


Abstract
Aim: The current phase II clinical study was conducted to evaluate the efficacy and safety of weekly docetaxel alone, and weekly docetaxel-plus-oxaliplatin, as a second-line chemotherapy in patients with cisplatin-refractory advanced gastric cancer. Patients and Methods: We enrolled patients with histologically confirmed gastric adenocarcinoma whose disease had progressed after cisplatin-based regimens. Patients were randomly assigned to receive docetaxel alone (36 mg/m2, days 1 and 8) or docetaxel (36 mg/m2, days 1 and 8) and oxaliplatin (80 mg/m2, day 1) combination therapy every three weeks. Results: This trial was terminated early due to poor patient accrual rate. From January 2009 to January 2012, a total of 52 patients were enrolled in the current study from six centers: 27 patients in the docetaxel monotherapy arm and 25 patients in the docetaxel/oxaliplatin combination arm. Fifty-two patients were assessable for efficacy, and response rates as follows (response rate: 14.8% in the monotherapy arm, 24.0% in the combination arm; disease control rate: 48.1% in the monotherapy arm, 76.0% in the combination arm. The median progression-free survival was 2.0 (95% confidence interval=1.2-2.9) months in the monotherapy arm and 4.9 (95% confidence interval=3.6-6.6) months in the combination arm (p=0.002). The most common grade 3 or 4 adverse event was neutropenia (14% for monotherapy versus 32% for combination). No treatment-related mortality was observed. Conclusion: Weekly docetaxel and weekly docetaxel-plus-oxalipaltin regimens were found to be well-tolerated and effective as a second-line chemotherapy for patients with advanced gastric cancer.
Despite improvements in survival achieved by early detection and curative surgery, gastric cancer remains one of the most common causes of cancer deaths in Korea (1). Although the prognosis for advanced gastric cancer (AGC) is poor, combination chemotherapy improved the quality of life and overall survival compared to best supportive care in several randomized studies (2-4). Among the various active chemotherapeutic agents, platinum-based combination chemotherapy has been most commonly used, with a high response rate (5, 6). For AGC, many targeted-agents have also been evaluated in international randomized studies, and trastuzumab, an anti-human epidermal growth factor receptor 2 (HER2) monoclonal antibody, has been shown to improve survival in patients with HER-2-positive AGC (7). Although a larger proportion of patients with metastatic or recurrent gastric cancer initially respond to chemotherapy, their disease ultimately progresses. In addition, a significant proportion of patients have primary refractory disease. For these patients, taxanes or irinotecan monotherapy has been most commonly used as second-line chemotherapy. However, there is currently no standard second-line treatment regimen (8).
Docetaxel has demonstrated promising activity as a monotherapy (9), and its combination regimen with oxaliplatin led to a higher response rate with favorable toxicity profile for the treatment of AGC in our previous study (10). However, standard 3-weekly administration of docetaxel in combination with platinum has been associated with a significant incidence of severe myelosuppression, which is more prominent in Asian populations. In addition, previous studies on non-small-cell lung cancer and breast cancer have suggested that weekly administration of docetaxel could reduce hematological toxicity compared to 3-weekly infusion, but retain therapeutic efficacy (11, 12). However, there exist no published data on the efficacy of a combination of weekly docetaxel/oxaliplatin as a second-line treatment for AGC.
Accordingly, the current randomized phase II clinical study was conducted to evaluate the efficacy and safety of weekly docetaxel alone, and of weekly docetaxel-plus-oxaliplatin as a second-line chemotherapy in patients with cisplatin-refractory AGC.
