


Abstract
Aim: To evaluate the value of radiosurgery with a rotating gamma-system (RGS) for cerebral cavernomas. Patients and Methods: Seventy-nine patients with symptomatic cerebral cavernomas underwent RGS radiosurgery at the Bach Mai Hospital, Hanoi, Vietnam. Median dose (single fraction) was 20 Gy (range=14-26 Gy). Endpoints included effect on headache, seizures and tumor size. Results: Of 60 patients with headache, 17% had complete response, 82% partial response and 2% stable disease (best response). Of 39 patients with seizures, 31% had complete response, 64% partial response and 5% stable disease. Four patients developed recurrent seizures after 1 year. Regarding the size of cavernoma at 15 months, complete response was observed in 6%, partial response in 75%, stable disease in 15%, progression in 1% and pseudo-progression in 3% of patients. Bleeding within 2 years after RGS radiosurgery occurred in only five patients (6%). RGS dose had no significant impact on outcomes. Conclusion: RGS radiosurgery provided very high rates of symptom relief in patients with cerebral cavernomas.
- Cerebral cavernoma
- radiosurgery
- Rotating-Gamma System
- headache
- seizures
- symptom relief
- cavernous hemangioma
- cavernous angioma
Cerebral cavernomas are cavernous malformations of the vascular bed (1). These tumors account for about 10-25% of all cerebrovascular malformations (2). In the general population, the incidence of cerebral cavernomas is less than 1%. About 75% of such lesions are located supra-tentorially and are often associated with headache and seizures. Intracerebral bleeding is also quite common.
At many centers, microsurgical resection is considered standard treatment approach for cerebral cavernomas (2). Optimal clinical outcome requires complete resection of the cavernoma. Subtotal resection is associated with subsequent episodes of bleeding in approximately 40% of cases (2). Therefore, only very experienced neurosurgeons should perform resection of cerebral cavernomas. Moreover, neurosurgical resection cannot be recommended for lesions in the brainstem or other eloquent areas of the brain, since it may result in significant morbidity. For these patients, stereotactic radiosurgery represents a reasonable alternative. Several studies have shown that radiosurgery is safe and effective for lesions not amenable to neurosurgery (3).
Several types of radiosurgery are available for the treatment of cerebral cavernomas, including mainly linear accelerator-based radiosurgery and gamma-ray based radiosurgery techniques (1, 4-6). Currently, two different gamma-ray based systems are available. The classic Gamma-Knife consists of 201 concentric cobalt-60 sources and has been used since 1968 for intracerebral lesions (7). About 30 years later, the Rotating Gamma System (RGS) system was introduced (8). This device combines features of both the traditional Gamma-Knife and linear accelerator-based radiosurgery. Our present study is the second study evaluating the role of RGS-radiosurgery for the cerebral cavernomas.
Patients and Methods
Seventy-nine patients underwent radiosurgery for a supra-tentorial cavernoma with RGS at the Nuclear Medicine and Oncology Center of the Bach Mai Hospital in Hanoi, Vietnam, between July, 2007 and May, 2015. The median age of these patients was 34 years (range=8-79 years). Thirty-nine patients were female, and 40 patients were male. The tumor was in the following lobes: temporal in 33 patients, frontal in 20, occipital in nine, parietal in 9 patients and other sites in eight. In all 79 patients, the cavernoma bled, acutely in two patients, subacutely in 69 patients and chronically in eight. Prior to RGS irradiation, 60 patients had significant headache, and 39 had significant seizures.
Subgroup analysis: Response rates related to different doses of Rotating Gamma-System radiosurgery (<20 Gy vs. 20 Gy vs. >20 Gy). Complete response was defined as complete relief of symptoms or complete disappearance of the cavernoma. Overall response was defined as complete or partial symptom relief or decrease of the cavernoma in size. p-Values were calculated with the Chi-square test.
Irradiation was performed as radiosurgery with a RGS (Gamma ART 6000; American Radiosurgery, San Diego, CA, USA). The median dose was 20 Gy (range=14-26 Gy) and was administered as a single fraction. The dose was prescribed to the outer margin of the tumor representing the 50% isodose.
The major endpoint was best response with respect to relief of clinical symptoms, namely headache and seizures, during the follow-up period of 15 months following irradiation. When compared to symptoms at baseline prior to RGS irradiation, response was either complete (complete relief of symptoms), partial (partial relief of symptoms), stable disease (no change of symptoms) or progressive disease (increase of symptoms). Additional investigated endpoints included symptom relief at 15 months following RGS irradiation, the impact of the RGS irradiation on the size of the cavernoma at 15 months following irradiation (complete response, partial response, stable disease or progressive disease), assessed with magnetic resonance imaging (MRI) and bleeding within 2 years after RGS radiosurgery. The average time of follow-up was 54.9 (±21.9) months.
