


Abstract
Background: The majority of gastrointestinal stromal tumours (GISTs) contain oncogenic KIT (v-kit Hardy-Zuckerman 4 feline sarcoma viral oncogene homolog) or platelet-derived growth factor-alpha (PDGFRA) receptor tyrosine kinase (TK) mutations and are initially, but only temporarily sensitive to TK inhibitors. The aim of this study was to establish and characterize a human GIST xenograft that could be used for evaluating various molecularly targeted therapies. Materials and Methods: GIST tissue from four patients was implanted under the skin of athymic nude mice. In one case a tumour line was established. Results: The xenograft showed characteristic GIST morphology and exhibited the same mutation profile as that of the patient. Conclusion: A human GIST xenograft with mutation in KIT exons 11 and 17 has been established and maintained in nude mice for 3 years (13 passages). This model will enable further studies on mechanisms of resistance, combination therapies and allow testing of novel targeted therapies.
Gastrointestinal stromal tumour (GIST) is the most common malignant mesenchymal tumour of the gastrointestinal tract (1) and accounts for 1-3% of all gastrointestinal malignancies with an annual incidence of 6-20 cases per million (2-4). It is believed that GISTs arise from mutations in the interstitial cells of Cajal or in precursors of these cells (5).
Surgery is currently the first-line treatment for patients with primary resectable GIST (6, 7). A large portion of patients develop recurrent or metastatic disease despite complete surgical resection (8), and conventional chemo- or radiotherapy is ineffective (9). Tyrosine kinases (TKs) are common oncogenes and the human genome contains about 90 TKs and 34 gene-like TKs (10). Abberent TK signalling is an important feature of malignant transformation (11) and whereas transmembrane receptor TKs transduce extracellular signals by ligand binding, cytoplasmic TKs relay intracellular signals (12).
The majority of GISTs have mutations in the receptor TK gene KIT, (v-kit Hardy-Zuckerman 4 feline sarcoma viral oncogene homolog) in regions that encode auto-regulatory domains of the TK (4). These mutations occur predominantly in KIT exon 11 (66%) and exon 9 (10-18%) (1, 4, 13). GISTs with mutations in KIT exon 13 or exon 17 are less common (4). A few GISTs harbour mutations in the related TK gene PDGFRA encoding platelet-derived growth factor receptor α (4, 13). Previous studies have shown that 10-14% of GISTs have no identifiable receptor TK mutations (1, 4, 13). Activating KIT or PDGFRA mutations have been defined as the driving force and the underlying pathogenic event in GIST development. Understanding the molecular pathophysiology of GIST has allowed the development of agents targeting and selectively inhibiting TK activity (9). Suppressing signal transduction pathways results in reduced cell proliferation and the induction of apoptosis (14).
The introduction of these new targeted drugs has significantly improved the prospects for patients with locally advanced or metastatic GIST and the TK inhibitor imatinib is currently the standard, first-line treatment for these patients (15, 16) and the use of imatinib has improved overall survival by 4 years as compared to conventional chemotherapeutic treatments (8, 16). However, the majority of patients for whom imatinib is initially effective, will eventually develop resistance to the drug. Furthermore, about 19% of GIST patients do not respond to imatinib and another 5% develop unacceptable adverse effects (17). Secondary or late resistance develop after a median of almost 2 years of treatment (18, 19). During the past years other signal transduction inhibitors have been developed, such as sunitinib, nilotinib and sorafenib (17, 20, 21). Out of these TK inhibitors (TKIs), only sunitinib has reached clinical practice as second-line treatment when imatinib resistance occurs (17).
Tumour characteristics of the human GIST tissue used in attempts to establish human xenografts in athymic nude mice.
This study describes the establishment of a human GIST xenograft from an imatinib resistant tumour, its histology, immunohistology and molecular characteristics.
Materials and Methods
Establishment of the GIST xenograft. Between November 2005 and June 2006 tumour tissue from surgically removed GISTs in 4 patients was implanted into athymic nude mice (Table I). For patient 1 tumour tissue was obtained from resection of a GIST metastasis performed one year after primary surgery. For patients 2-4 tumour tissue was obtained from surgical resection of the primary tumour. Patient and tumour characteristics of the resected GIST tissue that was implanted subcutaneously into athymic nude mice are given in Table I.
Tumour tissue was collected in serum-free RPMI 1640 medium and immediately processed for transplantation. The tumour specimen was cut into small fragments (2 mm)3 and kept in a petri dish containing physiological saline. The tissue fragments were implanted bilaterally into 6 weeks old athymic nude mice (n=3). Growth factors, hormones, matrigel or other supplements were not used.