Patients and Methods
Study population. Patients with histologically confirmed metastatic or recurrent gastric adenocarcinoma with at least one measurable lesion were enrolled in the current study. The patients were 19-75 years of age with a performance status of 0-2 on the Eastern Cooperative Oncology Group (ECOG) scale and a life expectancy of more than 12 weeks. In addition, patients were required to have experienced documented, objective radiographic disease progression either during first-line chemotherapy or within six months after the last dose of a cisplatin-based adjuvant chemotherapy regimen. Patients previously exposed to docetaxel or oxaliplatin were excluded. Patients were also required to have adequate organ function. Patients with symptomatic peripheral neuropathy of grade 2 or more, brain metastasis or a history of any other tumor type (except basal skin cell carcinoma or successfully treated in situ cervical carcinoma) and patients with another serious medical condition, known hypersensitivity to atropine, or who were pregnant or breast-feeding were excluded. The Institutional Review Board of each author's institution approved the protocol (KNUH2008047), and written informed consent was obtained from all patients before enrollment.
Study design and treatment. The primary end-point was to evaluate the objective response rate (ORR) of each arm; secondary end-points included determination of progression-free survival (PFS) and overall survival (OS). Patients were stratified by EOCG performance status (0-1 vs. 2) and then randomly assigned to receive weekly monotherapy of docetaxel at 36 mg/m2, or its combination with oxaliplatin at 80 mg/m2. Docetaxel was administered intravenously on days 1 and 8, and oxaliplatin on day 1 every three weeks up to a maximum of nine cycles. Patients whose disease progressed during or after treatment were treated according to physicians' discretion. Docetaxel administration was preceded with 10 mg dexamethasone and antihistamine intravenously to prevent hypersensitivity. Serotonin antagonist or other antiemetics were given as antiemetic prophylaxis before commencing chemotherapy. The prophylactic use of a granulocyte-colony stimulating factor (G-CSF) was not allowed in the first cycle.
Dose modification. The next cycle of treatment was only begun when the absolute neutrophil count was above 1.5×109/l, the platelet count was above 100×109/l, and any other treatment-related toxicities were of grade 1 or less: otherwise, treatment was withheld for up to three weeks. If adverse events did not improve to grade 0 or 1 after two weeks, the patients were excluded from the study. Dose reductions of chemotherapy were made according to pre-specified guidelines based on episodes of febrile neutropenia, grade 4 thrombocytopenia or bleeding episode. In cases of grade 3 or 4 non-hematological toxicity, study drug doses were reduced. Treatment delays of up to three weeks were allowed. Any patient who required a dose reduction continued to receive a reduced dose for the remainder of the study. The drug dose was allowed to be reduced up to 40% of the initially planned dose due to toxicity.
Study assessments. A screening assessment, including a medical history, physical examination, ECG, chest X-ray, and tumor assessment, was conducted within two weeks before starting treatment. Further assessments conducted within seven days before starting treatment included vital signs, ECOG performance status, and laboratory tests. Complete blood counts were performed weekly during the first cycle and every cycle thereafter, and biochemical tests performed before each cycle. Response and progression were evaluated using RECIST criteria (1.1) in this study, which take into account changes only in the largest diameter of the tumor lesions (13). Tumor response assessments were carried out at baseline and every two cycles. Patients were follow-up every three months after the last cycle of chemotherapy until death or loss to follow-up. Safety was assessed by recording adverse events during treatment, and these events were graded according to the National Cancer Institute-Common Toxicity Criteria Version 3.0.
Statistical analysis. Sample size was calculated using Simon's optimum two-stage method with a 80% power to accept the hypothesis and 5% significance to reject the hypothesis. An observed ORR of less than 5% was considered as futile, whereas the study regimen would be regarded as a promising candidate for further evaluation if an ORR of 20% was achieved. Allowing for a follow-up loss rate of 10%, the total sample size of 42 patients per treatment was required. Interim analysis was not planned. All enrolled patients were included in the intention-to-treat analysis of efficacy. Descriptive statistics are reported as proportions and medians. The PFS was calculated from the day of randomization until disease progression, last day of follow-up or death. OS was measured from the first day of randomization until death or the last day of follow-up. Kaplan–Meier estimates were used in the analysis of all time-event variables, and differences between curves were analyzed using the log-rank test. Statistical significance was accepted for p-values of less than 0.05. The statistical data were obtained using an SPSS software package (SPSS 15.0; SPSS Inc., Chicago, IL, USA).
