


Abstract
Background/Aim: Cell-free DNA may serve as a biomarker for patients with cancer; we designed our study to determine its potential in patients with bladder cancer (BCA). Materials and Methods: Short β-actin (ACTB)-106 and large ACTB-384 fragments were quantified using real time PCR (RT-PCR); the ratio of ACTB-384/ACTB-106 was defined as DNA integrity. We analyzed the serum from 95 patients with and from 132 without BCA. Results: Patients with BCA had increased ACTB-106 levels and lower DNA integrity compared to patients without cancer. However, patients undergoing transurethral bladder resection (TURB) with histological exclusion of BCA had a similar ACTB-106 level and DNA integrity, as patients with BCA. Cell-free DNA was not correlated with smoker status, pT stage, grade or lymph node metastasis, or DNA integrity. There was a weak inverse correlation of age with DNA integrity in patients with BCA. Conclusion: Analysis of serum cell-free DNA levels and fragmentation patterns are of limited value regarding the identification of patients with BCA.
The existence of cell-free DNA in blood was discovered as early as the 1940s (1), but its potential for diagnosis, prognosis and monitoring of cancer patients was unrealised. The implementation of easy and less-expensive detection methods permitted for extensive research on the diagnostic and prognostic role of cell-free DNA, and in recent years a number of studies reported higher levels of cell-free DNA in plasma/serum of patients with various tumour entities [ovarian cancer (2), breast cancer (3), lung cancer (4), prostate cancer (5), renal cell carcinoma (6), gastric cancer (7), esophageal cancer (8)], which allowed there to be differentiated from healthy individuals and patients with non-malignant diseases. Furthermore, high levels of cell-free DNA were found to be indicative of poor prognosis [lung cancer (4); prostate cancer (5, 9)]. It was also recognized that cell-free DNA in cancer patients and healthy controls is differently sized: some studies reported an increase [breast cancer (10), colorectal cancer (11), renal cell carcinoma (12)], whereas others reported a decrease [prostate cancer (13), testicular cancer (14)] of DNA integrity in cancer patients. Similarly to quantitative changes, fragmentation patterns were also useful for prognosis (10, 13). There is no biomarker, in addition to urine cytology, used in daily routine for the diagnostic work-up of patients suspected of having bladder cancer (BCA). We reported that cell-free DNA levels and the DNA integrity allowed for patients with BCA to be identified, however, that cohort consisted only of patients undergoing radical cystectomy (15). The aim of the present study was to analyze cell-free DNA levels and fragmentation patterns in patients with non-muscle-invasive bladder cancer (NMIBC) and muscle-invasive bladder cancer (MIBC).
Materials and Methods
Patients, sample collection and DNA isolation. We prospectively collected serum samples from 227 consecutively treated patients at four urological departments (University Hospital Bonn, Saint Josef Hospital Troisdorf, Evangelische Kliniken Bonn, Katholische Kliniken Oberberg) between November 2006 and July 2007; patients with history of other cancers (apart from BCA) were excluded. Among these patients, 132 underwent transurethral resection of the bladder (TURB; presence of urothelial BCA in 84 patients) and 11 patients underwent radical cystectomy; 31 patients with non-malignant urological disorders and cystoscopically excluded BCA (e.g. surgery for incontinence or benign prostate hyperplasia) and 53 healthy individuals served as controls. All patients gave written informed consent according to the institutional guidelines; the study was approved by the Ethic Committee at the University of Bonn. The detailed clinical information of the study patients is provided in Table I. Serum samples were collected prior to surgery in a Serum-S Monovette with clotting activator (Sarstedt, Nürnbrecht, Germany). Clotting occurred for 30-240 min prior to centrifugation at 1800 ×g (10 min), and serum was then separated and stored at −20°C before shipping to the University Hospital Bonn, where all subsequent experiments were performed. Shipping was performed on dry ice within one week following collection of the samples, and samples were stored thereafter at −80°C until DNA isolation.
