


Abstract
Background/Aim: This study was designed to evaluate the clinical significance of the C-reactive protein-to-albumin ratio (CAR) in patients with rectal cancer undergoing preoperative chemoradiotherapy (CRT) followed by surgery. Patients and Methods: This retrospective study evaluated the correlation between CAR and prognosis in 115 patients with locally advanced rectal cancer. We also carried out subgroup analyses limited to patients with low modified Glasgow prognosis score (mGPS) (score 0) or pathological TNM stage I-II [ypN(−)]. Results: CAR exhibited significant relationships with sex, tumor invasion, recurrence, serum carcinoembryonic antigen, and mGPS. Elevated CAR was an independent prognostic factor for overall survival (OS) and disease-free survival (DFS) among all patients. Elevated CAR also predicted poor OS and DFS in patients with pathological TNM stage I-II [ypN(−)] and low mGPS score. Conclusion: CAR is a promising predictor of survival and recurrence in patients with rectal cancer treated by CRT.
Rectal cancer is one of the most common types of cancer in Japan and western countries. Preoperative chemoradiotherapy (CRT) followed by curative surgery including total mesorectal excision (TME) has been the widely accepted treatment for locally advanced rectal cancer for more than a decade. Many clinical studies have shown that preoperative CRT improves the rate of sphincter preservation and decreases the local recurrence rate (1-4). Nevertheless, postoperative distant metastasis following TME with or without preoperative CRT remains the major cause of rectal cancer-related death (5, 6). It is, therefore, necessary to develop new therapeutic strategies to identify predictors of early disease recurrence and poor prognosis in these patients.
Several studies have investigated postoperative pathological features such as surgical margins, lymph node metastasis, and mucinous histological type as risk factors for local and distant recurrences in rectal cancer patients treated with preoperative CRT (7-10). However, pretreatment serum markers that could predict recurrence and poor prognosis would represent a convenient tool to enhance both preoperative neoadjuvant and postoperative adjuvant chemotherapy strategies.
The systemic inflammatory response (SIR) is known to be associated with poor outcomes in a variety of cancer types (11). The Glasgow Prognostic Score (GPS) is easily calculated based on serum levels of the acute phase proteins C-reactive protein (CRP) and albumin, and McMillan et al. reported that GPS had prognostic value in patients with various types of cancers (12). A high CRP-to-albumin ratio (CAR) was also recently reported to correlate with poor outcomes in patients with acute medical admissions and sepsis (13, 14). CAR is characterized as quantitative, with a continuous value range, and has been reported to be a good prognostic indicator in patients with various malignancies including gastric cancer, hepatocellular carcinoma, colorectal cancer, and esophageal squamous cell carcinoma (15-18). However, to the best of our knowledge, the clinical significance of CAR in patients with rectal cancer undergoing CRT followed by surgery has not yet been fully investigated.
In this study, we evaluated the prognostic value of pretreatment CAR in patients with rectal cancer undergoing CRT followed by surgery. We also evaluated CAR in subgroups of patients with low modified GPS (mGPS) or pathological TNM stage I-II.
Patients and Methods
Patients. We retrospectively analyzed 115 rectal cancer patients who received preoperative CRT followed by TME in Mie University Hospital (Tsu, Japan) between January 2001 and December 2015. The criteria for preoperative CRT were patients aged 80 years or younger with clinical stage I-III based on the International Union Against Cancer TNM classification, with an Eastern Cooperative Oncology Group performance status of 0 or 1. All patients provided written informed consent. The investigations were performed in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Mie University School of Medicine, Mie, Japan.
CRT schedules and surgery. Patients with rectal cancer were treated with short-course (20 Gy in four fractions) or long course (45-50 Gy in 25 fractions) radiotherapy using the four-field approach. All the patients underwent concurrent 5-fluorouracil (5-FU)-based chemotherapy, including 5-FU/leucovorin, tegafur/uracil and S-1 (19, 20). A total of 54 patients received short-course radiotherapy with chemotherapy for 1 week, and the remaining 61 patients received long-course radiotherapy with chemotherapy for 4 weeks. The time interval between preoperative CRT and surgery was 2-3 weeks for short-course and 4-6 weeks for long-course irradiation. Adjuvant 5-FU-based chemotherapy was administered for 6 months to 1 year following surgery.