Patient characteristic.
Results
Patients' characteristics. This trial was terminated early due to poor patient accrual rate. From January 2009 to January 2012, a total of 52 patients were enrolled in the study, from six Centers: 27 patients in the docetaxel monotherapy arm and 25 patients in the docetaxel–oxaliplatin combination arm. The median age was 54.0 and 59.0 (range=29-70) years in the monotherapy and combination arms, respectively. Males were dominant in both arms. All patients had received cisplatin-based treatment as first-line chemotherapy. Capecitabine-plus-cisplatin chemotherapy was the most common first-line regimen (55.6% in the monotherapy arm 52.0% in the combination arm). There were no significant differences in patient's characteristics between the two arms (Table I).
Efficacy. Fifty-two patients were evaluated for response. The results of the response rate, as assessed on an intention-to-treat basis, are shown in Table II. The ORR and disease control rate (DCR) of the monotherapy arm was lower than those of the combination arm (ORR=14.8% vs. 24.0%, p=0.40; DCR=48.1% vs. 76.0%, p=0.02). Tumor response and time to progression (TTP) from first-line chemotherapy had no effect on the ORR for the study treatment. At the time of analysis, all patients had died in the monotherapy arm, while three patients (12.0%) were still alive in the combination arm. There was a significant difference in the median PFS between the two arms (2.0 months, 95% confidence interval [CI]=1.2-2.9 months for the monotherapy arm; 4.9 months, 95% CI=3.6-6.6 months for the combination arm; p=0.002) (Figure 1), while the median OS was not different (7.2 months, 95% CI=6.0-8.4 months for the monotherapy arm vs. 8.1 months, 95% CI=7.6-8.6 months for the combination arm; p=0.353) (Figure 2). Eleven patients (40.7%) in the monotherapy arm and 10 (40.0%) in the combination arm received third-line chemotherapy after progression, and the FOLFIRI regimen (infusional 5-fluorouracil plus leucovorin with irinotecan) was commonly used.
Tumor response (intention-to-treat analysis) to therapy for advanced gastric cancer.
