


Abstract
Background /Aim: Studies evaluating the integrity of cell-fee DNA (cfDNA) in colorectal cancer (CRC) have led to inconsistent results. Herein, we analyzed the utility of two different DNA integrity indexes (ACTB384/ACTB106 and ALU247/ALU115) to assess cfDNA fragmentation in Turkish CRC patients. The correlation of circulating nucleosomes (cNUC) with the fragment sizes was also evaluated. Materials and Methods: Seventy two CRC patients and 42 CRC-free control individuals were enrolled in the study. cfDNA was analyzed by quantitative polymerase chain reaction (qPCR). Results: While with ALU247/ALU115there was a small difference between the groups, an approximately 3-fold (median values=0.12 and 0.34) lower integrity was found in the patients using the ACTB384/ACTB106 ratio (p=0.06). The correlation between cNUC and qPCR threshold cycles was much higher for shorter fragments. Conclusion: Lower DNA integrity and the predominance of mononuclesomes in serum reveal high fragmentation of cfDNA in CRC patients.
Despite intensive research and clinical trials, including the newest targeted-drugs, colorectal cancer (CRC) remains one of the leading cancers with respect to its incidence and mortality (1). Nearly one million people worldwide develop CRC each year. Out of these, around 50% die of systemic disease within 5 years of diagnosis (2). Over the last two decades, advances in screening programs, surgical techniques, adjuvant chemotherapy and surveillance programs have improved the survival rates (3). At the molecular level, CRC is a heterogeneous disease. This heterogeneity is associated with differences in disease progression, survival and response to chemotherapeutic agents. Recent advances in genomics, proteomics, transcriptomics and metabolomics have demonstrated that diverse pathways are involved in the development of CRC. Fecal occult blood testing and colonoscopy are two established screening modalities of CRC, while there is no accepted molecular biomarker for CRC screening and early detection. The diagnostic utility of the carcinoembryonic antigen is limited, although it has some impact in the detection of recurrent disease (3).
Plasma and sera of healthy individuals and patients with various disease conditions contain small amounts of non-cell-bound DNA, which is referred to as circulating cell-free DNA (cfDNA) (4). cfDNA is potentially considered a promising source for the development of minimally-invasive diagnostic tests based on tumor-specific DNA markers (5). Several studies have assessed the usefulness of quantitative and qualitative tumor-specific alterations of cfDNA as diagnostic, prognostic and monitoring markers in cancer patients. These markers include quantification of total DNA, DNA strand integrity, frequency of mutations, abnormalities of microsatellite sequences and methylation of specific genes.
cfDNA can exist in the plasma or serum as free, unbound DNA, as histone-bound DNA in the nucleosomes or as DNA packed in the apoptotic bodies (6). DNA fragments released from the tumor cells vary in length (7). Integrity of cfDNA has been widely studied in serum/plasma of patients with various cancers (8-10). Experimental studies with human CRC xenografts have revealed a high fragmentation of tumor-derived plasma DNA (11, 12). Studies using patients' samples, however, have led to inconsistent results. While certain reports (13-15) found increased DNA integrity (e.g. less DNA fragmentation) in CRC patients, others (12, 16) reported a reduced integrity (e.g. higher DNA fragmentation). In a recent study, Mouliere et al. (17) have analyzed cfDNA from CRC patients by atomic-force microscopy and found that it is highly fragmented. Thus, it is obvious that the level of DNA fragmentation has significant impact on the accuracy of the DNA concentration measurement (18) and that selection of different ampliconsizes and the abundance of target sequences can also affect DNA integrity. In the present study, using single- (the ACTB gene) and multiple-copy (ALU elements) sequences we investigated the performance of two different serum DNA integrity indexes (ACTB384/ACTB106 and ALU247/ALU115) to distinguish CRC patients from cancer-free individuals. Additionally, we analyzed circulating nucleosomes (cNUC) and their correlation with the fragment sizes to further evaluate the fragmentation levels of cfDNA.
