


Abstract
Cancer is the second leading cause of death in the world. Radiolabeled nanocarriers or nanoparticles can be designed and used for cancer diagnostic and therapeutic purposes when tagged with appropriate radionuclides. Current progress in nanotechnology and nanomedicine has exploited the possibility of designing tumor-targeted nanocarriers able to deliver radionuclide payloads in a selective manner to improve the efficacy and safety of cancer imaging and therapy. The major nanocarriers include liposomes, dendrimers, quantum dots, iron oxide and carbon nanotubes. In addition, the combining of tumor specific multifunctional and multimodality nanocarriers will hopefully achieve earlier tumor detection and better tumor treatment. Several radiolabeled multifunctional and multimodality nanoparticles have been effectively demonstrated in detecting and treating cancer in animal models. However, further preclinical and clinical efficacy and toxicity studies are required to translate these advanced technologies to the health care of cancer patients. The aim of this article is to provide a brief overview of current status of applications, advantages and up-to-date research and development of nanotargeted radiopharmaceuticals in cancer imaging and therapy.
More than 12 million cancer cases and 7.6 million cancer deaths were reported in 2007 worldwide (1). The incidence and mortality of cancer were about 5.6 million and 2.7 million, respectively in 2007 in Asia. By 2050, the global new cancer incidence is expected to grow to 27 million, and the cancer mortality will be 17.5 million (1). To conquer cancer is really a challenge of health care for mankind. Cancer exhibits up-regulated cell growth, with an ability for tumor cells to invade and metastasize. A century ago, Paul Ehrlich hypothesized that a ‘magic bullet’ could be developed to selectively target cancer disease (2). Over the past few decades, the progress in molecular biology and the understanding of malignant transformation and tumorigenesis have revealed the two major classes of anti-tumor therapeutics: i) Application of molecularly targeted therapeutics to block hallmarks of cancer, and ii) Employing drug delivery systems through tumor-targeted nanomedicines to improve the pharmacokinetics and bioavailability of vehicle-carried drugs. From 1980 to 2005, a total of 205 monoclonal antibodies (mAb) were studied in clinical trials (3-5). The US Food and Drug Administration (FDA) approved the first anti-CD20 mAb (Rituximab) for the treatment of non-Hodgkin's lymphoma in 1997. To date, 12 of these anticancer molecular-targeted mAbs have been approved worldwide (4, 5).
Conventional anticancer drugs exhibit a lack of specificity, poor solubility and distribution, unfavorable pharmacokinetics and high tissue damage or toxicity. Targeted drug delivery systems such as passive and active targeting nanocarriers, with diameters ranging from 10-100 nm have been developed to improve the biodistribution, pharmacological, therapeutic and toxicity properties of agents used in cancer diagnostics and therapeutics (6-9). The status of the development of targeting delivery systems, including targeting strategies, potential applications and the prospects of tumor-targeted nanocarriers were reviewed and discussed recently (6-9). Cancer nanotechnology is expected to transform current treatment systems by providing more efficient cancer diagnostics and therapeutics. Today, nanocarriers are used in detecting cancer at an early stage, delivering anticancer drugs specifically to malignant cells, and determining if these drugs are killing malignant cells (8, 9). Two therapeutic nanocarrier-liposomes and albumin nanoparticles have been approved by US FDA for clinical practices (7, 10). As nanocarriers are evaluated for safety and efficacy, nanotechnology will bring with it significant advances in molecular imaging and specific targeting of tumor therapeutic agents, elevating therapeutic efficacy, and finally achieving the goal of early detection and control of cancer. Customized nanoscale constructs can serve as targeted drug delivery vehicles capable of delivering large doses of radionuclide or chemotherapeutic agents into malignant cells while sparing normal tissues, greatly reducing the side-effects that usually accompany many current cancer therapies (7-10).
