


Abstract
Background/Aim: Superficial myxofibrosarcoma (MFS) and undifferentiated pleomorphic sarcoma (UPS) are highly associated with infiltrative growth (tail sign) and local recurrence, but the impact of preoperative radiotherapy is uncertain. Patients and Methods: Eight consecutive superficial MFS and 10 superficial UPS cases treated with preoperative radiotherapy and surgery were reviewed. Pathological response, surgical margin and magnetic resonance imaging (MRI) were retrospectively evaluated. Oncological events were reported in a descriptive form. Results: Pathologically, nearly-complete response was observed in six UPS cases. Tail sign was pathologically detected in 13 cases, eight of which remained viable. Among the eight cases with viable tail, three cases, including two with positive margin, locally recurred. No major discrepancy was observed between tail length on pre-treatment T1-weighted post-contrast, fat-saturated MRI and pathological tail length. Conclusion: Tail of superficial MFS and UPS can retain viability even after radiotherapy and cause local recurrence unless they respond to radiotherapy well. Wider resection including the tail on MRI is recommended.
Infiltrative growth or tail sign is frequently observed in superficial myxofibrosarcoma (MFS) and superficial undifferentiated pleomorphic sarcoma (UPS). This growth pattern was first reported in 1999 by Fanburg-Smith et al. (1), where pathological infiltration was observed in 83% of the superficial and 24% of deep malignant fibrous histiocytoma (MFH) cases. Since then, this growth pattern has been also described on magnetic resonance imaging (MRI) (Table I) (2-7). High correlations between the radiological and pathological infiltration, ranging from 87% to 100%, have been reported (1, 2).
In recent years, infiltrative growth, or tail sign, has become recognised as a primary risk factor for local recurrence and possibly distant metastasis (1-6). Most studies have emphasised on the importance of preoperative radiological assessment and wider resection, but the impact of radiotherapy (RT) on the tumour and its infiltrative tail as adjuvant therapy remains uncertain (3, 8-10).
Our sarcoma unit has been using preoperative RT for the majority of soft-tissue sarcomas. Despite satisfactory oncologial outcomes of this strategy (11), the controversy concerning the efficacy of RT for infiltrative MFS and UPS has raised the questions of how RT affects the tail pathologically and what kind of margin should be applied for these types of sarcoma in the setting of preoperative RT.
Patients and Methods
This is a comparative case series of superficial MFS and UPS treated with preoperative RT and surgery at a single institution from 2005 to 2014. All patient medical records, glass slides of resection specimens and MRI were retrospectively reviewed. Institutional Review Board approval of this study was obtained prior to the study (HREC-A: QA 104/14).
Patients were identified from the Institutional Connective Tissue Tumour database. Inclusion criteria were superficial sarcomas, diagnosed as malignant fibrous histiocytoma (MFH), MFS or UPS that were surgically treated after preoperative RT but without chemotherapy. Cases referred after excision or those excised without RT were not included. A total of 18 consecutive (eight of MFS and 10 of UPS) cases were included in this study.
The definitions of ‘infiltrative growth’ or ‘tail sign’ of soft-tissue sarcomas in previous studies.
The 18 cases included 11 females and seven males aged 41-88 (mean=68.4) years old, with 15-86 (mean=50.5) months of follow-up. Pathological diagnosis was determined according to the World Health Organization classification in 2013 (12). There were one low-, one intermediate- and 16 high-grade sarcomas according to the French Federation Nationale des Centres de Lutte Contre le Cancer grading system (13).
Preoperative RT consisted of external beam 50.4 Gy, in divided doses over 28 sessions, to the planning target volume (PTV). The gross tumour volume (GTV) was determined by MRI and computed tomography (CT). The clinical target volume (CTV) was defined as GTV plus 3 cm of grossly uninvolved tissue but at risk proximally, distally, medially or laterally. The radial margin included the intact fascial boundary (Figure 1A). The PTV was defined as CTV plus 1 cm. A verification port film was performed weekly over the period of RT.