Association of DNA integrity indexes and cNUC with clinical characteristics.
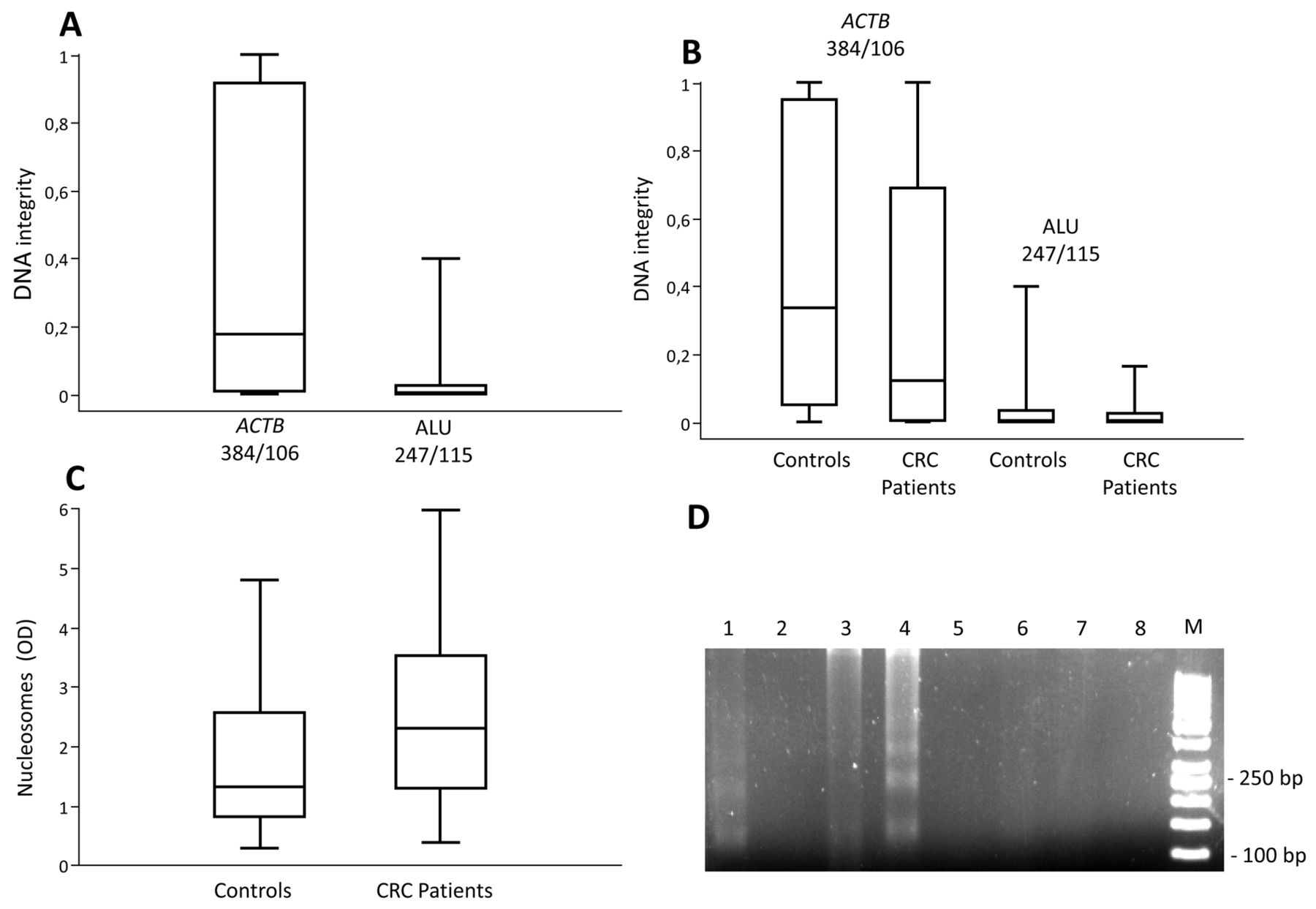
DNA integrity and nucleosome levels in CRC patients and controls. The integrity of cfDNA in serum was calculated by using the ACTB106/ACTB384 and ALU247/ALU115-qPCR ratios in whole study group (A) and in the CRC patients and controls (B). The concentrations of nucleosomes in sera were measured and expressed relatively (C). The results in A-C are presented as the median and interquartile range. Presence of nucleosomal DNA in serum was demonstrated electrophoreticaly (D). Lanes 1-4 include randomly chosen patients' samples, while lanes 5-8 are samples from controls. M, DNA size marker; bp, base pairs.