Laboratory measurements of albumin, CRP, carcinoembryonic antigen (CEA), and carbohydrate antigen 19-9 (CA19-9). Albumin, CRP, CEA, and CA19-9 were analyzed in routine blood tests. Blood samples from each patient were obtained within 1 week prior to CRT. CAR was calculated and patients were divided into two groups using a cut-off value of 0.049. mGPS was determined by allocating one point each for elevated CRP levels (0.5 mg/dl) and hypoalubuminemia (<3.5 g/dl), such that patients with elevated CRP levels and hypoalubuminemia had mGPS 2, patients with just one of these had mGPS 1, and patients with neither had mGPS 0 (12). We divided patients into two subgroups of mGPS 0 and mGPS 1/2. The cut-off values were 5 ng/ml for CEA and 37 U/ml for CA19-9, according to the normal ranges at our institute.
Clinical response and tumor regression after CRT. Clinical response following preoperative CRT was evaluated by barium enema, endoscopy, computed tomography, and magnetic resonance imaging. After resection of the tumor, all specimens were analyzed histopathologically, and pathological TNM classification and staging were determined according to the classification established by the American Joint Committee on Cancer (21). The degree of histopathological tumor regression was defined according to the Guidelines for the Clinical and Pathological studies on Carcinoma of the Colorectum, and was classified into four grades: grade 0, no necrosis or regressive change; grade 1a, 66% vital residual tumor cells (VRTCs); grade 1b, ~33%-66% VRTCs; grade 2, <33% VRTCs; and grade 3, no VRTCs (22). Non-responders were defined as patients with histopathological tumor regression grade 0-1b, and responders as those with grade 2-3.
Statistical analyses. All statistical analyses were performed using JMP version 10 (SAS Institute, Cary, NC, USA). The results ware expressed as median values or mean±standard deviation (SD). Comparisons were performed using non-parametric Mann–Whitney U-tests for continuous variables. Overall survival (OS) and disease-free survival (DFS) curves were analyzed using the Kaplan–Meier method, and differences were examined using log-rank tests. Univariate and multivariate analyses were performed using a Cox proportional hazards model to determine the factors affecting OS and DFS. Parameters with p<0.05 in univariate analysis were used in multivariate analysis. Receiver operating characteristic (ROC) curves were established to determine cut-off values for diagnosis and prognosis by Youden index. All p-values were two-sided and values less than 0.05 were considered statistically significant.
Results
Patient characteristics. A total of 115 patients were enrolled in this study. Their demographic and clinical characteristics are shown in Table I. The median age of the study subjects was 64 years (range=33–83 years), and the male:female ratio was 2.5:1. The pretreatment clinical T stages were cT1 (n=2), cT2 (n=14), cT3 (n=76), and cT4 (n=23). Eighty-three patients (72%) had clinical lymph node metastasis before CRT. Post-CRT pathologic T stages were ypT0 (n=7), ypT1 (n=11), ypT2 (n=33), ypT3 (n=61), and ypT4 (n=3). A total of 38 patients (38%) had lymph node metastasis (ypN1-3). A total of 100 tumors (87%) showed a well- or moderately differentiated adenocarcinoma histology. Five patients (4%) had local recurrence, and 26 patients (23%) had distant recurrence. The historical tumor regression grades were as follows: grade 0 (n=2), grade 1a (n=34), grade 1b (n=37), grade 2 (n=33), and grade 3 (n=8). The median follow-up period was 65 months (range=2-189 months).
Association between pre-CRT CAR and clinicopathological parameters. The correlation between pre-CRT CAR and clinicopathological parameters is shown in Table II. Pre-CRT CAR was significantly associated with sex (p=0.04), pre-CRT tumor invasion (p=004), recurrence (p=0.006), pre-CRT serum CEA (p=0.004), and pre-CRT mGPS (p<0.0001). However, there was no significant association between CAR and tumor regression grade following CRT (p=0.87).