Three to 8 weeks after the completion of preoperative RT, definitive surgery was performed. The tumour was excised with at least 2 cm of horizontal normal tissue from the proximal, distal, medial, and lateral ends of the palpable tumour mass and one layer of normal tissue in the radial plane. However, we also intended to include the whole abnormal signal area on pre-RT MRI, whether on T2, short tau-inversion recovery (STIR) or post-contrast T1 images, in the resection field (Figure 1B).
Glass slides of all the cases were reviewed by two board-certified Pathologists (JS and LJ). Firstly, overall response was scaled using the percentage of non-viable area, fibrosis or necrosis, on glass slides. Cases with ≥95% non-viable area was regarded as nearly-complete response (CR) to RT as reported in some literature (14-16). The pathological response in the peripheral area was graded as non-viable cell or no tail growth (−), possibly viable without mitotic features or similar morphological appearance to initial biopsy before RT (±), or viable (+). In this study, any cells having nuclei with uptake of haematoxylin stain were considered as viable or possibly viable. The presence of mitosis was regarded as an indicator of viability in this study (17).
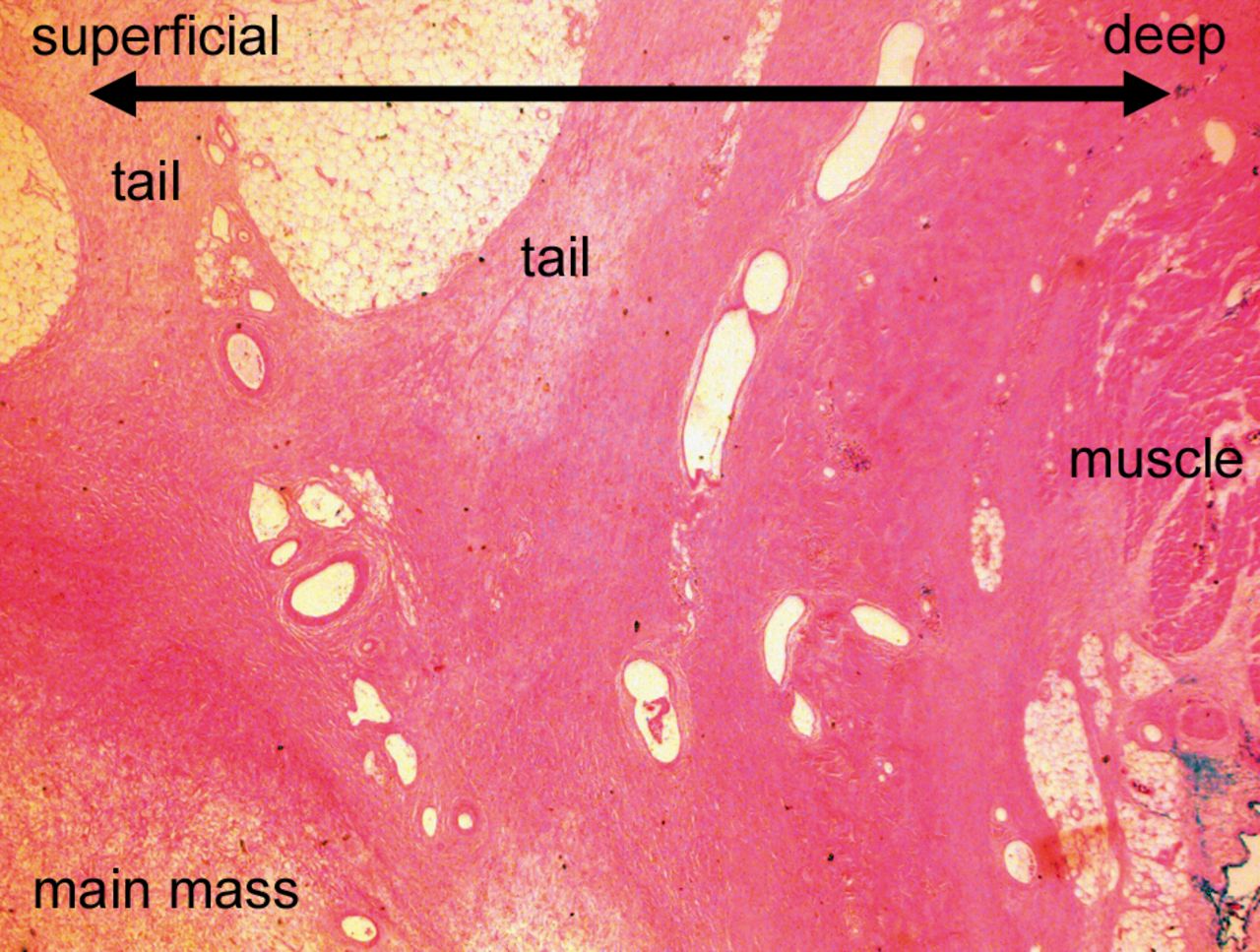
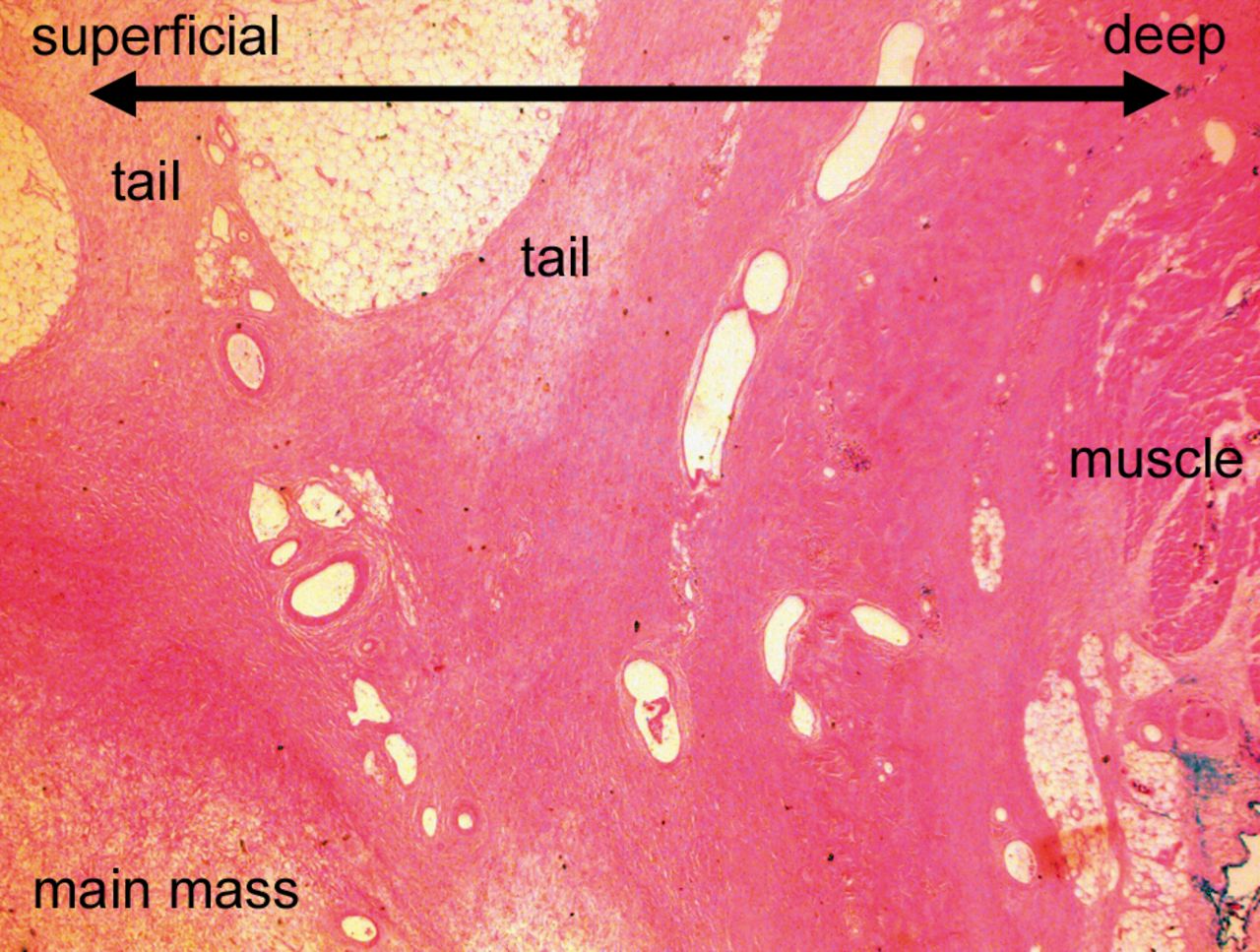
Surgical margins were classified according to the R classification (18) as being R0, microscopically negative margin; R1, macroscopically negative but microscopically positive margin; or R2, both macroscopically and microscopically incomplete margin. Pathological tail length was defined as the maximum length of viable or possibly viable tail on glass slides (Figure 2C).
