


Abstract
Background/Aim: Low pre-operative lymphocyte–to–monocyte ratio (LMR) is associated with worse outcomes in several malignancies. The aim of this study was to determine the prognostic value of LMR in tongue cancer. Materials and Methods: A total of 103 patients with pathologically-proven tongue cancer were retrospectively analyzed. The peripheral LMR and the ratio of CD8-positive to CD14-positive (CD8+/CD14+) tumor-infiltrating cells were determined by immunohistochemical staining. Receiver operating characteristic curve analysis, log-rank test, and Cox proportional hazards regression models were used for statistical analysis. Results: There was a significant difference in overall survival (OS) between low LMR and high LMR, and low CD8+/CD14+ tumor-infiltrating cells and high CD8+/CD14+ tumor infiltrating cells. For the clinical analysis, multivariate analysis showed that clinical ocular inspection type and low LMR were independent predictors for poor OS. Concerning the immunohistochemical analysis, monocyte count was independent predictor of poor OS. Conclusion: Pre-operative LMR and CD8+/CD14+ tumor-infiltrating cells serve as independent prognostic biomarkers.
Oral cancer, including tongue cancer, is the most common form of head and neck cancer (1). Survival of oral cancer patients mainly depends on the stage of the disease. More than 50% of patients with oral cancer have advanced disease at the time of diagnosis (1, 2). However, the survival rates have improved due to new cytotoxic drugs introduced in the last decade.
Lymphocytes play a fundamental role in most immune system mechanisms aimed at identifying and destroying cancer cells (3). Patients with cancer are known to have abnormalities in T-cell and B-cell counts (4). The microenvironment of oral cancer is characterized by imbalanced cytokine profile, favoring immunosuppressive over stimulatory cytokines (5). It is known that systemic inflammatory responses play important roles in both the development of human cancers and the spread of metastatic tumors (6, 7). Several markers of systemic inflammation, including neutrophil, lymphocyte, monocyte, and platelet count, have been used as prognostic indicators (6, 8). These markers of systemic immune responses can be measured easily, reproducibly, and inexpensively.
The circulating blood lymphocyte–to–monocyte ratio (LMR) is an indicator of systemic inflammation that can be measured by a simple, inexpensive, and reproducible test (9). Recent research has shown that the absolute count of lymphocyte was independently correlated with the survival of patients with several malignancies (9, 10). Other studies demonstrated that a low LMR was associated with worse overall survival (OS) in patients with bladder cancer and pancreatic cancer (11, 12).
Among clinical and experimental studies on head and neck cancer, few have included the measurement of immune responses (13). The failure to develop an accurate tumor model that mimics the host and tumor environment, along with the innate heterogeneity of head and neck cancer, may limit the clinical implications of experimental studies.
The present study was designed to determine the prognostic significance of preoperative LMR in patients with tongue cancer. Furthermore, an immunohistochemical study of LMR was performed to determine the association between the ratio of CD8-positive to CD14-positive (CD8+/CD14+) tumor infiltrating cells around the cancer cells and clinicopathological factors of the patients.
Materials and Methods
Patients and collection of the data. The medical records of 103 patients with pathologically proven tongue cancer, diagnosed between April 2001 and December 2015, were retrospectively analyzed. All patients received surgical treatment for the tongue cancer, but had not received any prior treatment. Data from medical records on routine laboratory measurements of white blood cells performed prior to the onset of treatment including the counts of lymphocytes and monocytes were retrospectively collected. The tumor stage was classified according to the TNM classification of the International Union Against Cancer (14). In addition, data on age at diagnosis, gender, and pretreatment of tumor staging were also collected. The status of patients (alive/dead) at the end of 5 years from the date of diagnosis was retrieved from medical records.
Receiving operating characteristic (ROC) curve analysis to select the most appropriate cut-off point for the counts of LMR was performed to stratify patients at high risk of malignancy-related death. The score at the point with both maximum sensitivity and specificity was selected as the best cut-off value. In survival analysis, OS time was defined as time from diagnosis until death; the follow-up of patients still alive was censored at their latest date of follow-up.