Association between elevated pre-CRT CAR and prognosis in patients with rectal cancer undergoing CRT followed by TME. We determined the cut-off value (<0.049) for CAR according to the ROC curve for survival analysis. Kaplan–Meier analysis showed that patients in the high-CAR group had significantly poorer OS compared with those in the low-CAR group (p<0.0001) (Figure 1a). Univariate analysis for OS identified pathological TNM stage III [ypN(+)] (p=0.0004), venous invasion positive (p=0.036), pre-CRT elevated CEA (p<0.0001), high mGPS (1 or 2) (p=0.04), and elevated CAR (p<0.0001) as risk factors for poor OS. Furthermore, multivariate analysis using Cox proportional hazards models identified pathological TNM stage III [ypN(+)] (hazard ratio (HR) 3.01, 95% confidence interval (CI) 1.23-7.26; p=0.01), pre-CRT elevated CEA (HR 4.06, 95%CI 1.55-13.95; p=0.003), and elevated CAR (HR 6.52, 95%CI 2.12-18.91; p=0.002) as independent risk factors for poor OS (Table III).
Characteristics of patients with rectal cancer who underwent preoperative CRT.
Association between CAR and clinicopathological factors in rectal cancer patients with preoperative CRT.
Association between pre-CRT CAR and recurrence in patients with rectal cancer undergoing CRT followed by TME. We analyzed recurrence using the cut-off value (<0.049) for CAR. Kaplan–Meier analysis showed significantly poorer DFS in the high-CAR compared with the low-CAR group (p<0.0001) (Figure 1b). Univariate analysis for DFS identified pre-CRT TNM stage III (p=0.04), pathological TNM stage III [ypN(+)] (p=0.0001), venous invasion positive (p=0.014), pre-CRT elevated CEA (p<0.0003), and elevated CAR (p<0.0001) as risk factors for poor DFS. Furthermore, multivariate analysis using a Cox proportional hazards model identified pathological TNM stage III [ypN(+)] (HR 4.54, 95%CI 1.86-11.32; p=0.0008), pre-CRT elevated CEA (HR 3.17, 95%CI 1.36-8.71; p=0.006), and elevated CAR (HR 4.98, 95%CI 2.34-11.14; p<0.0001) as independent risk factors for poor DFS (Table IV).
