


Abstract
Background: Pure signet-ring cell colorectal carcinoma (SRCC) is an infrequent and highly malignant histological variant of colorectal cancer (CRC), while it is present as a histological component in colorectal carcinomas more frequently. Materials and Methods: The aim of this work was to widen the knowledge of the biological factors involved in the pathogenesis and aggressiveness of SRCC by the identification and evaluation of possible molecular abnormalities. By means of immunohistochemistry the expression of the proteolytic degradation enzyme matrix metalloprotease (MMP)-1, that is a collagenase specifically degrading collagens I, II, III and of the adhesion proteins E-cadherin, β-catenin and fibronectin which are usually involved in the carcinogenesis of conventional colorectal tumours was investigated. Results: SRCCs showed a significantly greater MMP-1 expression compared to the ordinary intestinal colorectal cancer (ICRC) and a significantly reduced E-cadherin, β-catenin and fibronectin expression. Conclusion: The biological aggressiveness and strong metastatic behaviour of SRCC could be due to high MMP-1 and low expression of the adhesion molecules.
Pure signet-ring cell colorectal carcinoma (SRCC) is a rare form of colorectal cancer (CRC), reported to be approximately 1-2% of all CRCs (1), but the signet ring cell histotype is more frequently present in many intestinal carcinomas <50% of tumour component (2). This component grows in a diffuse fashion and in contrast to the pattern of mucinous carcinomas, these tumours synthesise all their mucin in the intracellular space. This intracellular production of mucin results in the displacement of the nucleus, so that the cancer cells acquire the typical signet ring configuration. A substantial number of studies have reported that SRCC presents different biological behaviour and a different clinical course compared to ordinary colorectal adenocarcinomas (3).
SRCC has a worse prognosis and relatively greater drug resistance than ordinary intestinal colorectal cancer (ICRC), and also shows aggressive infiltration to surrounding tissues, the frequent peritoneal seeding (2). These observations might suggest a different molecular behaviour implying characteristic carcinogenesis and progression of SRCC.
In a previous study, we found that SRCC expressed very low levels of Ki-67 (a proliferation marker) suggesting that these cells were in a post-mitotic phase of the cell cycle, and very low levels of thymidylate synthase (4), the main target of the most common drug used in CRC therapy 5-fluorouracil (5-FU) (5), which could be one reason for the frequent drug resistance of SRCC (6).
Metalloproteases play key roles in the responses of cells to their microenvironment. By effecting proteolytic degradation or activation of cell surface and extracellular matrix (ECM) proteins such as collagen and laminin, they can modulate both cell—cell and cell—ECM interactions, which influence cell differentiation, migration, proliferation and survival (7). Both secreted and membrane-bound forms of metalloproteases have been implicated in pericellular proteolysis. Cells use various strategies to regulate extracellular proteases: transcriptional regulation, trafficking of membrane-bound forms (secretion and endocytosis), activation of latent proenzyme forms, extracellular binding proteins and the action of endogenous inhibitors. Matrix metalloprotease (MMP)-1, is a collagenase specifically degrading collagens I, II and III, and is involved in tumour invasion and metastasis (8). It is the predominant collagenase of resident cells, and of endothelial cells (9), tissue macrophages (10), synovial cells (11-12), and fibroblasts (13-14). Its expression has been found in various cancer tissues (15-17), but there are no reports on its expression in SRCC. Some adhesion proteins such as E-cadherin, β-catenin and fibronectin, are usually involved in the carcinogenesis and metastatic behaviour of conventional CRC. E-cadherin, is involved in cell—cell adhesion through calcium-regulated homophilic interaction, whereas in its intracellular domain, it connects to the actin cytoskeleton via catenins. E-cadherin has a significant function in intracellular adhesion of epithelial cells, the establishment of epithelial polarization, glandular differentiation and stratification. Down-regulation of E-cadherin expression has been observed in a number of carcinomas and is usually associated with advanced stage and progression (18).
β-Catenin is an 88 kDa multifunctional protein playing an essential role in cell-cell adhesion by binding to the transmembrane protein, cadherin. β-Catenin is also involved in the regulation of gene expression as a mediator of the Wnt signaling pathway. The expression and intracellular localization of β-catenin is altered in many types of carcinomas, such as breast cancer (19).