Immunohistochemistry. Paraffin-embedded sections were obtained from biopsy specimens from 103 patients. The histological differentiation of tumors was defined according to the WHO classification (15), and the invasive grade was assessed using the Yamamoto-Kohama (YK) mode of invasion (16). Deparaffinized sections in xylene were soaked in 10 mmol/l citrate buffer (pH 6.0) and placed in an autoclave at 121°C for 5 min for antigen retrieval. Endogenous peroxidase was blocked by incubation with 0.3% H2O2 in methanol for 30 min. Immunohistochemical staining was performed using an Envision system (DAKO, Glostrup, Denmark). The primary antibodies used were anti-CD8 (1:250) and anti-CD14 (1:500) (Abcam, Cambridge, UK). Results were evaluated by calculating the immunohistochemically-positive cells around the cancer cell nest, which was selected at three points at random. CD8+/CD14+ tumor infiltrating cells was calculated from the ratio of lymphocyte counts and monocyte counts, and cut-off points were detected by ROC analysis.
Statistical analysis. Survival curves were generated by the Kaplan–Meier method and were compared using the log-rank test. The relationship between LMR and clinical factors was assessed using Fischer's exact test. The Cox proportional hazards model was applied for univariate and multivariate analysis to identify prognostic factors. All p-values <0.05 were considered statistically significant. All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing Vienna, Austria) (17). More precisely, it is a modified version R commander designed to add statistical functions used in biostatistics.
Results
The median age of patients was 63 years (range 26-92), and the percentage of males and females were 53.8% and 46.2%, respectively. Out of the 103 patients, 87 (84.5%) were diagnosed at early stages (I and II) and 16 (15.5%) patients were at late stages (III and IV). The 5-year OS of the cohort was 84.9%.
The mean value of peripheral blood lymphocytes was 1.79×109 cells/l (range=0.55-4.79×109), and mean value of peripheral blood monocyte was 0.32×109 cells/l (range=0.04-0.88×109). The cut-off value of LMR was determined, and using the LMR cut-off point of 4.29, all patients were divided into either high (LMR≥4.29) or low (LMR<4.29) groups. Thereafter, clinical factors were analyzed against LMR (high LMR vs. low LMR) (Table I). Regarding the clinical stage, as well as the survival rate, including both OS and disease-specific survival, results showed significant differences between high- and low-LMR groups (Table I, Figure 1). Moreover, a univariate analysis of clinical features, including gender, age, alcohol status, smoking, T classification, N classification, clinical stage, clinical ocular inspection type, monocyte count, lymphocyte count, and LMR, and their association with OS was performed (Table II). The analysis revealed that gender, T classification, N classification, clinical stage, clinical ocular inspection type, and LMR were significantly associated with OS. The aforementioned clinical factors were also included in a multivariate analysis, which showed that clinical ocular inspection type and low LMR were independent predictors of poor OS in patients with tongue cancer (Table II).
Correlation between peripheral blood LMR and clinical features.

Kaplan-Meier survival curve. Significant differences in disease-specific survival and overall survival were observed between low lymphocyte–to–monocyte ratio (LMR) and high LMR groups. There was significant difference between low-LMR and high-LMR groups.
