


Abstract
Pseudomyxoma peritonei (PMP) is a clinical condition characterized by diffuse intraabdominal spread of mucinous tumor implants that form on peritoneal surfaces. To complement the efficacy of cytoreductive surgery, an effective cytotoxic drug is required as an intraperitoneal agent for microscopic cytoreduction locoregionally. To develop a model for drug discovery, human pseudomyxoma peritonei tumor implants consisting of a mixture of mucin and epithelial cells were injected into the peritoneal cavity of CBH/rnu/rnu rats. A fixed quantity of tumor (2 ml) was implanted in each of the 9 male rats. Over 90 days, all rats developed PMP indicating that this in vivo animal model may become useful platform in a drug discovery program to allow drug efficacy testing against human PMP.
Pseudomyxoma peritonei (PMP) is a clinical syndrome that is characterised by diffuse spread of intra-abdominal tumor implants that follow from the perforation of a mucinous appendiceal or ovarian neoplasm (1). These mucinous implants form on the parietal and serosal peritoneum and ranges in its viscosity from purely liquid to a semi-solid like texture. The epithelial cells within the mucin proliferate and results in continuous production of mucin. Despite the extensive intraperitoneal spread of this tumor, it rarely invades into organs and almost never metastasizes through the blood stream or lymphatics. This mucinous material remains intra-abdominally and accumulates to eventually cause severe abdominal distension and anorexia from compression of the small bowel, which are the main cause of morbidity and mortality in untreated patients. The intraoperative findings of extensive carcinomatosis with mucinous implants accumulating in the pelvis and subphrenic regions are often daunting to general surgeons (2). Traditional treatments include repeated abdominal lavage of mucin, limited debulking of tumor and systemic chemotherapy (3). However, these treatments are unable to adequately combat the reaccumulation of mucin that characterizes the failure of these treatments.
Over the last two decades, cytoreductive surgery and perioperative intraperitoneal chemotherapy comprising of hyperthermic intraperitoneal chemotherapy (HIPEC) using mitomycin C with or without postoperative intraperitoneal chemotherapy (EPIC) using 5-fluorouracil has emerged to become the standard of care in specialized centers (4, 5). A systematic review reporting the results of this treatment in 10 specialized institutions of 863 patients showed a 5-year survival ranging between 52 to 96% from the time of cytoreductive surgery (6). Ten-year overall survival rates have also been reported to be about 85% (7, 8). The survival outcomes of this combined modality treatment is based largely on the concept of locoregional therapy where extensive surgery to remove the tumor implants together with the administration of heated chemotherapy serves to target microscopic residual disease.
Despite the success of this treatment on prolonging survival, treatment failure is common and is often associated with the grade of the tumor (9). To improve the recurrence-free survival, it is of utmost importance that effective cytotoxic therapy be developed to complement the surgical procedure. This will reduce the need for repeated treatment and the risk of morbidity from subsequent cytoreductive surgeries. Here, we report the outcomes of our efforts at developing an in vivo PMP model from our laboratory's drug discovery program.
Materials and Methods
Animals. Male CBH/rnu/rnu rats (n=9) weighing between 200-250 g were purchased from the Biological Resources Centre of the University of New South Wales and were housed in the PC2 facility at the St. George Hospital. The purchase of the rats and the experimental conduct of this study was approved by the University of New South Wales Animal Ethics Committee (approval no. 06-114B). The animals were kept under specific pathogen-free conditions with free access to autoclaved food and water.
Tumor collection. Three patients with histologically proven PMP consented to retrieval of tumor specimen at the time of operation. Mucinous tumors were collected after a laparotomy but before cytoreductive surgery in sterile containers and immediately brought to the animal facility. The tumor was processed under sterile conditions to remove cellular debris such that the remaining tumor extract contained pure mucin with the accompanying epithelial cells.
Tumor implantation. Nude rats were given buprenorphine (0.01 mg/kg) 30 min prior to surgery for pain management. Anaesthesia for surgery was performed using isoflurane. Mini-laparotomy was performed using a lower middle incision of 3 cm. Intraperitoneal tumor inoculation was performed by injecting the patient's tumor specimen under the right lower quadrant of the abdomen (1 mL) and the left lower quadrant of the abdomen (1 mL). Each patient's tumor was implanted in three rats. After the procedure the wound was closed by sutures. Animals were monitored daily for a maximum of 90 days for the development of intraperitoneal tumor.
Post-mortem. At the end of 90 days, all 9 rats underwent a laparotomy with an extended incision from the xiphisternum to the pelvis. Intraabdominal inspection was performed. Tumors in rats were obtained and sent for routine histology analysis. The specimens were fixed in 10% buffered formalin, embedded in paraffin, cut with a microtome to 4 μm and stained with hematoxylin and eosin.