Fibronectin is a dimeric glycoprotein which is present in cells, ECM and blood. It possesses at least four binding sites for collagen, glycosaminoglycans, transglutaminase and cell surface receptor. Fibronectin is involved in cell adhesion, tissue organization, and wound healing, and fibronectin low carcinomas expression has been shown to be associated with many tumours, such as gastrointestinal carcinomas (20)
Few studies have investigated the mechanism of the distinctive phenotype and aggressive clinical behavior of SRCC, thus the aim of this study was to assess the expression of the proteolytic degradation and adhesion protein molecules MMP-1, E-cadherin, β-catenin and fibronectin in SRCCs compared to ICRCs in order to identify the distinct biological profile of these tumours.
Materials and Methods
The study used formalin-fixed, paraffin-embedded primary tumour samples of 102 patients who had undergone surgery for previously untreated CRC, retrieved from archival material.
Immunohistochemistry assay. For each case, 10 serial 5-micron sections from the formalin-fixed tissue blocks, dewaxed and rehydrated, were used. Antigen retrieval was carried out using Dako antigen retrieval fluid and microwaving at 850 W for a total of 15 minutes, divided into 3 periods, each lasting 5 minutes, adding distilled water during the break between each microwaving. The sections were then treated with 3% hydrogen peroxidase for 5 minutes, followed by the monoclonal antibodies: E-cadherin clone NCH-38, at a dilution of 1:50 for 30 minutes; β-catenin clone Beta- catenin 1, at a dilution of 1:30 for 30 minutes, fibronectin clone FBN11, at a dilution of 1:50 for 30 minutes and MMP-1, at a dilution of 1:100 for 30 minutes. Visualization was obtained by incubation with anti-mouse rabbit and goat antibody (Dako) for 15 minutes, followed by a streptavidin-biotin peroxidase complex (Dako) for 15 minutes and finally, Dako chromogen for 5 minutes. Mayer's haematoxylin was used to counterstain the sections. As a positive control the normal mucous glands, present adjacent to the tumour, were used. Negative controls, lacking primary antibody, were included in each run of immunohistochemistry
Clinicopathological features of patients.
Staining was evaluated as being positive when the intensity of staining of the samples (cytoplasmatic and/or nuclear) was greater than the control intensity of staining. The staining positivity for every patient was evaluated in 10 microscopic high power fields (HPFs) in which the neoplastic epithelial area was more than 70% of the whole field.
The staining positivity was evaluated semi-quantitatively as strong positivity (+++) if more than 50% of the neoplastic areas were positive; mild positivity (++) if 10-50% of neoplastic areas were positive, or negativity (—) if less than 10% of the neoplastic areas were positive.
Statistical analysis. Differences in the distribution of the study variables, and associations between variables were assessed by means of the Chi-square test.
Results
The clinicopathological features of the patients are summarised in Table I. The histopathological features of the tumours were evaluated by two different pathologists and classified as follows: ICRC, 70 cases, of which 22 were well-differentiated, 35 were moderately differentiated and 13 were undifferentiated, and SRCC, 32 cases. Their classification according to Dukes' system is shown in Table II.