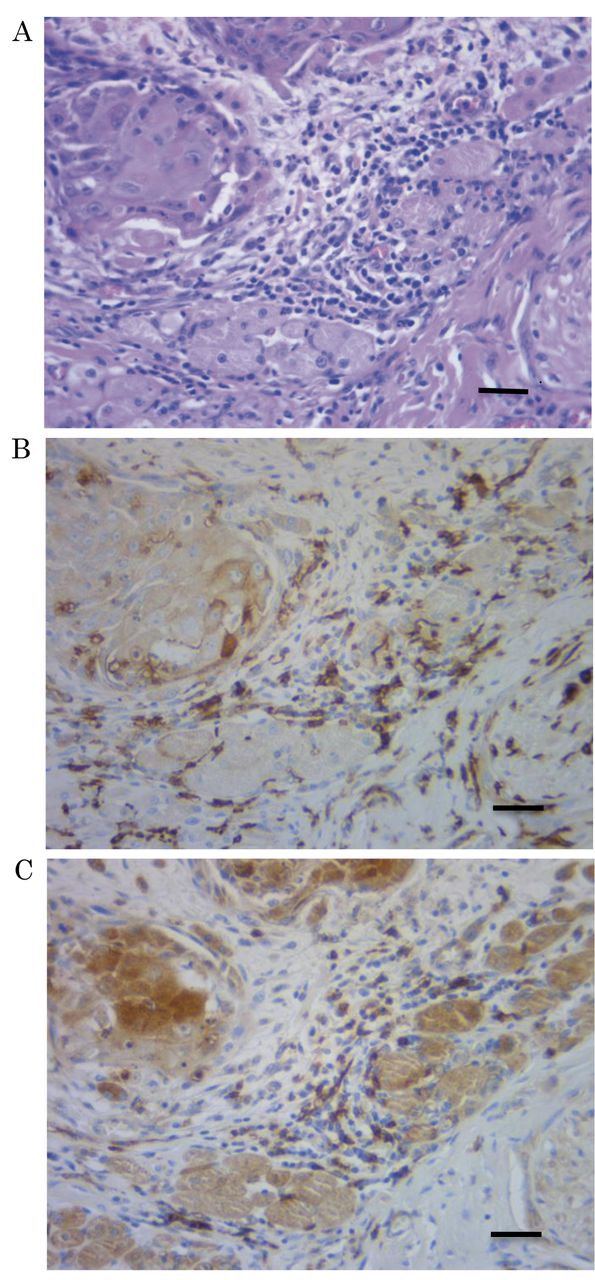
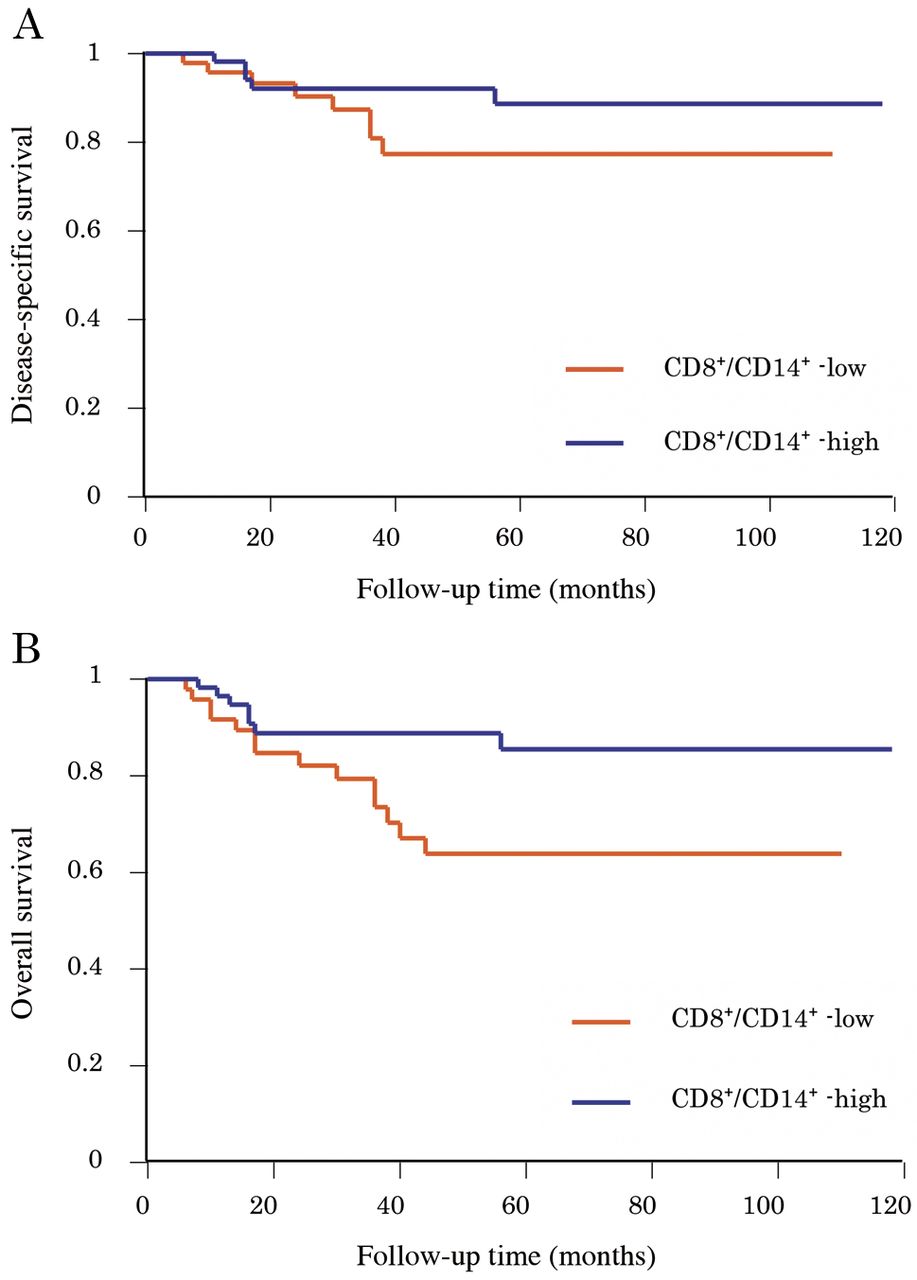
Immunohistochemical findings. The mean labeling index of lymphocytes was 36.3 (range=0-86), and mean labeling index of monocytes was 21.3 (range=3-48) (Figure 2). The cut-off value of CD8+/CD14+ ratio was determined at 1.27 by ROC curves, and using this cut-off point patients were divided into either high- (CD8+/CD14+≥1.27) or low-CD8+/CD14+ (CD8+/CD14+<1.27) groups. Clinicopathological factors were analyzed against CD8+/CD14+ (high