatigued. Literature concerning this relation in cancer is currently lacking. Only on NF-κB is there some evidence for its relation to fatigue.
It is proposed that cancer-related symptom clusters, which include fatigue, share common cytokine-based neuroimmunological mechanisms. The review of Lee et al. (90) provides evidence for a correlation between the altered cytokine profile and cancer-related symptoms. The expression of coexisting symptoms such as fatigue could thus be linked to the dysregulated activity of NF-κB.
As presented in Figure 1, there is already evidence for the relation between immune dysfunctions and fatigue in CFS, but in cancer this relation is far less understood.
Discussion
It may be clear that fatigue is a major complaint in both diseases. Exact causes are not yet identified, but several contributing factors could apply for both CFS and cancer-related fatigue. The immunological problems in particular are clearly apparent and quite similar in both diseases.
RNase L is likely to play a role in the protection against cancer reoccurrence in cancer survivors and various intracellular pathogens. In those with CFS, a literature review concluded that proteolytic cleavage of the native RNase L enzyme is characteristic of this nosological entity (54). In addition, and in contrast to the reduced catalytic activity of RNase L in prostate cancer (40), there is increasing evidence for up regulation of various aspects of the 2-5A synthetase/RNase L pathway in CFS (54). Another intracellular immune dysfunction apparent in both entities is the hyperactivation of NF-κB, leading to inflammation and increased (cytotoxic) NO concentrations (50, 51, 59, 60). Finally, NK cytotoxicity seemed reduced in both patient groups, with frequent familiar aggregation of low NK syndrome in both CFS and cancer (65). In CFS, it has already been shown that these immunological abnormalities are related to the experienced fatigue. In cancer, however, more research is warranted to explore the relation between the cancer-related fatigue and the specific immune dysfunctions.
Since, for example, RNase L and NK cells may play a role in both the disabling fatigue and the protection of cancer patients against cancer reoccurrence, it would be important to target treatment approaches at improving functioning of these immune aspects. Several pharmacological therapies could offer a solution, but rehabilitation might also be beneficial. Given the fact that appropriate amounts of physical activity have positive effects on the number and cytotoxicity of NK cells in both healthy humans (72) and cancer patients (91), sufficient physical activity could be an important item in rehabilitation, especially since both CFS and cancer patients seems to be rather passive (92-96). A lack of physical activity might not only predispose cancer patients to experience severe fatigue, it might even decrease NK cell functioning and hence make them prone to cancer reoccurrence (97, 98). In addition, in CFS patients, light physical activity is associated with better well-being (unpublished data).
In consequence, exercise is currently recommended as a conservative intervention for both fatigued cancer patients and CFS patients. However, with regard to these immunological abnormalities, prudence is called concerning exercise during the rehabilitation of these patients. Based on literature findings and our own results, we know that intracellular immune dysfunctions restrict exercise capacity, but also that too vigorous exercise may further worsen the immune system (99, 100) and the complaints in CFS patients (1). The exercise response to intensive activity in cancer patients is less understood. Several conditions during cancer treatment and recovery can preclude any physical activity, including chest pain, irregular pulse, acute vomiting, blurred vision, sudden onset dyspnoea, bleeding, and extreme immunocompromised states. Moreover, many patients suffer anaemia and some patients are at risk of lymphoedema development (101). From animal studies, there is also evidence that high-intensity (>80% of maximum heart rate), high-volume physical activity in cancer patients may increase the spread of the disease (102). On the other hand, it is well known that moderate exercise has beneficial effects on the immune system and may even have preventive effects on cancer in all disease stages. Therefore physical rehabilitation should be carefully balanced. But it is clear that far more research is warranted to guide the conservative treatment and the rehabilitation of these patients.
In conclusion, despite the major difference in mortality rates, there are many points of clinical overlap between cancer patients and CFS patients. Fatigue and immunological abnormalities especially have surprisingly similar characteristics. The relation between cancer-related fatigue and immune dysfunctions deserves further research in cancer patients. The application of physical activity schemes, which could be beneficial in both pathologies, also needs more research regarding the risks and benefits.
- Received July 31, 2009.
- Revision received October 8, 2009.
- Accepted October 15, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}