Monoclonal antibody-guided radiation therapy, or radioimmunotherapy, demonstrated promise in preclinical and clinical anticancer applications (11-15). Two radiolabeled anti-CD20 monoclonal antibodies 90Y-ibritumomab (Zevalin®) and 131I-tositumomab (Bexxar®) were approved by the US FDA in 2002 and 2003, respectively, for treatment of B-cell non-Hodgkin's lymphoma (NHL), which indicates the potential benefit of antibody-guided systemic radionuclide-targeted therapy (11-15). Emerging new methods improve the specific uptake of radionuclides in tumor cells while sparing the normal tissues. Several advanced strategies for radionuclides delivery have been studied extensively, including the combination of chemotherapy agents with particle-emitting radionuclides and the development of novel multimodality and multifunctional therapeutics. Optimization of treatment protocols has significantly improved the therapeutic efficacy and reduced the toxicity to normal tissues. Nanoparticles delivering radionuclides for improving pharmacokinetics and therapeutic efficacy of cancer have been presented elsewhere (16, 17). The recent research progress and applications of advanced nanocarrier radiopharmaceuticals for in vivo cancer imaging and therapeutic applications will be briefly discussed and summarized in this review article.
Radionuclides for Tumor Imaging and Therapeutics
The research into tumor-targeted diagnostic and therapeutic radiopharmaceuticals is one of the potential areas of cancer drug development. Radiopharmaceuticals consist of two components, a targeting carrier and a trace amount of radionuclide with a specific radiation. The tumor therapeutic efficacy and diagnostic quality are determined by the selectivity or specificity of delivery systems and radionuclide radiation characteristics (11, 15-19).
The selection of potential radionuclides for tumor imaging (Table I) and radionuclide radiotherapy (Table II) involves the physical half-life, decay mode and the emission properties of the radionuclides. Gamma emitters with energy in the 150 keV range can be used for gamma imaging or single photon-emission tomography (SPECT), and high energy positron-emitters with energy at 511 keV energy can be applied for positron-emission tomography (PET) (16, 17, 20, 21). For targeted radionuclide radiotherapy applications, high and low energy β-emitters are ideal radioisotopes for the treatment of small to large clusters of tumor cells. The tissue penetration range (1-10 mm) (11, 18), and cross fire effect of β-particles can kill tumor cells in close proximity to neovasculature (11, 15, 18). Alpha-emitters hold great promise as therapeutics for small cancer lesions and micrometastatic cancers due to the high linear energy transfer (LET, 80 keV/μm) and short range energy depositions with tissue penetration range of 50-100 μm. Monoclonal antibody labeled with α-emitters has been demonstrated to have high specific killing effects and minimal normal-tissue damage in a tumor-bearing animal model (17). Auger electrons have an energy of <30 keV and subcellular pathlength of 2-12 μm. Thus, auger electron emitters can exert their radiotoxic effects on cells only when they are internalized into the cytoplasm (19, 22, 23).
Nanocarriers for the Targeted Delivery of Radionuclide
Targeted radionuclide therapy is often limited by insufficient delivery of radionuclide to tumor sites using the currently available targeting strategies, such as monoclonal antibodies and peptides, due to relatively low and heterogeneous expression of receptor on tumor cells, as well as dose-limiting toxicities to normal tissues. To maximize the therapeutic index and to minimize the outcome of toxicity, it is very important to deliver the radionuclides to the right site at the right concentration and at the right time. The rapidly advancing field of cancer nanotechnology has generated several innovative drug delivery systems, such as liposomes, dendrimers, quantum dots, iron oxide and carbon nanotubes, to improve and enhance targeted transport of cytotoxic drugs and radionuclides to tumor lesions. It is estimated that approximately 240 nano-enabled products entered pharmaceutical research pipelines in 2006. These nanocarrier systems could provide the delivery platforms needed for improving the delivery of radionuclide to tumor sites. Nanocarrier delivery systems have also revealed enhanced imaging and therapeutic efficacy by targeted delivery of drugs to the tumor site and by reducing their toxic side-effects (6-10). Major advantages of nanocarriers are that they can be prepared in sizes <100 nm, and selectively increase the localization of drugs and radionuclides in the tumor through passive targeting or active targeting, while sparing non-targeted tissue, ensuring minimal drug or radionuclide leakage during circulation, and facilitating intracellular drug or radionuclide delivery and uptake for active targeting (16, 17). Figure 1 shows the schematic concept of passive (A, B) and active (C, D) targeting nanoliposome encapsulated with radionuclides (A, C) and co-delivery of radiochemotherapeutics (B, D).