DNA isolation and quantitative real-time PCR. The methods used for DNA isolation and quantification were reported in detail earlier (12). In brief, cell-free DNA was isolated from 1 ml serum using the ChargeSwitch gDNA Kit (Invitrogen, Paisley, Scotland, United Kingdom) according to the manufacturer's recommendations.
We used two primer sets to determine the amount of short and long circulating DNA fragments: The 106 bp amplicon (β-actin, ACTB-106; forward primer: 5’-TCGTGCTGACAT TAAGGAG-3’; reverse primer: 5’-GGC-AGC-TCG-TAG-CTC-TTC-TC-3’) amplified both short and long DNA fragments, whereas the 384 bp amplicon (ACTB-384; forward primer: 5’-GCT-ATC-CCT-GTA-CGC-CTC-TG-3’; reverse primer: 5’-AGG-AAG-GAA-GGC-TGG-AAG-AG-3’) amplified only large DNA fragments. ACTB-106 represents total cell-free DNA including DNA of apoptotic origin, whereas ACTB-384 represents DNA from non-apoptotic cells. The annealing sites of ACTB-106 are located within ACTB-384 annealing sites, thus the ratio of ACTB-384 to ACTB-106 (termed “DNA integrity”) characterizes the fragmentation pattern of cell-free serum DNA: the DNA integrity is 1 if the cell-free DNA is not fragmented and 0 if the DNA is completely truncated into fragments smaller than 384 bp. Quantitative real-time PCR was carried out in triplicate on an ABIPrism 7900HT instrument (Applied Biosystems, Foster City, CA, USA). Each 10-μl reaction mixture consisted of 1 SYBRGreenER Mix (Invitrogen, Life Technologies, Paisley, UK), 200 nM forward and reverse primers and 1 μl of DNA sample. PCR was conducted at 90°C for 10 min, followed by 40 cycles at 95°C for 15 s and 60°C for 60 s. Melting curve analysis was performed to confirm the specificity of the PCR products. Each run included 5-fold dilutions of an external standard, negative controls and water blanks.