Results
Patients. Tumor specimens were taken from three patients: a 66-year-old female, 72-year-old male, and a 56-year-old male with biopsy-proven pseudomyxoma peritonei arising from an appendiceal mucinous neoplasm during cytoreductive surgery combined with perioperative intraperitoneal chemotherapy. All patients had extensive intraperitoneal mucinous tumor with a score of 22, 24 and 38 on the peritoneal cancer index respectively. All patients underwent a complete cytoreduction (CC0/1). Final histopathological examination of the tumor from all three patients revealed disseminated peritoneal adeno-mucinosis (DPAM).
Gross pathological findings. All 9 rats developed visible evidence of peritoneal mucinous implants. Tumor implants were widespread and the distribution in the peritoneal cavity included the parietal and serosal peritoneum, small bowel mesentry, omentum, paracolic gutters, liver, kidney and spleen. A representative image is shown in Figure 1. Compression of the small bowel by the mucinous tumor was identified in 6 of 9 rats and appeared to be causing a partial bowel obstruction. This had caused diarrhea and weight loss in these rats.
Histopathological findings. Figure 2 is a representative histological display of the mucinous tumor obtained from the rat that is characterized by pools of mucin with strips of cellular tissue of columnar mucinous epithelium with goblet cells on the surface of the bowel mucosa. Accompanying serosal fibrinous material and minimal acute inflammatory response to the pool of mucin is also evident in the hematoxylin and eosin staining at ×10 magnifications.
Discussion
We demonstrate the feasibility of establishing an in vivo model of pseudomyxoma peritonei in immune-compromised nude rats which may serve as a platform for drug discovery whereby intraperitoneal efficacy of various compounds may be subjected to in vivo experimenting after proving its effects in vitro. To our knowledge, this model represents the first of an animal model for DPAM type PMP, which from our institution's experience accounts for almost 70% of all PMP histological subtypes (10).
A previous PMP model was reported by Flatmark et al. (11) using a similar method as reported in this study where human tumor tissue were implanted in the peritoneal cavity of nude mice to establish the orthotopic models. In their study however, peritoneal mucinous carcinomatosis intermediate (PMCA-I) subtype tumor were used. This histological subtype is one of three as described by Ronnett et al., comprising DPAM, PMCA-I and PMCA. DPAM arises from a low-grade appendiceal mucinous tumor and is characterized by widespread peritoneal deposits of abundant pools of extracellular mucin with strips of proliferative mucinous columnar epithelium with little cytologic atypia or mitotic activity. This subtype has been shown to be the most indolent type of PMP and following cytoreductive surgery and perioperative intraperitoneal chemotherapy, long-term survival with 5-year survival rates between 75% to 90% may be reached (10, 7, 8). PMCA consists of abundant mucinous epithelium, forming glands and/or signet ring cells and commonly have severe cytological atypia and are poorly differentiated architecturally. Histological variants with intermediate features of both DPAM and PMCA are termed PMCA-intermediate, which are essentially DPAM but have additional cellular foci containing well differentiated mucinous carcinoma. Clinical outcome studies following treatment of this less common group have been shown to be poorer as compared to patients with DPAM (8, 13-16). Hence, the use of a DPAM model for biological and therapeutic studies in PMP would appear to be more useful as it has been shown to be more common. Targets for therapeutic studies may be achieved through identifying cytotoxic drugs that may target the atypical cells and also dissolve the mucinous component within the tumor.