MR images were reviewed by a board-certified Radiologist (MP), regarding the tail sign (positive or negative) and the length of radiologic tail on pre-RT and post-RT MRI (radiologic tail length), corresponding to the maximum pathological tail on glass slides. Tail sign was defined as tapering tumour extension onto a fascial plane or into subcutaneous fat tissue on any sequence of T1 gadolinium-enhanced, fat-saturated, T2 fat-saturated, or STIR, based on the past literature (Table I) (2-7). The radiological tail length was measured on MRI from the edge of the main mass to the end of the tail on the maximal section, axial, sagittal or coronal dimension, using a tool function on the Picture Archiving and Communication System (Figure 2A).
The timing of local recurrence, metastasis, and death was reported in months from the surgery date to the date of event confirmation. All local recurrences and metastases in this study were identified radiologically then confirmed by core needle biopsy or resection.
JMP® version 10 (SAS Institute, Cary, NC, USA) was used for statistical analysis. Two-sided Fisher exact test was used in the comparison of viable tail growth between MFS and UPS. A p-value of 0.05 or less was regarded as statistically significant.
Results
The pathological response and characteristics of 18 cases are summarised in Table II. Six UPS but no MFS cases were classified as nearly-CR (≥95% non-viable area), and the non-viable proportion of the remaining 12 cases ranged from 0% to 90%. Tail, viable or non-viable, was pathologically detected in 13 cases (72%). Five (four of nearly-CR and one with overall non-viable rate of 90%) cases had no viability in the tail (Table III, Figure 3). In contrast, eight (seven MFS and one UPS) cases had viable or possibly viable tumour cells in the tail, with a significantly higher incidence for MFS (7/8 vs. 1/10, p=0.003). Among these eight cases with viable or possibly viable tail growth, one MFS case (case 13, Figure 4) extended over the fascia without nodular formation for more than 70 mm with microscopically positive margin. The remaining seven cases (six MFS and one UPS) had a main mass with tails ranging from 4 to 27 mm (mean=17.5 mm) in length on glass slides. A microscopically positive margin was observed in two MFS cases (cases 4 and 13).