Statistical analysis. Cell-free DNA levels and DNA integrity were analyzed using the Mann Whitney test. The area under the curve (AUC), sensitivity and specificity were determined by Receiver Operating Characteristic (ROC) analysis. Correlations between clinicopathological parameters and serum DNA fragment levels and DNA integrity were assessed using the Mann Whitney test. Age and cell-free DNA were correlated using the Spearman test. Statistical tests were performed using the IBM SPSS Statistics v20 (IBM cooperation, Armonk, NY, United States). Significance was concluded at p<0.05.
Clinicopathological parameters.
Results
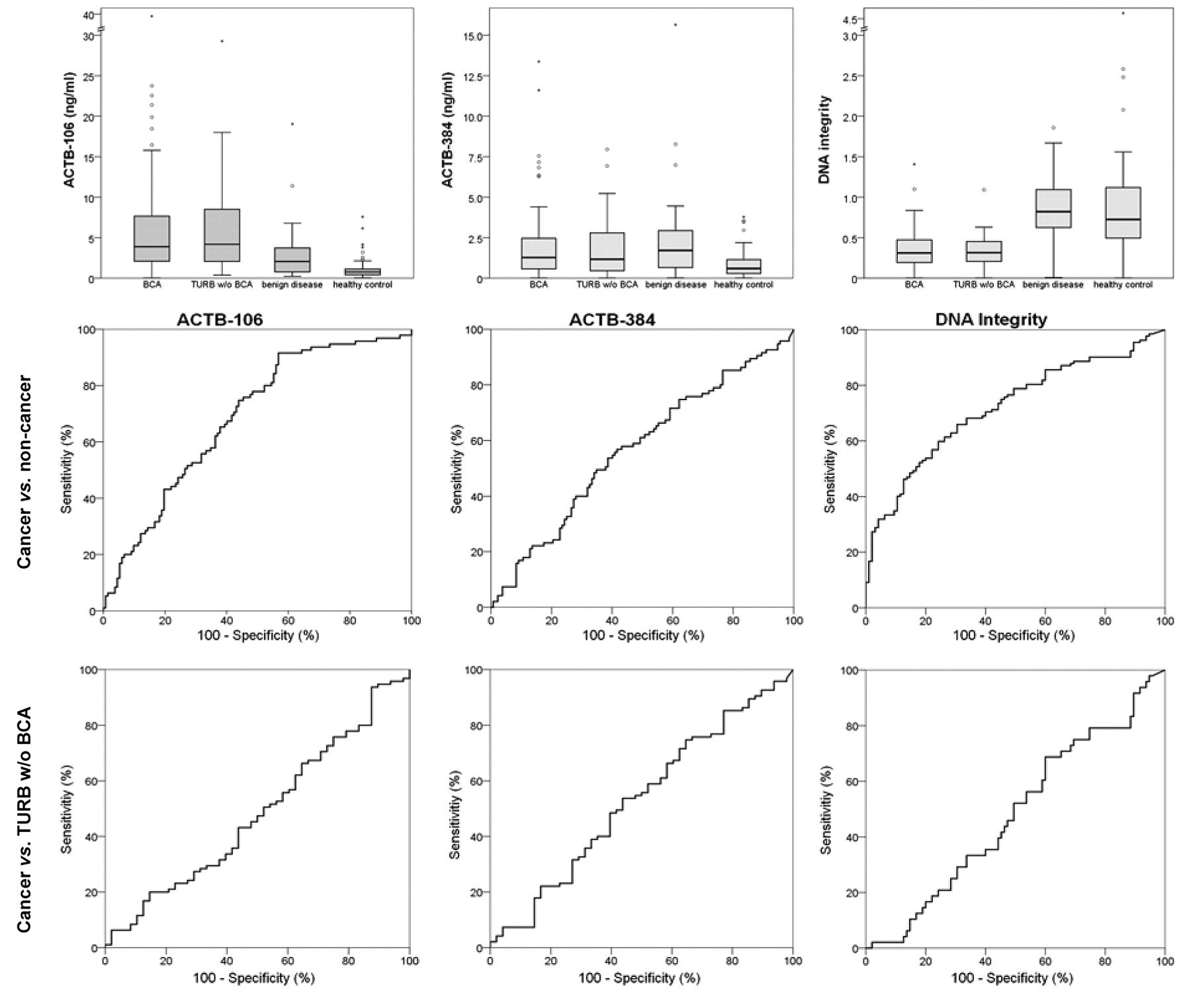
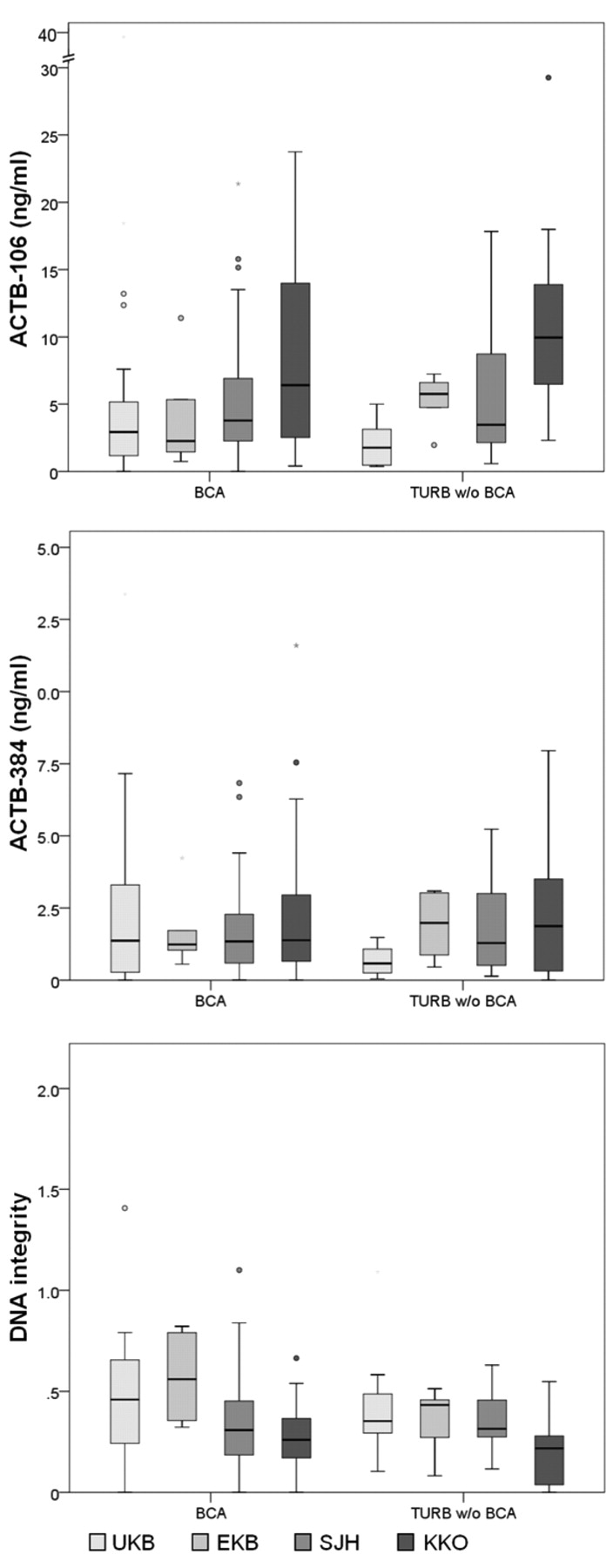
ACTB-106 was significantly increased in patients with BCA compared to those without cancer (p<0.001; mean=6.2 ng/ml vs. 3.4 ng/ml); ACTB-384 had a trend towards higher levels in cancer patients (p=0.081; mean=2.0 vs. 1.6 ng/ml). The fragmentation of cell-free DNA was higher in patients with BCA (DNA integrity; p<0.001, mean=0.36 vs. 0.69). Subgroup analyses indicated that cell-free DNA levels (ACTB-106: p=0.869; ACTB-384: p=0.722) and DNA integrity (p=0.960) were similar in patients with NMIBC and MIBC. However, the group of patients without cancer exhibited heterogeneity: patients undergoing TURB with histological exclusion of BCA had similar DNA levels (ACTB-106: p=0.732, mean=6.2 ng/ml; ACTB-384: p=0.554, mean=1.8 ng/ml) and DNA integrity (p=0.710, mean=0.33) compared to patients with BCA. DNA levels and