Tumour tissue from four patients was implanted, but only tissue from patient 1 engrafted. From this patient, tumours developed bilaterally in all three nude mice. Tumour growth was monitored and reached 1 cm in diameter after 3 months. The tumour line has, since November 2005, been maintained by serial passage in athymic nude mice in our animal facility. Frozen specimens from some of the passages have been stored.
Tumour growth curve. To assess tumour growth of the established human GIST xenograft, tumour tissue ~(2 mm)3 from passage 13 was implanted subcutaneously in 3 athymic nude mice. Tumour volume was measured weekly with an external caliper. Individual tumour volumes were calculated using the modified ellipsoid formulae (22, 23). Tumour volume=½·(a·b2) with a being the longest longitudinal diameter (length) and b the longest transverse diameter (width) of the xenograft.
Case history (Patient 1). A 41 year old male developed flu like symptoms with fever and malaise followed by abdominal pain for which he was admitted to hospital. He underwent ultrasound and computed tomography (CT), which showed a tumour with a diameter of 13 cm in the epigastrium situated between the ventricle, left liver lobe, aorta and pancreas. A tumour mass in the lower mediastinum was also found. Histological evaluation of a needle biopsy confirmed the diagnosis of a CD117+ GIST.
One month later a solid tumour mass of 2 kg was removed surgically together with local abdominal metastases and the mediastinal tumour. Pathological examination of the primary tumour revealed a malignant GIST with a mitotic count of 20/50 high-power fields (HPF). The postoperative course was uneventful and the patient was discharged one week later.
Two months after primary surgery the patient reported tenderness below the right costal margin and a swelling in his right groin. A gamma camera 18-fluoro-deoxy-glucose positron emission tomography (18FDG-PET) showed disseminated disease with FDG-avid tissue under the right diaphragm and in the right groin. Treatment was started with imatinib (Glivec®) 400 mg daily which was well tolerated. Initially, the patient responded to the treatment, and a CT performed 3 months later showed overall tumour regression. Some lesions were not visible and the others lesions were either reduced in size or exhibited decreased attenuation on CT.
Another five months later a new CT revealed reappearing tumour masses; both lesions with increased size and low attenuation and new high attenuation lesions. The imatinib dose was increased to 600 mg daily. The patient's general condition was still good and he was working full time.
Two months later the patient presented acute abdominal pain. CT showed small amounts of blood in the abdomen, suspected to be a result of tumour bleeding. PET/CT showed increasing tumour masses with intense FDG uptake in a large tumour in the epigastrium and one in the pelvis. Imatinib was increased to 800 mg daily and visible tumour masses and the omentum were surgically removed. Tumour tissue from the large tumour in the epigastrium was implanted bilaterally into three nude athymic mice.
One month later the patient again reported increasing abdominal pain and a new tumour was found in the omentum minus. After additional three months he was readmitted with ileus. Multiple tumour masses in the abdomen were again removed surgically and he was given the second line TKI sunitinib (Sutent®). The patient was stable for one month, before he again developed ileus. The abdomen was now filled with tumour masses and ascites was present. He received two 4-week courses of sunitinib, but he died four weeks later, 22 months after the initial diagnosis.
KIT and PDGFRA primer sequences (5′->3′).
Histopathological examination and immunohistochemistry. Material from the primary tumour and subsequent surgical specimens were reviewed by an experienced sarcoma pathologist (B.B.). Paraffin-embedded tissue was processed for staining with haematoxylin and eosin (HE) and microscopic examination. The mitotic index was counted in 10 or, if possible, in 50 HPF (objective ×40). For immunohistochemistry, formalin-fixed, paraffin-embedded tumour tissue was cut into 3 μm sections, deparaffinized and pretreated in a microwave oven for heat-induced epitope retrieval. The antibody CD117 (c-kit) was employed (polyclonal, 1:100, Dako Denmark A/S, Corporate Headquarters, Glostrup, Denmark).
Polymerase chain reaction (PCR) and sequencing. DNA was extracted from passage 7 of the GIST xenograft. PCR was performed using 50 ng genomic DNA, Hotmaster Taq DNA polymerase (5 PRIME, Hamburg, Germany), and PCR primers (Invitrogen, Paisley, UK) (Table II). Cycling conditions were as follows: denaturation for 2 min at 94°C; amplification for 40 cycles, with denaturation for 20 sec at 94°C, annealing for 10 sec at 60°C and extension for 20 sec at 65°C. After the last cycle, a final extension at 65°C for 4 min was performed. Sequencing reactions were performed using the BigDye Terminator v3.03 cycle sequencing kit (Applied Biosystems Inc, Foster City, CA, USA). The cycle sequencer products were run on an automatic capillary sequencer ABI PRISM 3100 Genetic Analyzer (Applied Biosystems).