Materials and Methods
Patient selection. Samples were collected between July 2013 and August 2014 from the Surgical Department of Istanbul Faculty of Medicine. Seventy two patients with CRC and 42 control individuals were enrolled into the study. Venous blood was drawn from the patients prior to surgery or any medical treatment. Patients' demographic and clinopathological characteristics are summarized in Table I. Association of the DNA integrity indexes and cNUC levels with the clinical variables, including age and gender, tumor size, TNM stage, differentiation, metastasis status, venous invasion or the tumor markers, was studied. The control group consisted of individuals who underwent colonoscopy and were verified to be cancer- and polyp-free. The study was approved by the Istanbul Faculty of Medicine Ethics Committee and informed consent was obtained from each participant.
Sample processing. A total of 4 ml of blood samples were collected from the healthy controls and CRC patients. Samples were transferred to an 8 ml gel separator tube and kept at room temperature for coagulation. Subsequently, the samples were centrifuged twice for 10 min at 1,000×g. The samples were processed within 1-4 h after collection to prevent loss of cfDNA. Sera were stored in aliquots at −80°C until use.
Quantitation of circulating nucleosomes (cNUC). Serum concentrations of cNUC were determined using the Cell-death Detection ELISA kit (Roche Diagnostics, Mannheim, Germany) as reported previously (19). Briefly, we applied 20 μl of sera in duplicate and mean absorbance values at 405 nm (reference wavelength approx. 490 nm) were used to calculate the relative serum concentrations.
Extraction of serum DNA. Serum DNA was isolated by phenol/chloroform extraction. Briefly, 200 μl of sera were treated with proteinase K (1.7 mg/ml) and 5% SDS for 1h at 65°C. The solution was heated to 95°C for 10 min to inactivate proteinase K. After adding 300 μl phenol, the mixture was vortexed and centrifuged at 8,000 rpm for 10 min. The supernatant was carefully transferred into a fresh tube. Sodium acetate (0.3 M) and cold ethanol (2.5 vol) were added and the mixture was incubated for 1h at −80°C. cfDNA was collected by centrifugation for 30 min at max. speed, at 4°C, dissolved in 25 μl of 10 mM Tris-HCl, pH 8.5, and was stored at −20°C until use.
Assessment of circulating serum DNA integrity. For the assessment of DNA fragmentation we amplified two different sequences: a single copy sequence from the ACTB gene with fragment sizes of 106 and 384 base pairs (bps) (8) and the abundant ALU sequences with fragment sizes of 115 and 247 bps (20). The quantification was performed by real-time PCR using the SYBR Green Master Mix (Applied Biosystems, Life Sciences, Carlsbad, CA, USA) in accordance with the manufacturer's instructions. The following primer pairs were used: ACTB106 (F: 5’-TCGTGCGTGACATTAAGGAG-3’; R: 5’-GGCAGCTCGTAGCTCTTCTC-3’) and ACTB384 (F: 5’-GCTATCCCTGTACGCCTCTG-3’; R: 5’-AGGAAGGAAGGCTGG AAGAG-3’). ALU115 (F: 5’-CCTGAGG TCAGGAGTTCGAG-3’; R: 5’-CCCGAGTAGCTGGGATTACA-3’) and ALU247 (F: 5’-CCTGAGGTCAGGAGTTCGAG-3’; R: 5’-CCCGAGTAGCTGGG ATTACA-3’). The ACTB106 and ALU115 primers amplify both short and long fragments of DNA, while the ACTB384 and ALU247 primers amplify the long DNA fragments, released mainly from non-apoptotic cells. Real-time PCR was performed in a total volume of 20 μl using 2 μl of template DNA beginning with an incubation at 95°C for 10 min, followed by 40 cycles of 95°C for 30 s, annealing at 60°C for 30 s and extension at 72°C for 30 s in the LightCycler 480 system (Roche). We calculated serum DNA amounts by doing an absolute quantification using serial dilutions of a DNA standard. The integrity of circulating cell-free DNA in serum was determined by calculating the ACTB384/ACTB106 and ALU247/ALU115-qPCR ratios. The results were presented as the median and interquartile range.