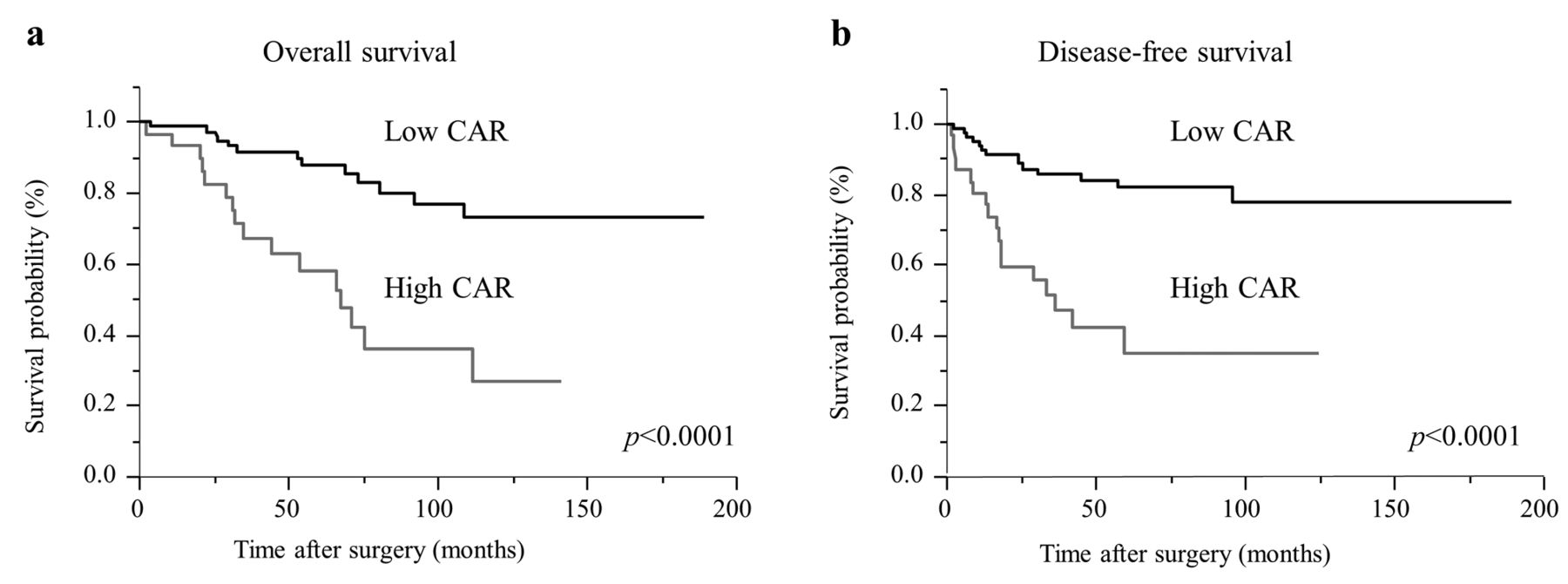
Prognostic impact of CAR prior to CRT in patients with rectal cancer. (a) Kaplan–Meier curves for OS prior to CRT in patients with rectal cancer based on CAR (n=115). OS was significantly lower in patients with high CAR compared to those with low CAR (p<0.0001, log-rank test). (b) DFS analyses based on CAR in patients with rectal cancer (n=115). Patients with high CAR had a significantly poorer prognosis than patients with a CAR below the cut-off value with respect to DFS (p<0.0001, log-rank test). CAR, C-reactive protein-to-albumin ratio.
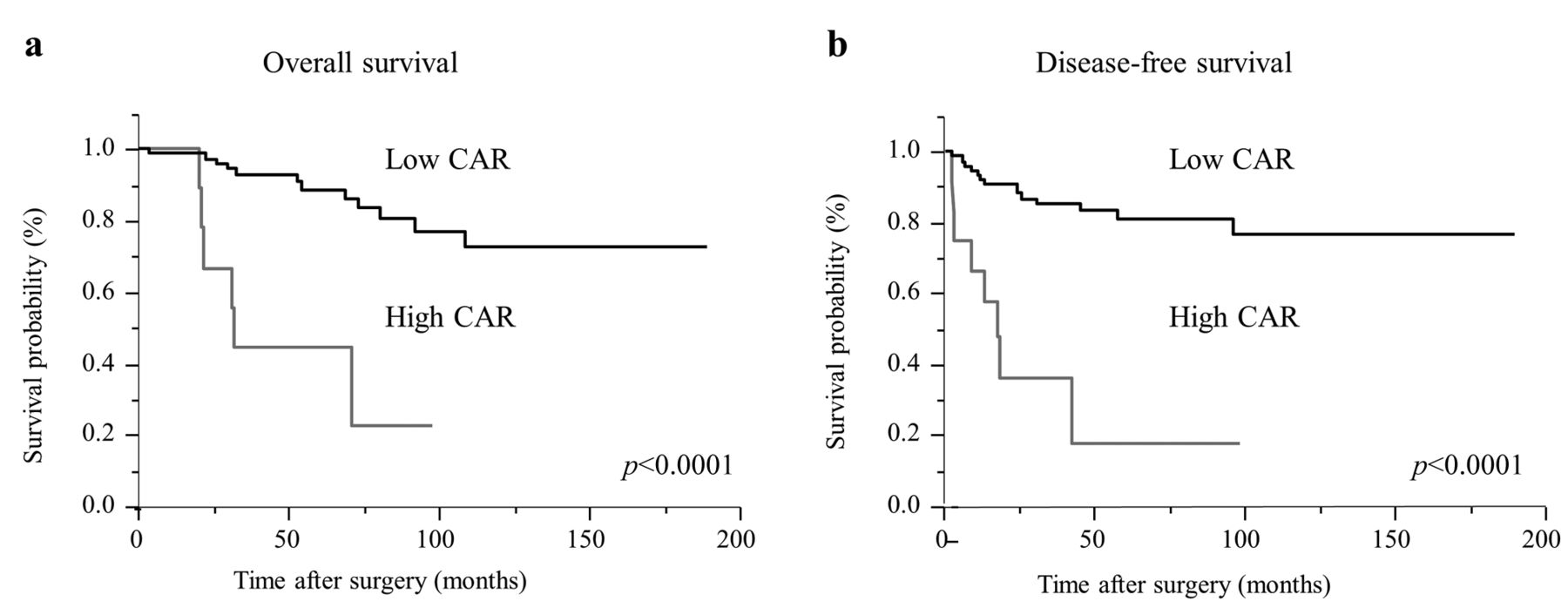
Predictive value of pre-CRT CAR for poor prognosis and recurrence in patients with low mGPS score or pathological TNM stage I-II [ypN(−)]. We conducted subgroup analyses limited to patients with low mGPS score (mGPS 0) or pathological TNM stage I-II [ypN(−)]. Kaplan–Meier analysis of patients with mGPS 0 showed significantly poorer OS and DFS in patients with high CAR compared with low CAR (OS, p<0.0001; DFS, p<0.0001) (Figure 2a and b). Similarly, Kaplan–Meier analysis of pathological TNM stage I-II [ypN(−)] patients also found significantly poorer OS and DFS in the high-CAR compared with the low-CAR group (OS, p<0.0001; DFS, p<0.0001) (Figure 3a, b).
Discussion
The results of the present study indicated that, among patients with rectal cancer undergoing CRT followed by TME, patients with higher pre-CRT CAR had a significantly poorer prognosis and earlier recurrence than those with a lower pre-CRT CAR. Multivariate analyses identified high CAR as an independent predictor of both shorter OS and DFS. Moreover, a high CAR pre-CRT was also associated with a significantly poorer prognosis and earlier recurrence among patients with a mGPS of 0 or ypTNM stage II, according to sub-group analyses. These results suggest that postoperative adjuvant therapy should be considered carefully in patients with higher pre-CRT CAR values.