Results
Establishment and tumour characteristics. To date the established GIST xenograft has been maintained for over 3 years and 13 passages in athymic nude mice with a tumour take of around 75%. Tumour doubling time for the 13th passage was found to be about 40 days. Microscopic examination of the initial human GIST metastasis and the xenograft (passage 8) revealed similar morphological appearance (Figure 1), comprising moderate cellular tissue with atypical epitheloid and spindle cells. The mitotic count in the xenograft was much higher (25/10 HPF) than in the human GIST (3/10 HPF for the GIST metastasis and 20/50 HPF for the primary tumour). The human GIST and the xenograft after 8 passages both showed positive staining for CD117 (Figure 1).
Genetic karyotype and molecular characterization. Cytogenetic analysis of xenograft tissue confirmed that it was of human origin (data not shown). Mutation analysis of KIT (NM_000222.2) exon 9, 11, 13, 14 and 17 and PDGFRA (NM_006206.4) exon 12 and 18 was performed by direct sequencing. Mutations were detected in KIT exon 11 (c.1673_1687del, p.Lys558_Glu562del) and in KIT exon 17 (c.2446G>C, p.Asp816His) (Figure 2). These mutations were identical to those found in the biopsy from the patient metastasis obtained after ten months with imatinib treatment.
Discussion
A new human GIST xenograft, denoted AHAX, originating from a patient with an imatinib resistant GIST, was established and characterized. When the present study was initiated no other GIST xenograft studies had been published. During the study, a Belgian group described the establishment of the first human GIST xenograft (24). Here the GIST xenograft was established from a GIST cell line grown in vitro and their experiment was conducted on the initial passage (24). Recently, another study has reported the establishment of two other human GIST xenografts (25). The tumour take in that study was similar to the present study. Implantation of tumour tissue from 7 human GISTs into SCID mice yielded 2 viable xenografts (25) both with mutations in KIT exon 11. Those xenografts were slow-growing and first detectable 58 and 62 weeks post-transplantation. The present tumour tissue was taken from a metastatic GIST lesion from a patient with a mutation in KIT exon 11 and a secondary mutation in KIT exon 17; mutations that were maintained in the established xenograft. The GIST xenograft here presented grew bilaterally in three athymic nude mice with an initial take rate of 100%. For the 8th generation the take rate had declined to 75% with a tumour doubling time of about 40 days. The xenograft is still being maintained through serial passages in our animal department. One interest of this tumour resides in it being from an imatinib resistant tumour.
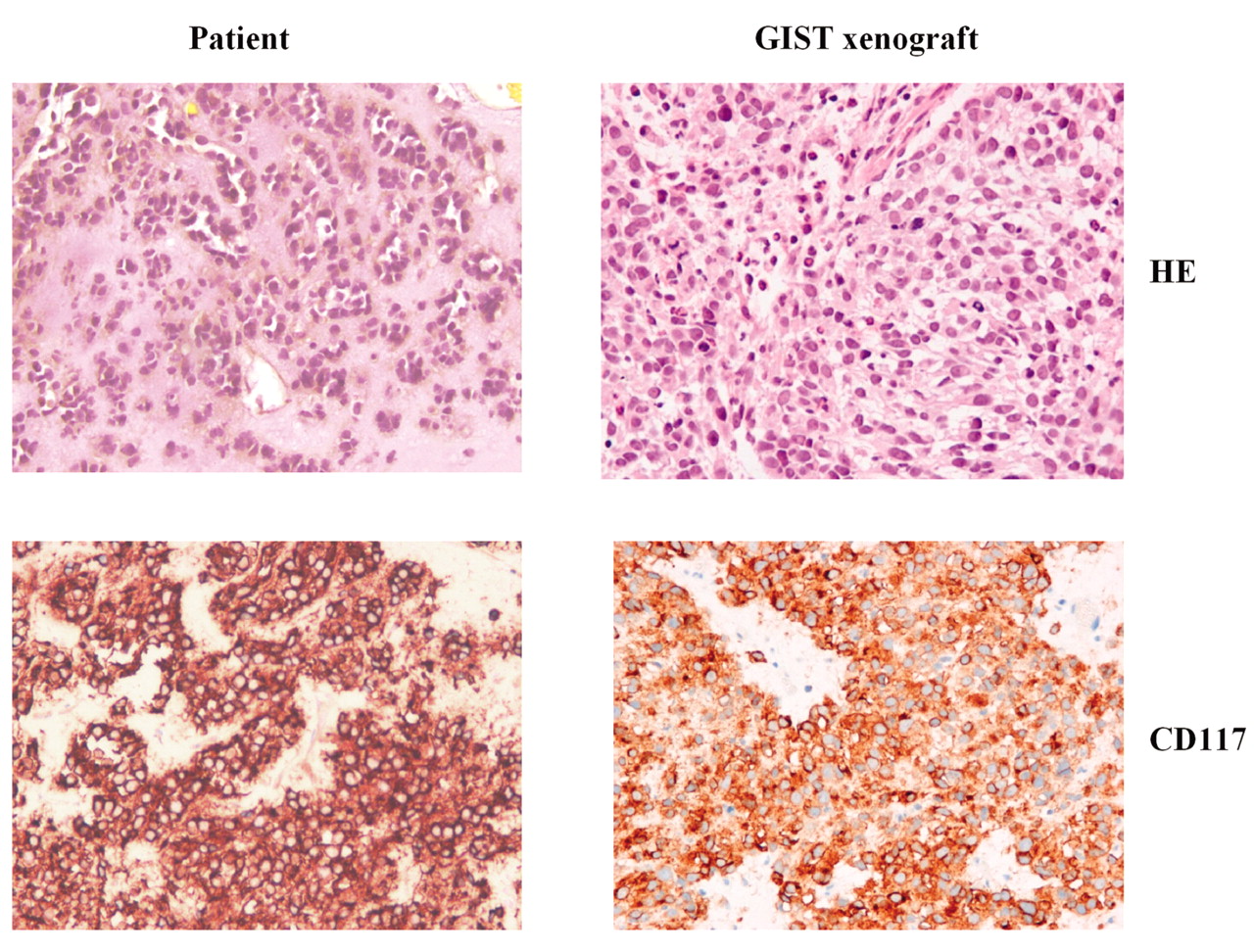