There are three generations of nanocarriers: i) The first generation of nanocarriers (passive targeting) which are rapidly trapped in the recticuloendothelial system (RES) organs (e.g. liver and/or spleen); ii) The second generation of pegylated nanocarriers (passive targeting), which can evade the RES of the liver and spleen, enjoys a prolonged circulation in the blood and allows for passive targeting through the enhanced permeability and retention (EPR) effect in leaky tumor tissues; iii) The third generation of nanocarriers (active targeting) has a bioconjugated surface modification using specific antibodies or peptides to actively targeted specific tumor or tissues. The pharmacokinetics and bioavailability of drugs and radionuclides delivered by the third generation of nanocarrier were much improved. One of the major challenges is to design a nanocarrier with less immunotoxic effect and to avoid higher biological barriers in the body such as to reduce delivered diagnostic and therapeutic agent uptake in the reticuloendothelial system (RES) (10).
There are five approaches generally used for labeling or encapsulating radionuclides on nanocarriers: i) Labeling nanocarriers by encapsulation during preparation; ii) nanocarrier surface labeling after preparation; iii) nanocarrier surface labeling of bioconjugates after preparation; iv) incorporation into the lipid bilayer after preparation; and v) after-loading of the aqueous phase of the nanocarriers after preparation. The after-loading method has provided higher labeling efficiencies (>90%) and the greatest in vivo stability for 99mTc,111In, and 67Ga radionuclides for nuclear imaging (16, 17, 20, 21).
Nanotargeted Radiopharmaceuticals for Tumor Imaging