CD8+/CD14+ vs. low CD8+/CD14+) (Table III). Significant differences were observed concerning the mode of invasion, perineural invasion, and depth of invasion between low- and high-CD8+/CD14+ groups. In relation to the survival rate, in terms of OS, there was a significant difference between high CD8+/CD14+ and low CD8+/CD14+ (Figure 3).
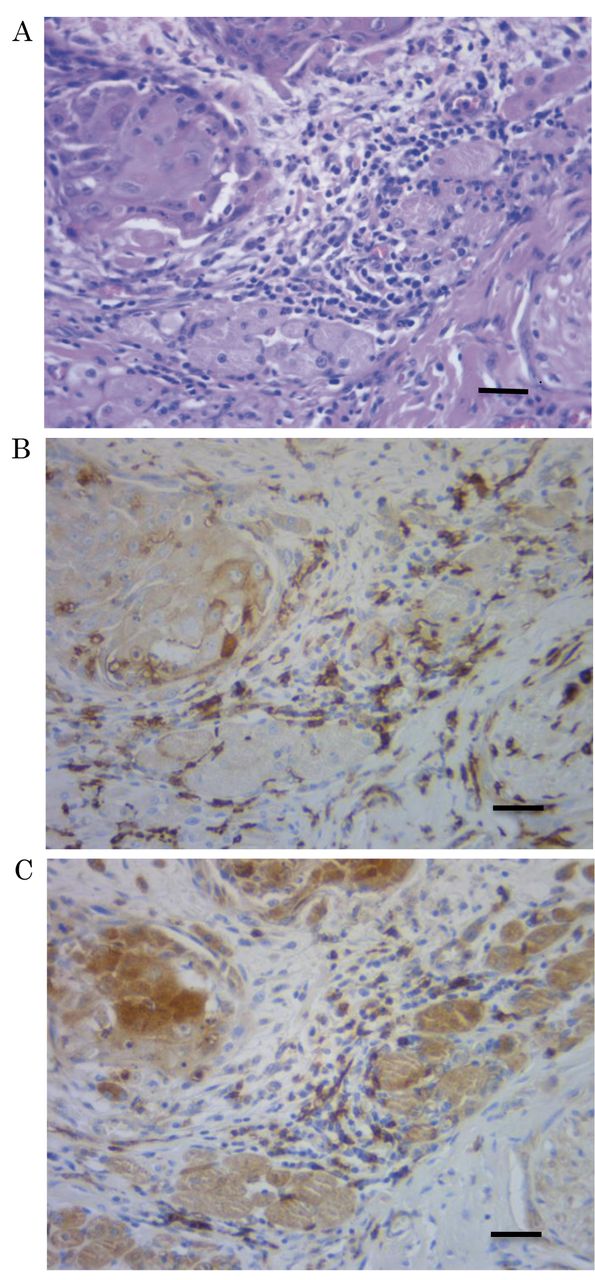
Hematoxylin-eosin staining (HE) and immunohistochemically–determined expression levels of CD8 and CD14. (A: HE, B: CD8, C: CD14) Bar=20 μm.