Adverse events on therapy for advanced gastric cancer.
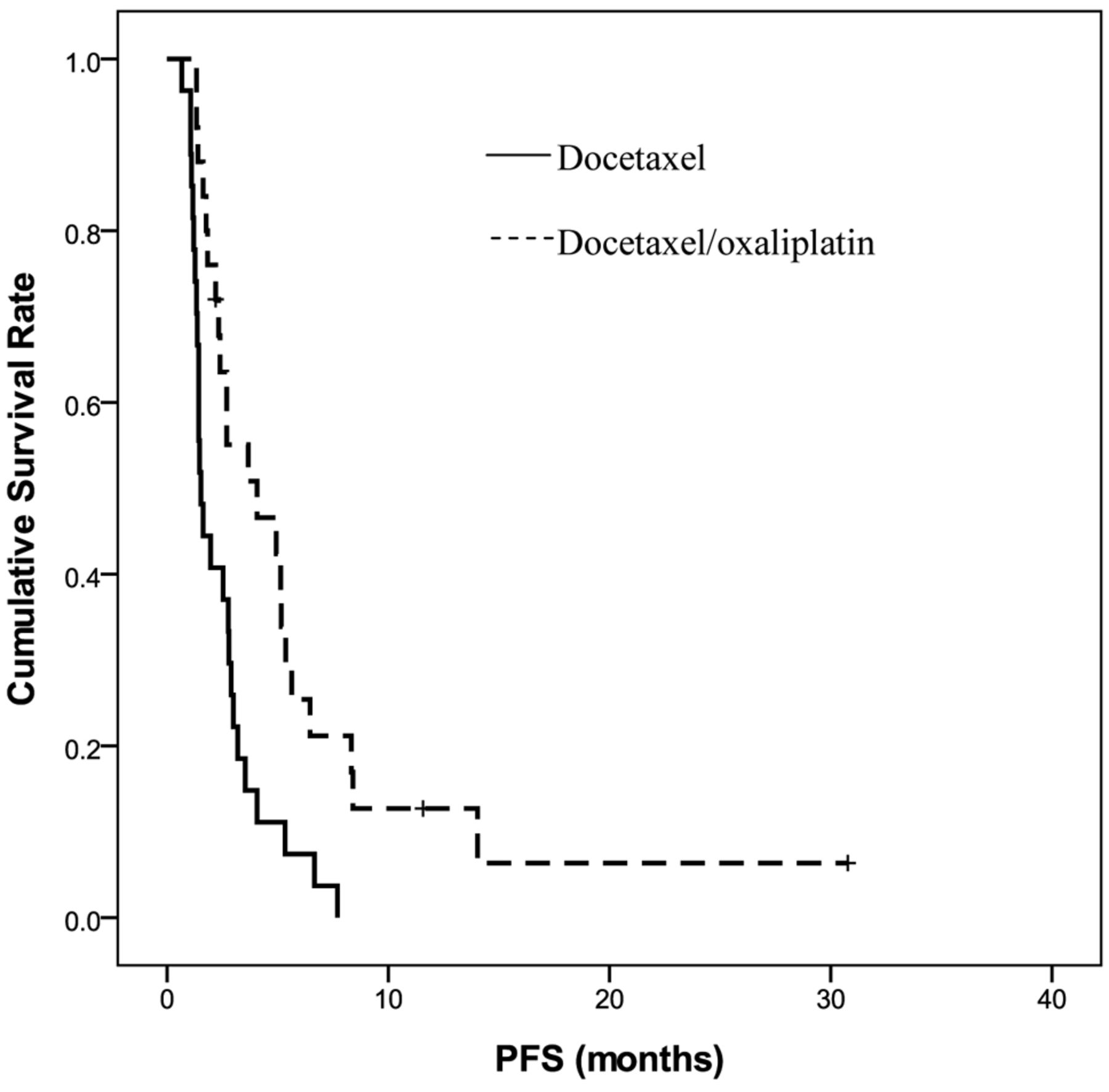
Kaplan–Meier curves for progression-free survival (PFS). The median PFS was 2.0 (95% confidence interval=1.2-2.9) months in docetaxel monotherapy arm and 4.9 (95% confidence interval=3.6-6.6) months in the docetaxel–oxaliplatin combination arm (p=0.002).
Drug delivery and toxicities. The hematological and non-hematological adverse events that occurred during the study are summarized in Table II. A total 81 cycles (median=3, range=1-9) were administered in the docetaxel arm and 103 cycles (median=4, range=2-9) in the combination arm. Treatment delay (10.3% vs. 11.7%) and dose reduction (3.7% vs. 2.2%) were recorded in both arms. Grade 3 or 4 neutropenia occurred in eight patients (32.0%) in the combination arm, while there were more none in the monotherapy arm. Febrile neutropenia developed in five patients (20.0%) in the combination arm. However, all cases were successfully treated with antibiotics and G-CSF. Non-hematological toxicities were generally mild and manageable in both arms. No grade 4 non-hematological toxicity or treatment-related death occurred in this study.
Discussion
In the current study, the weekly docetaxel and docetaxel plus oxaliplatin combination regimen, which can be administered on an outpatient basis, produced meaningful antitumor activity and had safe toxicity profiles in patients with AGC, although this trial was terminated early due to the poor patient accrual rate of 52 patients over a period of three years.
Despite the lack of evidence for any benefit associated with administering second-line chemotherapy, it has been common practice to offer further chemotherapy for patients with AGC after first-line therapy failure. However, three recent randomized clinical trials have demonstrated an OS prolongation with docetaxel or irinotecan as second-line chemotherapy when compared to best supportive care-alone (14-16). Moreover, ramucirumab (a monoclonal antibody against vascular endothelial growth factor receptor 2) also led to a marginal improvement in median OS in the REGARD trial (17).