The major characteristics of nanotargeted nuclear imaging modalities such as SPECT and PET are listed in Table III (16, 17, 20, 21). Liposomes are spherical bilayers of small phospholipid vesicles which spontaneously form when water is added to a dried lipid mixture. Significant progress has been made in the use of liposome as nanocarriers for the delivery of imaging radionuclides. The ability to modify the surface of nanocarriers permits improvement in the pharmacokinetics, bioavailability, toxicity and customization of nanocarrier formulations for particular tumor imaging agents (24). Selected current cancer nanotargeted nuclear imaging agents are summarized in Table IV.

Schematic representation of passive (A, B) and active (C, D) targeting nanoliposome encapsulated with radionuclides (A, C) and co-delivery of radiochemotherapeutics (B, D).
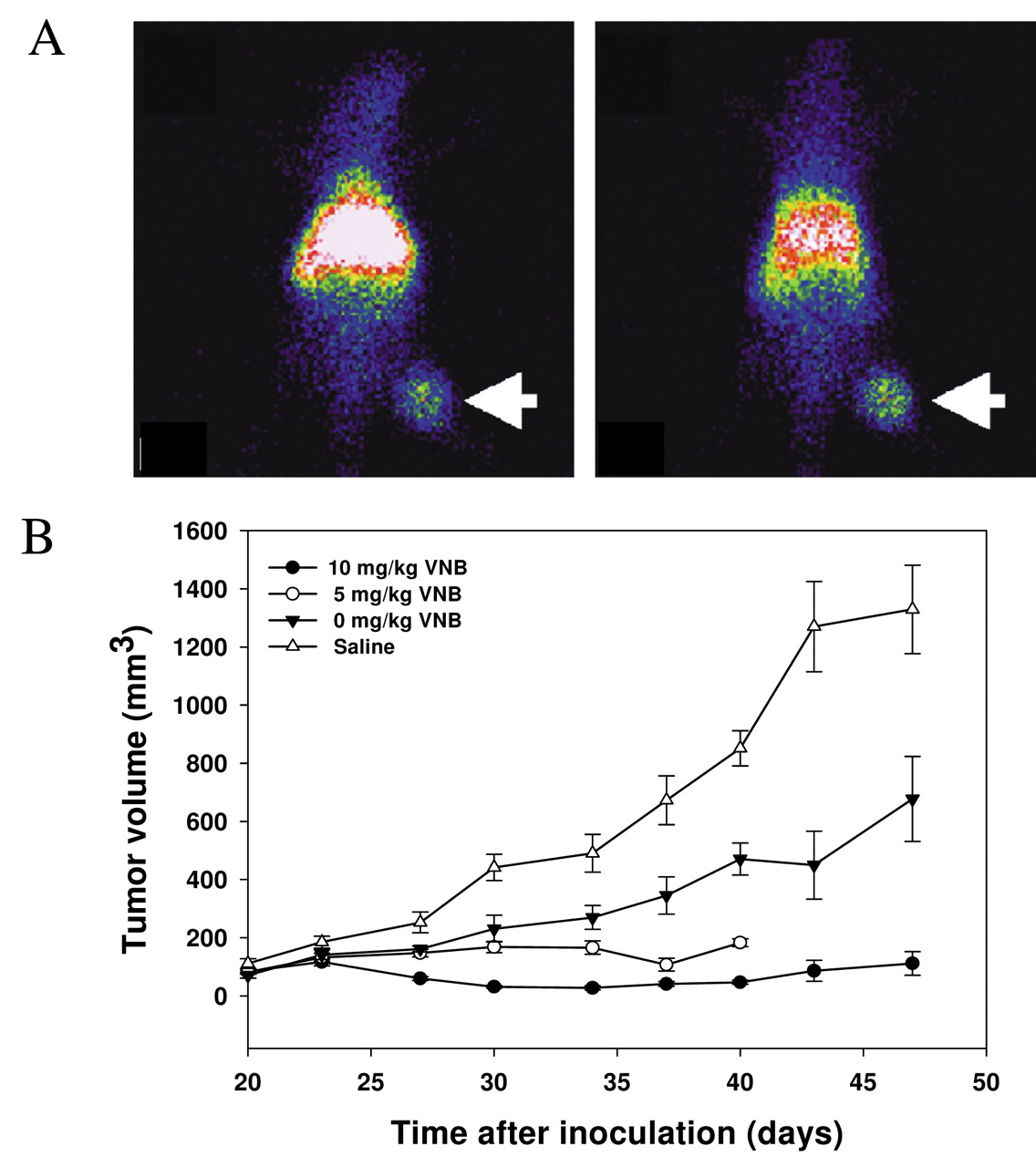
Delivery of 99mTc, 111In and 67Ga radionuclides by liposomes for gamma-imaging and monitoring drug treatment have been reviewed and reported (20, 21, 25). The biodistribution, pharmacokinetics and nuclear imaging of 111In-DTPA-labeled pegylated liposome were studied in patients with advanced local cancer (26). Effective targeting of solid tumors of breast (5.3±2.6 % ID/kg for a tumor volume of 234.7±101.4 cm3), head and neck (highest uptake of 33.0±15.8 % ID/kg for a tumor volume of 36.2±18.0 cm3), lung (18.3±5.7 % ID/kg for a tumor volume of 114.5±42.0 cm3), brain and cervix were also observed with gamma camera and SPECT imaging (26). Liposome encapsulating the positron-emitter 18F-FDG was applicable for diagnostic imaging and real-time liposomal tracking in vivo (27). Wang et al. demonstrated an intravenous administration of 111In-liposome by conjugating 111In-oxine to DTPA/PEG-liposome followed by whole-body scintigraphy. Images revealed that the tumor clearly accumulated 111In-liposome up to 48 h post injection (p.i.) (28) (Figure 2A). In addition to the diagnostic imaging of 111In-liposome, Lee et al. demonstrated the bifunctional imaging and bimodality therapeutic efficacy of 111In-VNB-liposomes in HT-29/luc mouse xenografts (29) (Figure 2B).