Univariate and multivariate analysis of clinical factors associated with overall survival.
Univariate and multivariate analyses were performed to examine the association between OS and pathological factors, including histological grade, local relapse, depth of invasion, pathological T classification (pT), pathological N classification (pN), perineural invasion, mode of invasion, late lymph node metastasis, CD8-positive lymphocyte count, CD-14-positive monocyte count, and CD8+/CD14+ (Table IV). Univariate analysis revealed that the depth of invasion, pT, pN, perineural invasion, mode of invasion, late lymph node metastasis, CD14-positive monocyte count, and CD8+/CD14+ were associated with OS. Moreover, according to the multivariate analysis, high monocyte counts were independent predictors for poor OS in patients with tongue cancer (Table IV).
Discussion
Total and differential white blood cell counts have been historically used as a marker of infection and inflammation (9). Recently, systemic inflammation has been recognized to correlate with tumor progression, and inflammatory markers have been reported to be useful for predicting prognosis (18-20). Although a link between inflammation and cancer has been known for more than a century, a strong association between pretreatment peripheral inflammatory cells and prognosis in different kinds of cancer has recently been revealed (21).
LMR is an inflammatory marker that has been reported to correlate with survival in patients with various types of cancer (12, 18-20, 22). However, there have been few reports concerning clinicopathological factors and prognosis in relation to oral cancer. To the best of our knowledge, this is the first study to assess the clinicopathological and prognostic significance of peripheral LMR and CD8+/CD14+ tumor infiltrating cells in oral cancer patients.
Correlation between the CD8-positive to CD14-positive (CD8+/CD14+) tumor-infiltrating cell ratio and pathological features.
Lymphocytes play an important role in the activation of antitumor immune responses, as well as destruction of residual cancer cells and micrometastases after complete resection (23). It has been proposed that tumor-infiltrating lymphocytes of the host significantly contribute to the efficacy of anticancer treatments, since they may lead cancer cells to death by presenting tumor-associated antigens to immune cells, in response to chemoradiation therapy (22, 24). In particularly, higher lymphocyte counts have been reported to predict a better response to operative chemoradiation therapy in rectal cancer (25). Recently, in laryngeal cancer, Dewyer et al. (26) reported that higher concentrations of CD4-positive lymphocytes predicted a response to induction chemotherapy.

Kaplan-Meier survival curve. Significant differences in disease-specific survival and overall survival were present between low ratio of CD8-positive to CD14-positive (CD8+/CD14+) and high CD8+/CD14+ groups. There was a significant difference in overall survival between low- CD8+/CD14+ and high- CD8+/CD14+ groups.
A large amount of accumulated evidence indicates that CD4-positive T cells have a pivotal role in generating and maintaining anti-tumor immune responses through their interactions with cytotoxic T lymphocytes, B lymphocytes, macrophages, and NK cells (3). Therefore, decreased number of lymphocytes is considered to be responsible for an insufficient immunological reaction to the tumor, thus enabling tumor progression and metastasis.