Kaplan-Meier curves for overall survival (OS). The median OS was 7.2 (95% confidence interval=6.0-8.4) months in the docetaxel monotherapy arm and 8.1 (95% confidence interval=7.6-8.6) months in the docetaxel–oxaliplatin combination arm (p=0.353).
The ORR (14.8%), median PFS (2.0 months), and median OS (7.2 months) following the weekly docetaxel regimen in the present study were comparable with previous results reported for 3-weekly docetaxel or docetaxel-plus-cisplatin regimen as a second-line treatment, where 3-weekly docetaxel chemotherapy achieved a response rate of 16.3% and median TTP of 2.5 months (18), while the combination regimen achieved a response rate and median PFS of 17.1% and 2.2 months, respectively (19). One of the major toxicities related to docetaxel therapy is myelosuppression. Severe chemotherapy-induced neutropenia can also result in treatment-related hospitalization or mortality, thereby compromising the quality of life and increasing medical expenditure. In a previous study by Lee et al. (docetaxel at 75 mg/m 2 at 3-week intervals), grade 3 or 4 neutropenia was observed in 18.4% of patients and febrile neutropenia in 18.4% of patients with AGC after failure of fluorouracil and platinum (18). However, in the current study with a weekly dose of docetaxel (36 mg/m2 on days 1 and 8 every three weeks), grade 3 or 4 neutropenia or febrile neutropenia was not documented. Furthermore, no grade 4 non-hematological toxicity or treatment-related death occurred in this study.
Oxaliplatin, which is commonly used in the treatment of colorectal cancer, has also been shown to be active and safe in the treatment of locally advanced or metastatic gastric cancer (6, 10, 20). Our previous phase II study reported that a docetaxel and oxaliplatin regimen produced a high response rate of 45.2% and median PFS of 5.7 months as a first-line chemotherapy for AGC (10). Furthermore, oxaliplatin was found not to be inferior to cisplatin in a randomized phase III study comparing capecitabine with fluorouracil and oxaliplatin with cisplatin (6). However, cross-resistance is major concern of oxaliplatin administration after failure of cisplatin in the salvage setting for AGC. In a previous in vitro study by Tozawa et al., a cisplatin-resistant cell line showed susceptibility to oxaliplatin, the new-generation platinum agent, and they suggested that this anticancer agent could be used in second-line treatment of patients with cisplatin-resistant gastric cancer (21). Moreover, Kim et al. reported that 5-fluorouracil, leucovorin, and oxaliplatin regimen produced a 21% response rate and TTP of 2.5 months for patients with AGC pretreated with fluoropyrimidine and cisplatin (22). In the current study, the weekly docetaxel plus oxaliplatin combination achieved an ORR of 24.0% and PFS of 4.9 months, which were relatively better than those of weekly docetaxel monotherapy, although the median OS was not statistically different between the two arms (8.1 months vs. 7.2 months). Furthermore, in a previous study by Zhong et al. that employed 3-week docetaxel (60 mg/m2) and oxaliplatin (130 mg/m2) for the second-line treatment of 48 patients with AGC, similar results were recorded (response rate=22.9%, median PFS=4.4 months, median OS=7.2 months) (23). The most common hematological toxicity was neutropenia in the combination arm. Eight patients (32.0%) experienced grade 3 or 4 neutropenia and five patients (20%) were hospitalized due to febrile neutropenia. However, all patients were successfully treated with antibiotics and G-CSF.
In conclusion, the weekly docetaxel and weekly docetaxel-plus-oxalipatin regimens were found to be well-tolerated and effective as a second-line chemotherapy for patients with AGC.
Footnotes
↵* These Authors contributed equally to this study.
Conflicts of Interest
The Authors declare that they have no conflicts of interest with regard to this study.
- Received March 5, 2015.
- Revision received March 13, 2015.
- Accepted March 16, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.