Enhanced tumor accumulation and visualization by γ-scintigraphy with 111In-labeled nucleosome-specific monoclonal antibody 2C5 bioconjugated immunoliposome has been studied, and the results indicated better and faster imaging in various tumor-bearing mice (30, 31). αvβ3-Integrin-targeted 111In perfluorocarbon nanoparticles have been developed and studied for the detection of rabbit Vx-2 tumor angiogenesis. The circulatory half-life was estimated to be 5 h. The mean tumor uptake was 4-fold higher than in the nontargeted control. The specificity activity (111In/NP) of 111In to nanoparticle (NP) may affect the tumor-to-muscle uptake ratio in patients. The tumor-to-muscle ratio for the nanotargeted 111In/NP=10 to 111In/NP=1 were 6.3±0.2 to 5.1±0.1, respectively. The data suggest that αvβ3-targeted 111In perfluorocarbon nanoparticles may provide a clinically useful tool for detecting angiogenesis in nascent tumors (32). 111In radiolabeled soluble functionalized multifunctional drug delivery platforms of active targeting with rituximab monoclonal antibody bioconjugated on single-wall carbon nanotubes have been developed, and the selectivity of targeting to disseminated human lymphoma were evaluated in vitro and in vivo (33).The results of the ability to specifically target tumor with prototype-radiolabeled or fluorescent-labeled, antibody-appended carbon nanotube constructs was encouraging and suggested further investigation of carbon nanotubes as a novel radionuclide delivery platform (33).

Comparisons of microSPECT/CT images of 188Re-BMEDA and 188Re-liposomes passive targeting tumors in C26 colorectal carcinoma-bearing mice. From (46) with permission.

A, Coronal microSPECT/CT image of co-delivery of nanotargeted radiochemotherapeutics of 188Re-DXR-liposome correlated with whole-body autoradiography in C26 colon carcinoma ascites mice. B, Therapeutic efficacy studies of survival curves for mice bearing peritoneal C26 tumor and ascites animal model of passive nanotargeted 188Re-liposome, Lipo-Dox, 188Re-DXR-liposome, and normal saline. From (48) with permission.
The development of a dual-function PET/near-infrared fluorescence (NIRF) molecular probe for the accurate assessment of pharmacokinetics and tumor-targeting efficacy of U87MG human glioblastoma tumor-bearing mice has been reported (11, 34). The amine-functionalized surface of quantum dot (QD) bioconjugated with arginine-glycine-aspartic acid (RGD) peptides and 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid (DOTA) chelators for 64Cu radiolabeled 64Cu-DOTA-QD-RGD nanoconstructs with 90 RGD per QD to target angiogenesis of integrin-αvβ3 PET/NIRF imaging was also illustrated (34). This dual-function nuclear/optical in vivo molecular probe revealed a quantitative targeting ability in deep tumor lesions (34). Dual modality optical and PET imaging of vascular endothelial growth factor receptor (VEGFR) on tumor vasculature using QDs of 64Cu radiolabeled 64Cu-DOTA-QD-VEGF was also investigated (35). The U87MG tumor uptake of active nanotargeted 64Cu-DOTA-QD-VEGF (1.52±0.6 % ID/g, 2.81±0.3 % ID/g, 3.84±0.4 % ID/g, and 4.16±0.5 % ID/g at 1, 4, 16 and 24 h, respectively, post injection) was one percentage injected dose per gram (% ID/g) higher than that passive targeted 64Cu-DOTA-QD (35). Development of a bifunctional polyaspartic acid-coated nanotargeted iron oxide (IO) molecular probe for PET and magnetic resonance imaging (MRI) of tumor integrin-αvβ3 expression was reported; this bifunctional 64Cu-DOTA-IO-RGD nanotargeted molecular imaging approach may allow for earlier tumor detection and may provide insight into the molecular mechanisms of cancer (36).
Selected cancer nanotargeted nuclear imaging agents.
Nanotargeted Radiopharmaceuticals for Tumor Therapeutics
Typically, nanotargeted radiopharmaceuticals have a two-component architecture for passive targeting therapeutics, e.g. a pegylated nanoliposome loaded with radionuclide payloads, and three-component architecture for active targeting therapeutics, such as pegylated nanoliposome bioconjugated with targeting antibody or peptide and encapsulated radionuclide payloads (16, 17). Selected cancer nanotargeted therapeutics are summarized in Table V. An analytical dosimetry study for the use of 131I, 90Y, 188Re, and 67Cu radionuclide labeled liposome for internal radiotherapy has been reported, and the analysis suggested that the optimal liposome system for radiotherapy differs from that for chemotherapy delivery (37). The results of the effective targeting of solid tumors in patients with advanced local cancer by radiolabeled pegylated liposomes support the possibility of the delivery of β-emitting radionuclide loaded pegylated liposome for the treatment of solid tumors, particularly those liposomes in head and neck patients with highest levels of tumor uptake 33.0±15.8 % ID/kg for a tumor volume of 36.2±18.0 cm3 (26).