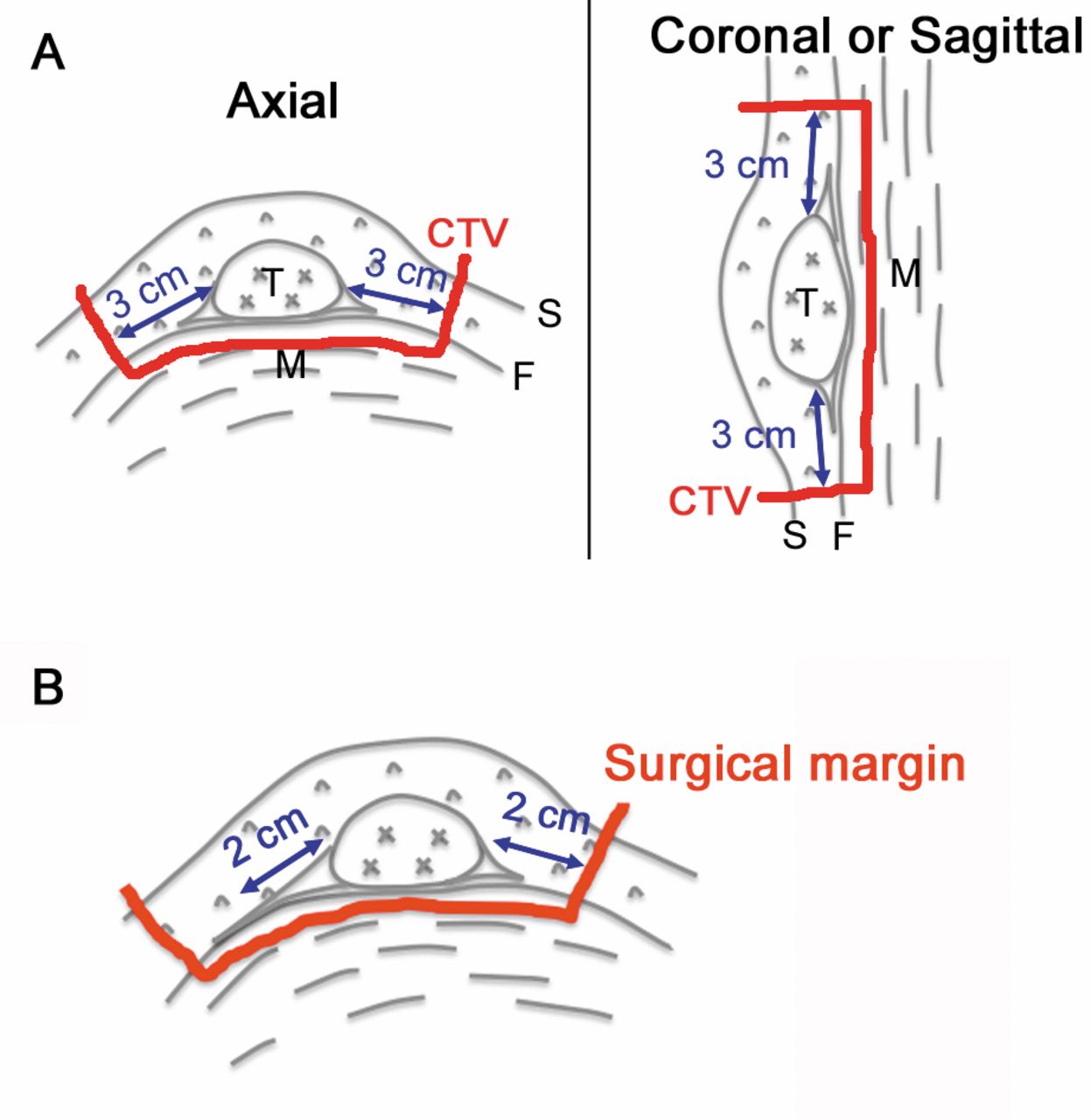
Scheme depicting the radiation field (A) and surgical margin (B) planned for superficial sarcomas with tail sign. CTV: Clinical target volume, S: skin, F: fascia, M: muscle, T: tumour.

A: Myxofibrosarcoma case with poor response to radiotherapy (case 4). Tail sign of pre- (A) and post- (B) radiotherapy post-contrast T1 coronal magnetic resonance imaging corresponding with pathological findings: C: macroscopic view, D: low-power view of inset in C (×4), E: high-power view of inset in D (×40). White arrows (A, C) show radiological and macroscopic tail. Viable tumour cells (#) infiltrated into fascia and subcutaneous fat tissue (D, E).