On the other hand, monocytes play an important role in tumor progression and metastasis (6, 27). Monocytes secrete various proinflammatory cytokines, such as interleukin (IL)-1, IL-6, IL-10, and tumor necrosis factor-α, which have been associated with shorter survival and worse prognosis in malignances (28, 29). Furthermore, tumor-associated macrophages, which are derived from circulating monocytes, suppress adaptive immunity and promote angiogenesis, invasion, migration, and tumor growth (30, 31). The study conducted by Tsai et al. showed that the peripheral total white blood cell count, monocyte, and neutrophil to lymphocyte ratio increased with advancement of clinical stage of the oral cancer patients, while the lymphocyte count decreased (32). The monocyte count was also increased in patients with lymph node metastasis. Moreover, the pretreatment circulating monocyte count was an independent prognostic factor for worse oral squamous cell carcinoma-specific survival (32).
Univariate and multivariate analysis of pathological factors associated with overall survival.
As mentioned above, the LMR reflects both the immune status of the host and the degree of tumor progression. Since both a low lymphocyte count and high monocyte count reflect insufficient anti-tumor immunity and an elevated tumor burden, a low LMR is associated with a poorer prognosis. Studies on patients with various types of malignancies, including urothelial (9), bladder (6), colorectal (18), oropharyngeal (25), and breast cancer (33) have reported that low LMR is associated with poor prognosis, which is consistent with the present results on tongue cancer patients.
Ong et al. (13) analyzed the association of peripheral LMR and platelet-to-lymphocyte ratio with the disease outcome in 133 cases of early tongue cancer (T1N0 and T2N0). They concluded that low pretreatment LMR and high platelet-to-lymphocyte ratio predicted poor survival in the studied population (13). The present cohort comprised 87 early tongue cancer cases (84.5%) and our results were in accordance with findings by Ong et al., suggesting close follow-up for the low-LMR group, even after radical resection with clear margin.
Further immunohistochemical study demonstrated that high monocyte counts were independent predictors for poor OS of tongue cancer. In the present study, we used CD14 and CD8 as markers for monocytes and T-lymphocytes, respectively. Most CD14+ cells and CD8+ cells were located in the cancer stroma, whereas only few infiltrated into the cancer cell nests. Nevertheless, high CD14+cells were independent predictors for poor OS.
The monocytes, with high level of CD14 but not CD16, differentiate into M1 macrophages, which play proinflammatory and tumor suppressive roles (34). In contrast, the monocytes, with a high level of CD14 and low CD16, differentiate into M2 macrophage, which play immunosuppressive and tumor-promoting roles (35). Moreover, Zhu et al. (36) showed that the LMR, CD45RO/CD68 ratio, and CD8/CD68 ratio were significantly associated with both overall survival and disease-free survival in esophageal squamous cell carcinoma. Hence, further investigations concerning another markers such as CD16, CD45RO and CD68, are required in tongue cancer.
In consideration of our results, we suggest that LMR and monocytes may be useful to predict prognosis in tongue cancer patients. Grimm et al. showed that neutrophilia, leukocytosis, and monocytosis were associated with advanced tumor stages. Their study also revealed a link between LMR, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio, which might be used in monitoring the clinical course of oral cancer patients (23).
Many studies have declared that circulating hematological parameters might be prognostic factors of oral cancer, but the mechanism underpinning this phenomenon remains unclear (13, 17, 21, 34). Additionally to the analysis of peripheral LMR, herein LMR was immunohistochemically studied as a prognostic factor of tongue cancer. A limitation of this study is that the hematological parameters except LMR have not been determined, hence in the future, we may need to investigate the relationship of other inflammatory markers with the prognosis of tongue cancer.
Conclusion
Pretreatment peripheral and CD8+/CD14+ tumor infiltrating cells were significantly correlated with OS of tongue cancer patients, suggesting that pre-operative LMR should be considered as an independent prognostic biomarker in tongue cancer.
Footnotes
Ethical Approval
This study was approved by the Ethics Committee of the Nagasaki University Graduate School of Biomedical Sciences (approval no. 18101505).
- Received October 16, 2018.
- Revision received November 20, 2018.
- Accepted November 23, 2018.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}