Bao et al. have developed a method of labeling liposomes with radionuclides using N, N-bis (2-mercaptoethyl)-N',N'-diethylethylenediamine (BMEDA) to post-load 99mTc or 186Re into liposomes (38, 39). In addition to therapy via intravenous administration, the intratumoral and intraoperational therapy were also investigated for the potential use of 186Re-liposomes (40-42). High-resolution SPECT/CT images revealed the intratumoral distribution of therapeutic liposomes and indicated the potential use of 186Re-liposomes for intratumoral therapy (40). Intraoperative passive nanotargeted 186Re-liposome therapy showed excellent tumor suppression and minimal side-effect profile in a head and neck squamous cell carcinoma xenograft positive surgical margin model (41).
Selected cancer nanotargeted therapeutics.
Concomitant chemotherapy and radiotherapy has been illustrated to improve treatment outcome in a range of solid tumors. Pegylated liposome-encapsulation of doxorubicin and cisplatin has been shown to target drugs to tumors, increase therapeutic efficacy and reduce toxicity (43). Trimodal cancer therapy combining antiangiogenesis, chemotherapy and radiotherapy has beneficial effects and is emerging as a clinical antitumor strategy (44). Image-guided and passive nanocarrier-based polymeric nanomedicine for radiotherapy holds significant potential for improving the treatment of advanced solid tumors (45). Biodistribution, pharmacokinetics, and nuclear imaging of passive nanotargeted radio-therapeutics of 111In/188Re-liposome on C26 and HT-29 colon carcinoma-bearing animal models have been studied by our group (28, 46, 47). 111In has γ-rays with 171 keV energy for nuclear imaging and auger electrons with 0.42 MeV energy in the nm tissue penetration range, with specific single tumor cell or small tumor cluster killing effect (as shown in Table II). 188Re has γ-rays with 155 keV energy for nuclear imaging and is a high energy beta emitter with 2.12 MeV energy for nonspecific large tumor cluster killing effect. Both radionuclides can be used in bifunctional nuclear imaging and internal radio-therapeutic applications. Long-circulating pegylated liposomes radiolabeled with 188Re (188Re-liposomes) showed a higher uptake in the tumor as compared with 188Re-BMEDA alone. Passive nanotargeted 188Re-liposomes were found to have a 7.1-fold higher tumor-to-muscle uptake ratio as compared to intravenously administered unencapsulated 188Re-BMEDA in an animal model of C26 murine colon carcinoma solid tumor (46). Biodistribution, pharmacokinetics, nuclear imaging and therapeutic efficacies were investigated for nanotargeted bifunctional radiochemotherapeutics of 111In/188Re-(vinorelbine/doxorubicin, VNB/DXR)-liposomes on colorectal carcinoma of HT-29 and C26 tumor, and ascites-bearing animal models (29, 48-50). The accumulation and localization of passive nanotargeted 188Re-liposomes have been studied in C26 solid-mouse model (Figure 3). The images revealed that 188Re-liposomes remained in the tumor for up to 72 h p.i., while the corresponding images for free 188Re-BMEDA revealed that it could not efficiently accumulate in tumor at 4 h p.i. (46) (Figure 3).