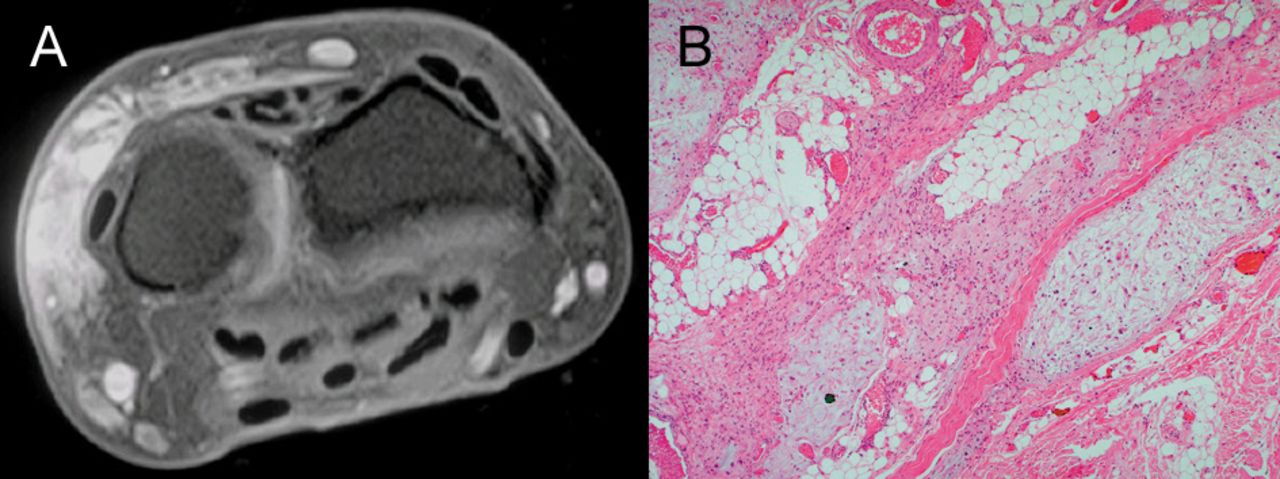
Low-power view (×10) of non-viable tail (case 9). The tail over fascia or into subcutaneous fat layer comprised mainly fibrosis. No viable tumour cells were observed in the tail.
Extensive finger-like infiltration by myxofibrosarcoma observed in case 13. A: T1 post-contrast magnetic resonance imaging after radiotherapy; B: high-power view of resection specimen after radiotherapy (×40).

Extensive abnormal tail sign observed after preoperative radiotherapy on T2-weighted magnetic resonance imaging (MRI) (case 8). A: T1-weighted fat-saturated post-contrast MRI, B: T2-weighted fat-saturated MRI.
Summary of the 18 cases in this study.
Local recurrence occurred in three out of the eight pathologically viable tail cases, including two with microscopically positive margins but in none of the cases without tail (5 cases) or with non-viable tail (5 cases). Tumour cells in the tail of these three recurrent cases appeared similar or mildly altered compared to the biopsy specimens before RT (Figure 2E). Four cases developed lymph node (one case) or distant lung or soft-tissue metastases (four cases) 0-32 months after surgery. The latest oncological status was continuously disease-free for 11 cases, no evidence of disease for three cases, alive with disease for two cases, died of disease for one case and died of other cause for one case. All six nearly-CR cases remained continuously disease-free.
MRI was unavailable for two cases (pre-RT MRI for case 1 and post-RT MRI for case 5). MRI data were not suitable for tail length measurement in two cases because they were scanned and imported from outside MRI films onto the hospital system (pre-RT MRI for case 3 and post-RT MRI for case 1). The length of tail on MRI, corresponding with pathological maximum tail, was 5-36 mm (mean=23.6 mm), on pre-RT T1 post-contrast, fat-saturated MRI in five cases and 7-79 mm (mean=26.0 mm on post-RT T2 fat-saturated MRI in five cases. No major differences between the tail length on glass slides and that on pre-RT T1 post-contrast, fat-saturated MRI were found (Table IV). Post-RT T2 fat-saturated MRI showed significantly wider area of abnormal intensity than pre-RT MRI or pathological tail in two cases (cases 3 and 8), but no viable or possibly viable tumour cells were observed in such an extended area (Figure 5).