fragmentation patterns were different in patients with benign disease (ACTB-106: p=0.002, mean=3.1 ng/ml; ACTB-384: p=0.381, mean=2.5 ng/ml; DNA integrity: p<0.001, mean=0.86) and healthy controls (ACTB-106: p<0.001, mean=1.2 ng/ml; ACTB-384: p=0.001, mean=0.9 ng/ml; DNA integrity: p<0.001, mean=0.93) compared to patients with BCA (Figure 1). We also investigated whether cell-free DNA levels were different in the participating centres; we restricted this analysis to patients undergoing TURB with and without BCA, because samples from most patients with benign disease and healthy individuals were collected at the University Hospital Bonn. We observed that there was a significant variation of ACTB-106 levels (BCA: p=0.034; without BCA: p<0.001) and DNA integrity (BCA: p=0.007; without BCA: p=0.044) between the participating centres, whereas ACTB-384 levels (BCA: p=0.957; without BCA: p=0.133) were similar. However, the cell-free DNA levels were similar in patients with and without BCA in one centre indicating that pre-analytical factors affect cell-free DNA levels (Figure 2).

Boxplot diagrams indicating the distribution of short (ACTB-106) and long (ACTB-384) cell-free DNA levels and the DNA fragmentation pattern (DNA integrity) in patients with and without bladder cancer (BCA). The Receiver Operating Characteristic (ROC) analyses show that ACTB-106 (AUC=0.686) and DNA integrity (AUC 0.719) allow for the BCA and for the whole non-cancer cohorts to be distinguished. However, cell-free DNA was not able to differentiate between patients with BCA and patients with suspicion of bladder cancer undergoing transurethral resection and exclusion of BCA (TURB w/o BCA).