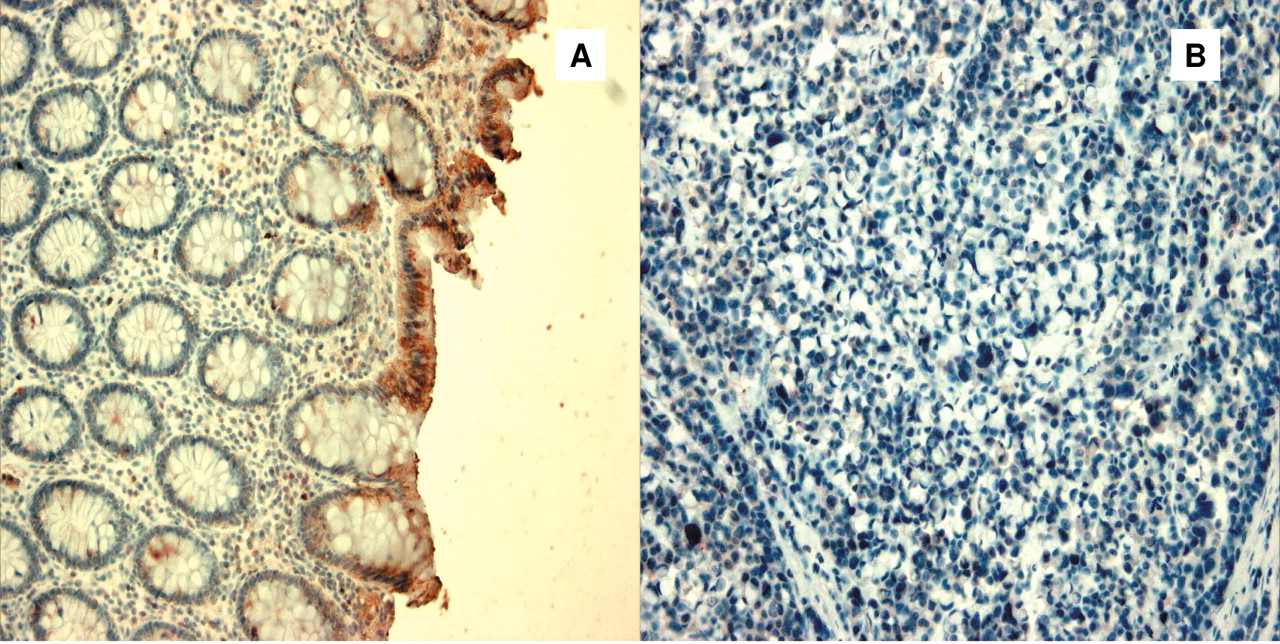
Immunohistochemical staining of E-cadherin, β-catenin, fibronectin and MMP-1. Normal colonic epithelium showed basolateral membrane staining for E-cadherin, β-catenin and fibronectin along the entire length of the crypt; this served as an internal positive control.
The ICRCs showed variable degrees of membrane expression of these markers. It was noted that no expression of E-cadherin was found in 16% of the cases, while 84% of the samples were strongly positive; β-catenin was moderately expressed in 28% of the samples and highly expressed in 72% of the samples; fibronectin expression was moderate in 60% and high in 40% of the ICRC tumours. The SRCC samples were 100% negative for E-cadherin and fibronectin staining (Figures 1 and 2), while staining for β-catenin was negative in 75% (Figure 3) and moderately expressed in 25% of the tumour samples (p<0.001) These results are summarized in Tables III, IV and V.
Dukes' stage of patients included in the study.
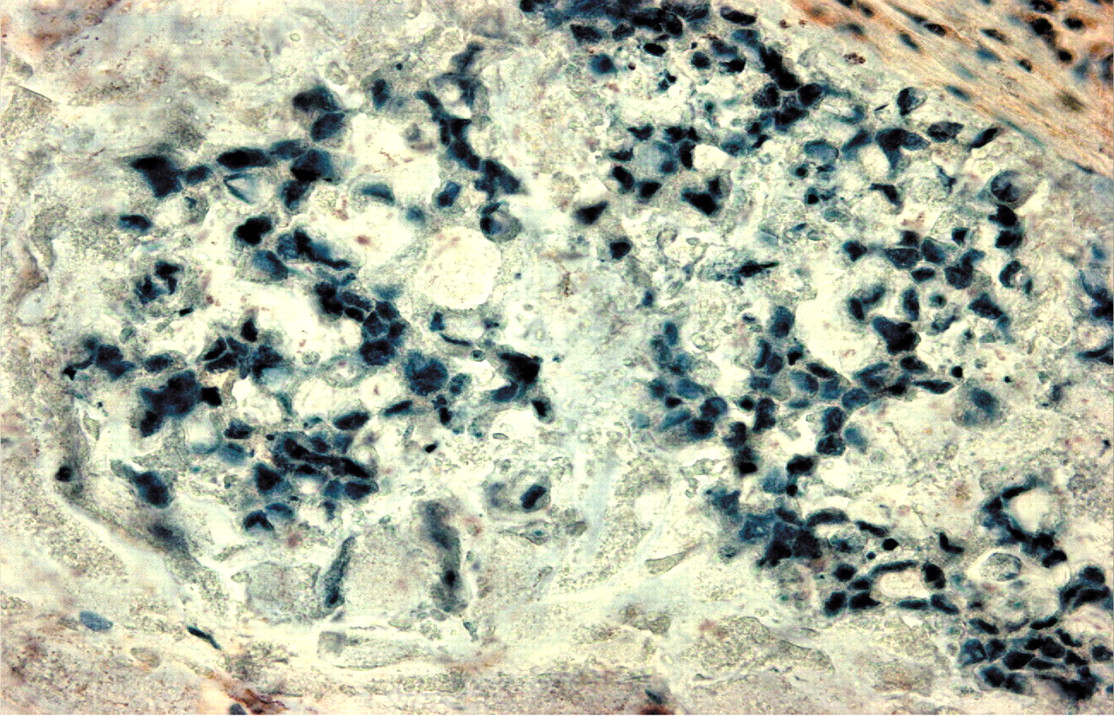
MMP-1 expression was found predominantly in the cancer cells, but also some stromal cells and endothelial cells stained weakly. In the MMP-1-positive cells, diffuse staining was observed in the cytoplasm of the cells. Some tumours stained diffusely and others focally, at different intensities, but SRCCs showed a higher expression of MMP-1 overall in the invasion front of the tumour and in the neoplastic embolus compared to ICRCs (p<0.001) (Table VI). Haematogenous metastases of SRCCs highly expressing MMP-1 staining were found (Figure 4).
Discussion
In this study, SRCCs showed a significantly greater MMP-1 expression compared to the ICRCs, and this could be a reason for the major aggressiveness and metastatic behaviour of SRCC which is demonstrated in spite of their proliferation index (4). As MMPs seem to play important roles in tumour invasion and metastasis, recently they have gained attention as targets for new anticancer therapy strategies. Inhibitors of MMPs have been shown to prevent tumor spread both in vitro and in vivo (21-23) and to inhibit tumour angiogenesis (24), and some