Discussion
Infiltrative growth pattern or tail growth, a primary feature of superficial MFS and UPS, is associated with a high risk of positive margins and local recurrence, with 29-67% of inadequate or positive margins and 20-62% of local recurrence reported (1-3). Although preoperative RT is one option for improved local control, the efficacy of RT in this situation is controversial. Iwata et al. concluded that RT for infiltrative MFS and UPS did not reduce the risk of local recurrence (3), while Look Hong et al. (10) and Mutter et al. (8, 9) reported the opposite. In our study, the surgical margin was microscopically positive in 11% (2/18) of the cases, local recurrence occurred in 17% (3/18), tail sign on pre-treatment MRI was observed in 71% (12/17), and pathologically viable or possible viable tail growth after preoperative RT was observed in 44% (8/18). Considering the high pathological infiltration rate of 83% among superficial MFH cases (n=24) previously reported by Fanburg-Smith et al. (1), preoperative RT may have the potential to improve local control of superficial MFS and UPS by eliminating viable tumour cells in some cases. Indeed, tail growth consisting of only fibrosis without tumour cells was observed in five cases (Figure 3).
Tail sign positivity on pre-treatment magnetic resonance imaging (MRI) and tumour viability in tail of 18 cases.
Correlation between pathological and radiological infiltration of eight cases.
The ratio of treatment-induced necrosis or fibrosis, often called the ‘necrosis rate’ in past literature, is a widely accepted tool for pathologically evaluating response of malignant neoplasms to neo-adjuvant therapy (19), but the meaning of total necrosis or complete response of soft-tissue sarcoma after RT is uncertain. Shah et al. recently reported three cases with ≥95% necrosis after RT out of 30 sarcomas and proposed this cut-off figure as a surrogate of better disease control (18). In the current study, six cases (33%) met this criterion and had no local recurrence or metastasis, which may support the hypothesis of Shah et al.'s study.
The current study focused on the tail of superficial MFS and UPS after RT, which can have an important impact on local control. In our study, cases with viable or possibly viable residual tumour cells in the tail were associated with a relatively high ratio of positive margins (25%, 2/8) and local recurrence (38%, 3/8). The two cases with positive margins and subsequent local recurrence at the positive margin strongly indicates that tumour cells in the tail can retain viability after RT. Wide resection safely including the tail should be considered for superficial MFS and UPS.
MRI plays an important role in surgical planning for soft-tissue sarcomas but it is inconclusive whether the pre- or post-RT MRI findings should be used when preoperative RT is given. In our study, there was no major difference between the pathological tail length and that of pre-RT T1 post-contrast enhanced, fat-saturated MRI. By contrast, post-RT MRI may lead to unnecessarily wider excision because it may reflect oedema caused by RT. Therefore, we propose using pre-RT MRI to estimate possible tumour extension from the edge of a palpable mass.
This study has several limitations. Firstly, the number of patients examined was small. This is partly because of the frequent unplanned excision of superficial sarcomas (20). Secondly, the reported pathological tail length may have been underestimated due to possible shrinkage of specimens during formalin fixation and paraffin embedding. Lastly, our study is preliminary for radiological evaluation because of the small study scale, heterogeneous MRI protocols and missing data. However, these limitations are thought not to affect the main message that wider resection may be advisable for superficial MFS and UPS even after RT.
In conclusion, the tail of superficial MFS and UPS may still be viable even after RT and have the potential for seeding local recurrence. Because of this, we propose that wider surgical margins safely including the tail based on pre-RT MRI be chosen for these sarcomas, especially for MFS. Larger studies are required to determine the extent of the wide margin from the area of abnormal intensity, as well as how tumour viability in the tail after RT can be predicted before surgery.
Acknowledgements
The Authors thank Deborah May, Clinical Research Nurse of Department of Orthopaedics at St. Vincent's Hospital Melbourne, and Danielle Jenson, Administrative Support for Bone and Soft-Tissue Clinic at the Peter McCallum Cancer Institute for their assistance with database management.
- Received February 9, 2016.
- Revision received March 25, 2016.
- Accepted March 31, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}