Results
Of the 60 patients who complained about significant headache prior to RGS irradiation, 10 patients (17%) had a complete response, 49 (82%) a partial response and one patient (2%) had stable disease, respectively, as best response during the period of follow-up (Figure 1). At 15 months following RGS irradiation, a complete response was found in five patients (8%), a partial response in 53 (88%) and stable disease in two (3%), respectively (Figure 2).
Of the 39 patients who experienced seizures prior to irradiation, 12 (31%) had a complete response, 25 (64%) a partial response and two (5%) stable disease, respectively, as best response during the period of follow-up (Figure 3). At 15 months following RGS irradiation, a complete response was found in eight patients (21%), a partial response in 23 (59%) and stable disease in four (10%), respectively (Figure 4). In addition, four patients (10%) developed recurrent seizures after an initial post-treatment seizure-free interval.
With respect to the effect of the RGS irradiation on the size of the lesions at 15 months, a complete response was observed in five out of the 79 patients (6%), a partial response (median decrease in size by 20%) in 59 (75%) and stable disease in 12 (15%), respectively. In three patients (4%), the lesion appeared larger than prior to RGS irradiation. Since a biopsy was not taken, it remained unclear whether this was true progression or pseudo-progression (radiation necrosis/swelling). In one patient (1%) who developed recurrent clinical symptoms at 12 months following RGS irradiation true progression appeared likely. In the other two patients (3%), the enlargement of the lesion was rated as pseudo-progression, since both patients showed improvement of their symptoms following RGS irradiation. Intracerebral bleeding following RGS radiosurgery occurred in five patients (6%) within 2 years of irradiation. RGS radiosurgery-related acute toxicity was not observed.
In addition, the best response to RGS irradiation regarding headache, seizures and decrease of the cavernoma in size were compared for RGS doses of <20 Gy (N=35), 20 Gy (N=26) and >20 Gy (N=18). The results of this subgroup analysis are summarized in Table I. There were no significant differences in response related to RGS radiation dose.
Discussion
Symptomatic cerebral cavernomas are rare (1, 2). Complete neurosurgical resection is the standard treatment approach at many institutions. However, complete removal of such lesions is often not possible due to their location and risk (2). For these patients, non-invasive radiosurgery is a reasonable option, which is also widely used for the treatment of brain metastases (9-14). Several studies have shown that radiosurgery, either performed as linear accelerator-based or Gamma-Knife radiosurgery is a safe and effective treatment for cavernomas (1, 4-6). The classic Gamma-Knife was introduced in 1968 and linear accelerator-based radiosurgery in the 1980s (7, 15). The RGS technique was introduced in the late 1990s (8) but is available only at a limited number of institutions worldwide.

Headache: Best response after Rotating Gamma-System irradiation.

Headache: Response at 15 months after Rotating Gamma-System irradiation.
The present study is the second study to be reported that evaluated the role of RGS for cerebral cavernomas. RGS radiosurgery resulted in very high rates of symptomatic response of headache or seizures. Overall (complete or partial) response rates were 98% and 95%, respectively. Decrease in cavernoma size was observed in 81% of patients. Bleeding after RGS irradiation occurred in 6% of the patients within 2 years. When comparing different RGS doses, dose had no significant impact on outcomes. In the only other study regarding the role of RGS radiosurgery for cerebral cavernomas (N=45), published in 2015, the cohort received a median dose of 14 Gy (range=10-16 Gy). It reported post-RGS irradiation bleeding rate of 4% within 2 years and decrease in cavernoma size in 38% of patients (16).
Prior to these two studies, several studies using linear accelerator-based radiosurgery or Gamma-Knife radiosurgery had been reported (17-22). Most of these studies reported results regarding the rate of bleeding within 2 years after radiosurgery. In 2010, Lunsford et al. reported a 21% bleeding rate in a series of 103 patients undergoing radiosurgery with a classic Gamma-Knife for a cerebral cavernoma (17). In a subgroup of this study including 68 patients with a brainstem cavernoma, the post-radiosurgery bleeding rate was 16% (6). A similar bleeding rate was reported by Park and Hwuang in 2012 for a series of 21 patients undergoing Gamma-Knife radiosurgery; the annual bleeding rate was 8.2% for the first 2 years (18). In another study including 45 evaluable patients treated with Gamma-Knife radiosurgery, the post-treatment bleeding rate was 7% (19). In 2014, a series of 39 patients who underwent Gamma-Knife radiosurgery for brainstem cavernomas with a median dose of 13 Gy was reported (20); within the first 2 years, bleeding occurred in five patients (13%). In two other studies reporting on the post-radiosurgery bleeding rate, radiosurgery was performed with a linear accelerator (4, 21). The post-radiosurgery bleeding rate in the series of 14 patients reported by Fuetsch et al. was 33% (21). In the study of Sager et al., the rate was considerably lower, namely 6%, after linear accelerator-based radiosurgery with median 15 Gy (range=10-20 Gy) (4). Summarizing the data from the literature regarding the bleeding rate within 2 years after radiosurgery, the bleeding rates after RGS radiosurgery of 4% and 6%, respectively, appear lower than the bleeding rates in most other studies using classic Gamma-Knife radiosurgery or linear accelerator-based radiosurgery, which ranged between 6% and 33% (median=16%) (4, 6, 17-21).