We then performed ROC analyses to determine the diagnostic information: ACTB-106 (AUC=0.686, 95% confidence interval (CI)=0.617-0.755; sensitivity=91.6%; specificity=43.3%) and DNA integrity (AUC=0.719, 95% CI=0.653-0.784; sensitivity=59.8%; specificity=75.8%) allowed for patients with BCA and those without BCA to be distinguished (including patients with benign disease and healthy individuals) (Figure 1). ACTB-384 fragments did not provide useful information (AUC=0.568, 95% CI=0.492-0.644). However, patients with BCA and those without BCA who underwent TURB could not be discriminated by ACTB-106 (AUC=0.482, 95% CI=0.382-0.583), ACTB-384 (AUC=0.530, 95% CI=0.382-0.583) or by DNA integrity (AUC=0.481, 95% CI=0.383-0.579).

Boxplots demonstrating the variability of cell-free DNA levels in the participating centres. The amount of ACTB-106 was significantly increased, whereas the DNA integrity was decreased in patients from Saint Josef Hospital (SJH) and Katholische Kliniken Oberberg (KKO).
We did not find any correlation of smoker status, pT stage, grade or lymph node metastasis with cell-free DNA levels nor with DNA integrity (p>0.05). However, there was a weak inverse correlation of age and DNA integrity (r2=−0.319; p=0.001; Figure 3) in patients with BCA.
Discussion
Cell-free circulating DNA in serum/plasma is a potential biomarker for diagnosis, prognosis and therapy monitoring of patients with various tumour entities (16). In an earlier study, we demonstrated that cell-free DNA may be helpful to differentiate patients with MIBC from patients with non-malignant disease; however, this study was small-scaled and did not include patients undergoing TURB (15). We therefore performed a prospective, multicenter study to investigate the value of cell-free DNA in serum. Although we demonstrate a significant increase of small cell-free DNA fragments and a decreased DNA integrity in cancer patients compared to the whole group of patients without cancer, the enthusiasm for the utility of cell-free DNA is dampened by the analysis of the subgroups in the non-cancer patient cohort: a decrease of cell-free DNA and an increase of DNA integrity was mainly observed in patients with various benign urological diseases and healthy controls, whereas patients undergoing TURB for suspicious bladder cancer and histological exclusion of cancer had mostly high DNA levels and a low DNA integrity. Thus, the diagnostic relevance of cell-free DNA may be limited. Patients with non-malignant, but differential diagnostically relevant diseases were often not included in studies evaluating cell-free DNA as a cancer biomarker. However, the study by Chang et al. indicates that benign disease may hamper diagnosis with cell-free DNA: the AUC was distinctly lower (0.74 vs. 0.90) for the comparison of patients with non-malignant disease than the comparison of healthy controls and patients with ovarian cancer (2). The origin of cell-free DNA is only poorly understood: only a small amount of cell-free DNA is derived from cancer cells themselves (17). A high serum DNA background level may therefore impair the diagnostic accuracy of cell-free DNA testing. Considerable variation was observed between participating centres: serum samples from Saint Josef Hospital and Katholische Kliniken Oberberg had increased levels of short DNA fragments. An earlier large-scaled multicentre study with patients from the EPIC study (18) also reported a tremendous variation between the participating centres. The reason for centre variability in our study and that of Gormally et al. is not completely clear, but it is likely that the pre-analytical factors contribute to this variability. Nevertheless, Chan et al. (19) demonstrated that cell-free DNA levels and DNA integrity in plasma samples is not affected by delayed plasma separation (up to 6 hours), freeze-thaw cycles, and prolonged storage at −80°C.

The histogram demonstrates a weak inverse correlation of DNA integrity and age in patients with bladder cancer (r2=−0.319; p=0.001).
Conclusion
The predictive accuracy of cell-free DNA levels and fragmentation pattern in patients undergoing TURB for the detection of BCA is limited and cell-free DNA does not provide relevant diagnostic information.
Acknowledgements
We thank Doris Schmidt for excellent technical assistance.
- Received March 26, 2012.
- Revision received May 9, 2012.
- Accepted May 14, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}