Recent studies reported a relationship between SIR and prognosis in patients with advanced cancer undergoing surgery (23-25). The SIR is based on tumor-versus-host interactions, which lead to increased levels of cytokines and plays an important role in tumor progression and treatment resistance (26-29). The magnitude and duration of the inflammatory cytokine responses might indirectly reflect the SIR-related clinical characteristics. CRP is an acute-phase protein that is synthesized in the liver, together with cytokines such as interleukin (IL)-1, IL-6, and tumor necrosis factor α (30, 31), and elevated serum levels of CRP have been shown to increase cancer-related production of inflammatory cytokines. Meanwhile, serum albumin is the most commonly used marker of nutritional status, and is also related to chronic inflammation. Malnutrition (hypoalbuminemia) caused by a condition under suppressed production of albumin, results in activation of cytokines such as IL-1, IL-6, and tumor necrotic factor α (32, 33). Low albumin and high CRP, thus, reflect tumor progression, and an increased CAR indicates a poor prognosis. Previous studies demonstrated the significance of lymphocyte count, platelet count, neutrophil/lymphocyte ratio, and fibrinogen as potential pre-CRT biomarkers for predicting prognostic outcomes in patients with rectal cancer treated with CRT followed by TME (34-36). However, to our best knowledge, the current study is the first to investigate the prognostic value of pre-CRT CAR. Collectively, the results of this study suggest that pre-CRT CAR may be a useful biomarker for predicting poor prognosis and early recurrence in patients with rectal cancer undergoing CRT followed by TME.
Univariate and multivariate analyses of predictive factors associated with OS in rectal cancer patients with preoperative CRT.