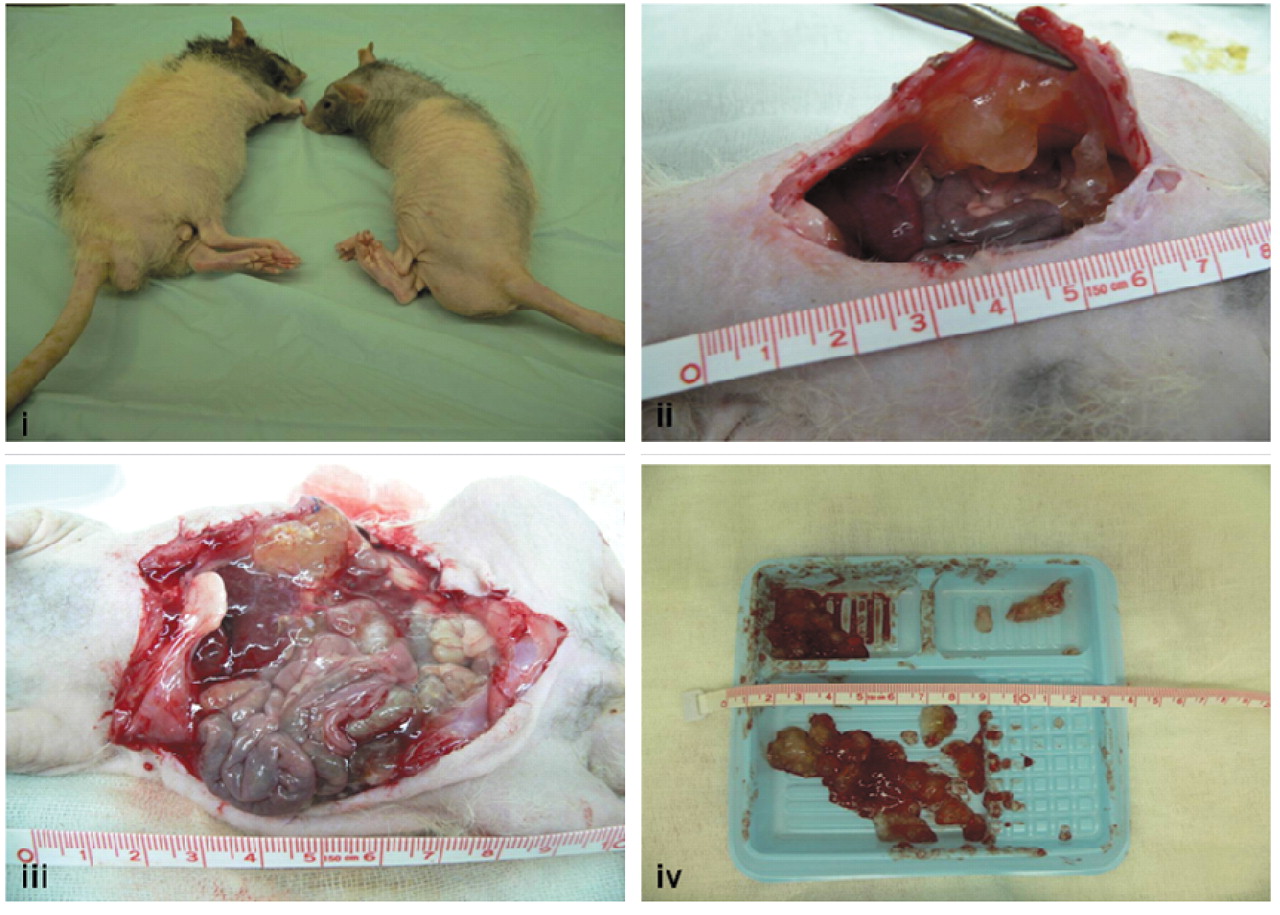
Representative depiction of the development of pseudomyxoma peritonei in the immune-compromised rats.

Section of mucinous PMP located on the bowel. ×10 H&E stain.
Importantly, there is a need to recognise that conventional DNA-damaging cytotoxics, though effective at targeting rapidly dividing cancer cells, have limited efficacy in PMP because the majority of PMP are DPAM containing largely mucin pools and are acellular. Hence, basic research have focused on the mucin component of the tumor, with an emphasis on determining the etiology of mucin gene expression (17) and where enteric bacteria were detected in all PMP tumor specimens, with correlation between the bacterial density and MUC2 expression, hence suggesting the bacteria present in PMP as contributing to the role of mucinous ascites and perhaps promoting carcinogenesis. A study by Bibi et al. (18) of factors affecting tumor invasion and metastasis, in particular cell adhesion-related molecules (N- and E-cadherin, vimentin), showed that PMP demonstrated a higher and specific pattern of adhesion-related protein expression of increased N-cadherin, reduced E-cadherin, and increased vimentin in PMP tumor compared to normal colonic mucosa. This suggests a possible epithelial-mesenchymal transition state that may characterize the distinct non-metastasizing behaviour of PMP. In translation research, expression of mucin gene markers MUC2 and MUC5AC, which were analyzed by in situ hybridization, immunocytochemistry, and digital image analysis showed a distinct overexpression of both MUC2 and MUC5AC in all cases of PMP which may potentially serve as a reliable molecular marker for pseudomyxoma peritonei (19). Analysis of such molecular markers including CK20, CDX-2, and MUC-2 have been shown to correlate with prognosis in prospective series of 102 patients who underwent complete cytoreduction and HIPEC from the National Cancer Institute, Milan, Italy (12).
Progress has been made in basic and translational research for PMP. To advance this field, drug discovery with a focus on targeting the mucinous component of the tumor through dissolution of mucin may improve resectability and reduce the morbidity from treatment of patients with PMP. This may also alleviate the symptoms related to the tumor burden of peritoneal carcinomatosis imposed by specific solid components in mucin. The results of our study appear encouraging and may allow the replication of the model development in larger animals. The tumors resulting from intraperitoneal implantation of PMP behaved similarly to those observed clinically in humans and have a similar histological appearance. The intraabdominal distribution of the tumor paralleled the pattern of spread that has been characteristically described in the clinical syndrome of PMP. This in vivo model will facilitate drug discovery for cure of the mucinous tumor of PMP.
- Received June 30, 2009.
- Accepted July 24, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.