Seizures: Best response after Rotating Gamma-System irradiation.
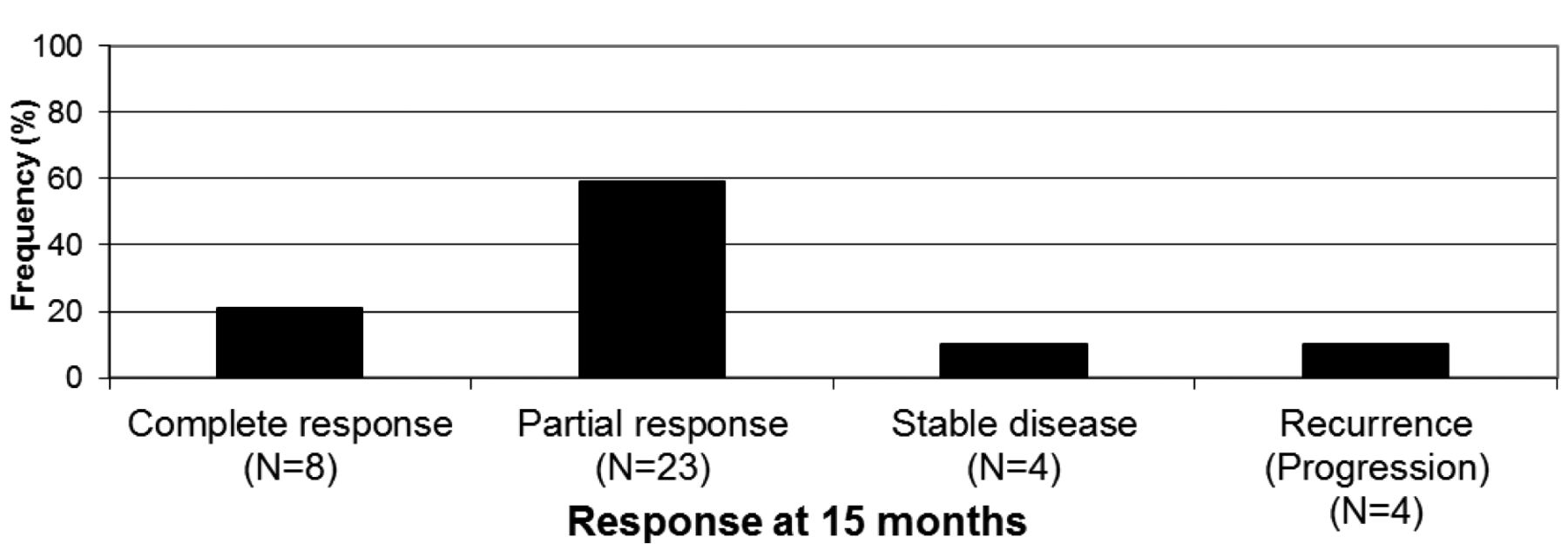
Seizures: Response at 15 months after Rotating Gamma-System irradiation.
In the studies from the literature, data regarding the other investigated endpoints from the present study were scarce. In the study of Sager et al. using linear accelerator-based radiosurgery, symptom relief (overall response) was observed in 64% of patients with headache and 55% of patients with seizures, (4). Liscak et al. reported symptom relief of seizures in 45% of a large series of 112 patients after Gamma-Knife radiosurgery with a median of 16 Gy (22). Decrease of the size of the cavernomas was observed in 53% of the patients. In the other study using RGS those if radiosurgery, decrease in size was observed in 38% of the cavernomas (16). Thus, the overall response rates observed in our present study were higher than those of other studies, revealing RGS radiosurgery to be an effective treatment for cerebral cavernomas. When comparing the results of the studies on radiosurgery of cerebral cavernomas, one should be aware that these studies were retrospective in nature and at risk of including hidden selection biases. However, cerebral cavernomas are uncommon and prospective studies are not expected soon.
In summary, this study found that RGS radiosurgery can provide high rates of symptom relief and decrease in tumor size of cerebral cavernomas. Thus, RGS radiosurgery represents a reasonable alternative for these lesions, if complete surgical removal is not possible.
Footnotes
Conflicts of Interest
On behalf of all Authors, the corresponding author states that there is no conflict of interest related to this study.
- Received May 2, 2017.
- Revision received May 12, 2017.
- Accepted May 16, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.