Univariate and multivariate analyses of predictive factors associated with DFS in rectal cancer patients with preoperative CRT.
mGPS is considered a helpful prognostic marker in various types of cancers. However, despite being based on the same criteria of serum CRP and albumin concentration, CAR and mGPS have different implications. mGPS has the disadvantage of being converted to categorical values, which are thus less able to reflect the patient's condition. Moreover, mGPS classified most patients (approximately 80%) into a good-prognosis group based on a score of 0, indicating a very limited classification ability. In contrast, CAR was able to divide the current patients into two groups with significant differences in survival and recurrence according to Kaplan–Meier analysis. CAR is thus a more accurate and useful prognostic marker than mGPS.
Pathologic stage III and high-risk stage II colorectal cancer require systemic postoperative adjuvant chemotherapy to prevent recurrence, but the value of this approach in patients with locally advanced rectal cancer, especially when the pathologic staging is affected by preoperative CRT, remains unclear. Although the final TNM stages are the same in patients with locally advanced rectal cancer that respond effectively to preoperative CRT (ypT1-2N0) and early rectal cancer (pT1-2N0), the oncological outcomes of the former are significantly poorer in terms of DFS and OS (37). Following effective CRT, pathological lymph node metastasis was diagnosed as going from ypN-positive to - negative, indicating that some patients treated effectively with CRT may be falsely assessed as having good outcomes. Pre-CRT biomarkers that do not depend on this staging system, and which will help identify patients with a poor prognosis or high recurrence risk are therefore needed. The present study clearly demonstrated a relationship between pre-CRT CAR and postoperative recurrence or cancer-specific death in rectal cancer patients with pathologic TNM stage I-II [ypN(−)], and may thus help identify patients more likely to benefit from postoperative chemotherapy.

Kaplan–Meier curves for OS and DFS in rectal cancer patients with mGPS 0 classified according to pre-CRT CAR. (a) OS rates were significantly lower in mGPS 0 patients with elevated CAR compared with patients with lower levels (p<0.0001, log-rank test). (b) DFS rates were significantly lower in mGPS 0 patients with elevated CAR compared with patients with lower levels (p<0.0001, log-rank test).

Kaplan–Meier curves for OS and DFS in ypN(-) rectal cancer patients classified according to pre-CRT CAR. (a) OS rates were significantly lower in ypN(−) patients with elevated CAR compared with patients with lower levels (p=0.0006, log-rank test). (b) DFS rates were significantly lower in ypN(−) rectal cancer patients with elevated CAR compared with patients with lower levels (p<0.0001, log-rank test).
This study had some limitations. First, the total numbers of patients and especially those with recurrences were small, and the study design was retrospective. Second, patients underwent different neoadjuvant radiation regimens with different time intervals between pretreatment and surgery. Further studies in a larger population, with longer follow-up and standardized pretreatments are needed to validate these results.
Conclusion
Pre-CRT CAR can be calculated from routine blood tests without the need for special techniques or expertise and may represent a significant independent biomarker of recurrence or poor prognosis in patients with advanced rectal cancer undergoing CRT followed by TME.
- Received July 24, 2017.
- Revision received August 2, 2017.
- Accepted August 11, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Impact of Nutrition and Inflammation Assessment Tools in Colorectal Cancer Treatment
- Relationship Between C-reactive Protein-to-albumin Ratio Before and After Bowel Decompression and Prognosis in Acute Malignant Large Bowel Obstruction
- Can D3 Lymph Node Dissection for Patients With Colon Cancer With a Poor C-Reactive Protein/Albumin Ratio Improve Survival Outcomes?
- A Matched-Pair Study Comparing Surgery Plus Neoadjuvant Radio-Chemotherapy and Surgery Alone for High Rectal Cancers
- Role of Neoadjuvant Radio-chemotherapy for the Treatment of High Rectal Cancer
- Prognostic Impact of Inflammation-related Biomarkers on Overall Survival of Patients with Inoperable Malignant Pleural Mesothelioma
- Fibrinogen Levels Are Associated with Lymph Node Involvement and Overall Survival in Gastric Cancer Patients