Statistical analyses. Correlations between the parameters were calculated by the Spearman's correlation test. Differences between the study groups were determined by the Mann-Whitney U test. Calculations were carried out using the SPSS statistics software (version 21.0) (IBM Corp., Armonk, NY, USA). A p-value lower than 0.05 was considered as the level of statistical significance.
Results
We tested the utility of two different integrity indexes (ACTB384/ACTB106 and ALU247/ALU115) to distinguish CRC patients from the cancer-free controls. Figure 1A depicts the DNA integrity indexes in the whole study group where the integrity index ACTB384/ACTB106 displays a much broader range (0.001 to 1) than the ALU247/ALU115 index (0.001 to 0.4). Values from both indexes did not show a normal distribution so that the median values between the study groups were compared. Consequently, the median value (0.18) using the ACTB384/ACTB106 integrity index was considerably higher than the median value (0.004) of ALU247/ALU115 in the whole study group. However, using both indexes, DNA integrity in the patients was lower than the controls (Figure 1B). For ACTB384/ACTB106 there was a high difference (median values 0.12 vs. 0.34) between patients and controls although the statistical significance was borderline (p=0.06) probably due to the higher standard deviation (0.4) of the values. For ALU247/ALU115 there exists only a small difference (0.03 vs. 0.05, p>0.05.) between the groups. Subsequently, we measured cNUCs levels (Figure 1C). As depicted in the Figure, patients with CRC had higher nucleosome levels (median 2.4) than the control group (median 1.3) (p=0.003). Figure 1D representatively demonstrates the obvious predominance of nucleosomal DNA in patients' sera. Similar to nucleosomes, the patients had higher levels of total serum DNA (median 44 ng/ml measured using ACTB106 as target) than controls (median 33 ng/ml).
We investigated the association of the DNA integrity indexes and cNUC levels with the clinical variables (Table I). We found no correlation between DNA integrity and the clinical variables. In contrast to DNA integrity, the nucleosome levels were higher in sera of patients with distant metastases (p=0.04) indicating high tumor burden.
Finally, we analyzed the correlation between the cNUC levels and fragmentation of cfDNA. To explore this, we analyzed the nucleosome levels and qPCR threshold cycles (Ct) of the short and long ACTB and ALU fragments. The correlation was much higher for the shorter fragments of both ACTB and ALU sequences in the whole study group (Figure 2A and B) and in the patients (Figure 2C and D). These findings confirm high fragmentation of cfDNA in the CRC patients.
Discussion
The integrity of cfDNA has been widely studied in serum/plasma of patients with various malignancies (8-10). However, in CRC, the results are inconsistent. Both reduced (e.g. elevated DNA fragmentation) and increased DNA integrity (e.g. lower DNA fragmentation) have been reported (12-17). It has also been shown that the level of fragmentation does not affect the accuracy of spectrophotometric measurements of DNA concentration, while fluorometric measurements, as well as qPCR, are significantly affected and a decrease in the measured concentration values is observed (18). However, different amplicon sizes and the amount of the target sequences could also affect DNA integrity.