HE stain and immunohistological staining of CD117 of the initial human GIST metastasis and the GIST xenograft established from this tumour.
Although imatinib has been shown to be effective as first line treatment for GISTs most patients will eventually develop imatinib resistance (13, 17, 26). Such resistance can develop through various mechanisms, the most common being secondary KIT mutations such as in exon 17 in clonally expanded cancer cells (27, 28). The fact that the present established xenograft harbours both exon 11 and 17 mutations may indicate that its behaviour upon treatment will mimic the clinical situation.
The mitotic index in the xenograft was higher than both the initial primary tumour of the patient and the metastatic tumour tissue used for implantation and establishment of the human GIST xenograft. The difference between primary tumour and xenograft could be related to altered tumour cell composition occurring following the onset of TKI treatment. Tumour cell biology could also initially be different between the primary tumour and its metastasis due to an evolution in the primary tumour that has led to the development of local and/or distant metastasis. As this tumour was extracted while the patient was under imatinib treatment, it may be speculated that, even in the case of imatinib resistance, the mitotic rate may be suppressed by imatinib treatment.
The established GIST xenograft may be used to study the mechanism of resistance, combination therapies and novel targeted therapies. It may also be used to develop new more specific biomarkers to GIST. In the future, other xenografts with different KIT mutations could give the opportunity to confirm the differences in treatment response to novel targeted therapies and to other TKIs. Recently, there has been an expansion of pharmacogenetics and attempts to identify potential responders to a candidate drug to provide individualized cancer treatment.

Sequencing of KIT exon 17 mutation (c.2446G>C, p.Asp816His) in A) the human GIST xenograft, B) the primary human GIST tumour prior to imatinib treatment and C) the human GIST metastasis after imatinib treatment.
In conclusion, a human GIST xenograft with KIT mutations in exon 11 and 17 was established from a human GIST metastasis. The xenograft can be used to test new drugs such as TKIs and other agents being developed to circumvent treatment resistance.
Acknowledgements
The authors greatly acknowledge the technical assistance provided by Alexandr Kristian, Department of Tumor Biology, Oslo University Hospital, Oslo, Norway and Ludmila Gorunova Department of Medical Genetics, Oslo University Hospital, Oslo, Norway.
- Received July 3, 2009.
- Revision received September 24, 2009.
- Accepted September 28, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}