In addition to the diagnostic imaging of 111In/188Re-liposome, additive therapeutic efficacy was observed for the comparative co-delivery radiochemotherapeutics of specific-killing auger electron emitters of 111In-(VNB)-liposomes on HT-29/luc mouse xenografts (29, 49) (Figure 2B), and nonspecific-killing high energy β-emitters of 188Re-DXR-liposomes on C26 ascites animal models (48) (Figure 4). Coronal microSPECT/CT image of 188Re-DXR-liposomes correlated with its whole-body autoradiography image in C26 colon carcinoma ascites in mice is illustrated in Figure 4A. Furthermore, 188Re-DXR-liposomes could provide a beneficial and promising strategy for the delivery of passive nanotargeted bimodality radiochemotherapeutics in the treatment of tumor (48) (Figure 4B). Previous theoretical dosimetry studies have addressed the potential use of radiotherapeutic liposomes for the treatment of tumors via intravenous injection (37, 51, 52). The comparative dosimetric evaluation of nanotargeted 188Re-(DXR)-liposome derived from the biodistribution indicated that the delivery radiation doses were safe and feasible for further clinical translation research from bench to bedside (50). The results for major organ doses for 188Re-(DXR)-liposome revealed that similar doses were received by spleen and liver, but a lower dose was given to kidney, compared to that of 111In-DTPA-octreotide therapy. Lower doses were also received by total body and liver, compared to 111In-DTPA-hEGF radiotherapeutics (0.19 and 0.76 mGy/MBq, respectively). The absorbed doses for spleen, liver, kidney and red marrow in these studies are much lower than those from 90Y-DOTATOC therapy (50).
Targeted α-particle emitters are promising therapeutics for micrometaststic tumors. Enhanced loading of 225Ac and retention of three α-particle-emitting daughters of 225Ac by passively targeted liposomes and actively targeted immunoliposomes have already been established (53-55). Targeted angiogenesis of αvβ3 and VEGFR2 with three-component actively nanotargeted radiopharmaceuticals of 90Y-liposome-IA (integrin antagonist) and 90Y-liposome-anti-Flk-1 (mAb) have been reported in the murine melanoma K1735-M2 and colon cancer CT26 animal models (56). The results demonstrated that 90Y-liposome-anti-Flk-1 (mAb) was significantly more efficacious than conventional radioimmunotherapy in the mouse melanoma model (14). Boron neutron capture therapy (BNCT) is a binary approach to cancer therapy based on the nuclear reaction that occurs when 10B is irradiated with thermal neutrons to yield high LET of α-particles and lithium nuclei. These particles have a short range (<10 μm) and deposit their energy within single cells. The efficacy and successful treatment of tumors by BNCT depend on the selective delivery of relatively high amounts of 10B to tumors. Application of passive stealth liposomes and active folate receptor-targeted pamam-dendrimer-entrapped 10B delivery systems have been studied for BNCT in animal models (57, 58). The results of the study of 10B-PEG-liposome through intravenous injection suggested that passively targeted delivery of 10BSH can increase the retention of 10B by tumor cells, causing the suppression of tumor growth in vivo by BNCT (58).
Conclusion and Future Prospects
This review article briefly summarizes the recent research on tumor nanotargeted diagnostic and therapeutic radiopharmaceuticals, which is a potential field of novel cancer drug development and application. As compared to conventional targeted radionuclide therapy or radioimmunotherapy, the use of nanocarriers can allow for the specific multivalent attachment of targeted molecules of antibodies, peptides or ligands to the surface of nanocarriers which can deliver a high payload of radionuclides, chemotherapeutics, and/or imaging agents to achieve multifunctional and multimodality targeting of tumor cells, and can enhance the efficacy and safety of targeted therapy. The simultaneous attainment of preferential location, reduction of immunotoxic effect and avoidance of the sequential biological barriers is a major challenge in passively and actively nanotargeted drug delivery systems.
Several passively and actively nanotargeted radiolabeled nanocarriers have been successfully applied to image and treat tumor models both preclinically and clinically. Future studies should be designed to optimize these novel approaches and extend them to combine potent radionuclides, imaging agents, chemotherapeutics and/or radiosentitizing agents. We have demonstrated that co-delivery of radiochemotherapeutics and simultaneous multifunctional imaging is an advantageous characteristic of nanotargeted radiopharmaceuticals for cancer imaging and therapy. An integrated ‘bench to clinic’ translational approach with good multidiscipline and multiinstitute collaboration between academia, research institutes and industry would accelerate the progression of research into nanotargeted radiopharmaceuticals toward clinical applications for the healthcare of cancer patients.
- Received May 4, 2009.
- Revision received July 15, 2009.
- Accepted July 20, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}