In our study, we assessed cfDNA integrity in sera of CRC patients by utilizing two different DNA integrity indexes (ACTB384/ACTB106 and ALU247/ALU115). We found that the integrity index using ALU247/ALU115 is much lower than the ACTB384/ACTB106. This difference is likely to be a consequence of very frequent presence of small ALU fragments (ALU115) in serum compared to single copy ACTB sequences. This finding confirms that cfDNA quantification by qPCR depends on the length of the amplified target sequence (12).
Using both indexes, we found lower DNA integrity values in CRC patients when compared to cancer-free individuals. While for the ALU247/ALU115 ratio there was a small difference between the groups, an approx. 3-fold (median values=0.12 and 0.34) lower integrity was found in the patients using the ACTB384/ACTB106 ratio. However, this difference did not reach statistical significance (p=0.06) possibly due to the broad range of the values resulting in a high standard deviation. This high variation is likely a result of the rarity of the long amplicon size (384 bp) and differences in its frequency between the samples leading to a broad range of DNA integrity values. Even of borderline significance, lower DNA integrity in CRC samples indicates high DNA fragmentation of serum DNA. Similar to our findings, Thierry et al. have reported predominance of mononucleosome-derived fragments in plasma from animals xenografted with CRC and apoptosis as the source of tumor-derived cfDNA in particular (11). Another recent study found a highly fragmented DNA in plasma of CRC patients where more than 80% of the cfDNA fragments were smaller than 145 bp (17). On the other hand, we found no correlation between the DNA integrity indexes and any clinical variable. However, it is possible that the small number of cases in some subgroups (Table I) and the predominance of small fragments for all stages of the disease and high variation of DNA integrity index values might have affected the statistical power of the calculations.

The correlation between nucleosomes and fragment sizes. Presented is the correlation between cNUC levels and qPCR threshold cycles (Ct) of short fragments of the ACTB and ALU in the whole study group (A and B) and in the patients (C and D), respectively. Note the reverse correlation between Ct values and nucleosomes. r, Correlation coefficient.
As discussed above, our findings are in accordance with certain studies (11, 12, 16, 17) but in contrast to others reporting a higher cfDNA integrity in CRC patients (13-15). Discrepancies across various studies may be related to many factors, including the selection of control group or preanalytical and analytical procedures, such as DNA extraction or the method to quantify cfDNA. In contrast to the majority of studies (13-15), which used samples from healthy volunteers without any information on the status of colon/rectum as controls, our control group was based on individuals who were confirmed by colonoscopy to be CRC- and polyp-free. On the other side, the phenol-chloroform extraction technique used in our study could have enriched small fragments more effectively than column-based nucleic acid isolation techniques influencing the outcomes of integrity measurements. The latter warrants further study.
Although cfDNA levels did not differ between CRC patients and controls, we found significantly higher nucleosome levels in CRC patients and distant metastases that were associated with increased levels of cNUC (21). In view of the lower DNA integrity in CRC patients, higher nucleosome levels in the patients might indicate the predominance of mononucleosomes and high fragmentation in patients' sera. When we analyzed the cNUC levels and the Ct values for the short and long fragments using both integrity indexes, we observed that the correlation is much higher for the short fragments in the whole study group and in the patients. These findings show the predominance of mononucleosomes in circulation and confirm high fragmentation of cfDNA in CRC patients.
In conclusion, our findings reveal that the size and abundance of the amplified target affects the integrity of cfDNA. Using sequences of lower abundance and longer amplicon sizes (e.g. ACTB384/ACTB106), DNA integrity analysis leads to a higher variation than the analysis with high abundant ALU sequences. Using both indexes, we detected lower cfDNA integrity values in sera of CRC patients where the ACTB384/ACTB106 index ensures better discrimination. Predominance of mononucleosomes in circulation further supports high cfDNA fragmentation in CRC patients.
Acknowledgements
The Authors declare that there is no conflict of interest.
- Received November 30, 2014.
- Revision received December 19, 2014.
- Accepted December 23, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}