are being developed for clinical use. Marimastat, a synthetic low-molecular weight inhibitor of MMPs, is currently in phase I/II and III clinical trials with satisfactory preliminary results, but some side-effects have been reported (25-27). An anti-MMP therapy could be advisable for those patients bearing SRCCs because of their poor prognosis and hyperexpression of MMP-1.
The loss of function in any of the E-cadherin—catenin complex components has been suggested as the cause of the loss of epithelial differentiation and architecture, or the acquisition of a motile and invasive phenotype. Alteration in the expression or function of E-cadherin in carcinomas may allow certain carcinoma cells to be readily detached from the surrounding structure and thereby develop a more infiltrative growth pattern (18). A variety of human malignancies, including thyroid, oesophageal, gastric, and colonic adenocarcinomas, showing a reduced E-cadherin expression, have been found to develop greater tumour de-differentiation, greater infiltrative growth, and lymph node involvement (28-31). In the present study, significantly reduced E-cadherin, β-catenin and fibronectin was found expression in the SRCCs, suggesting that the aggressive biological behaviour of SRCCs is partly attributable to this altered molecular profile. Further studies will be necessary to understand other possible mechanisms responsible for the aggressiveness and above all for the frequent drug resistance, for example possible alterations in the apoptotic pathway, of SRCC.
Expression of E-cadherin in SRCC and IRCC.
Expression of β-catenin in SRCC and IRCC.
Expression of fibronectin in SRCC and IRCC.
Expression of MMP-1 in SRCC and IRCC.

E-cadherin expression in (A) normal colonic mucosa and (B) SRCC.

Fibronectin expression in SRCC.

β-Catenin expression in (A) normal colonic mucosa and (B) SRCC.

MMP-1 expression in SRCC forming a neoplastic embolus.
Acknowledgements
This work was supported by University of Palermo and MIU grants.
- Received June 29, 2009.
- Revision received October 8, 2009.
- Accepted October 13, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}