


Abstract
There is no doubt that diet is one of the main modifiable risk factors for many degenerative diseases, including cancer. More than 30% of adult cancers can be prevented or delayed by diet, being physically active and having a healthy body weight. Plant-based foods, including fruit, vegetables, and whole grains, a favorable omega-6/omega-3 polyunsaturated fatty acids ratio, and fish consumption have a protective effect against cancer. On the contrary, a low intake of fruit and vegetables, high intake of red and processed meat, high intake of sodium, alcohol consumption, a diet rich in refined carbohydrates, and a high intake of total fat may increase risk of cancer. Furthermore, calorie restriction and having a body/mass index on the lower end of the normal range can significantly decrease or delay the onset of cancers. Most studies were performed on adults and thus the role of diet in childhood cancer is less well-understood. In the past, diet was not considered to play any role in its etiology in children. However, nowadays there is a growing body of evidence that prolonged and frequent breastfeeding, the maternal diet during pregnancy and vitamin intake during pregnancy, may impart benefit for reduced cancer risk in children. Usually, decades of healthy dietary habits are needed to see significant difference in cancer risk. Therefore, diet choices and diet preparation starting early in life deserve more attention. Here we review data focusing on which dietary factors, including food-borne carcinogens, affect the onset of cancers in adults and stress out the potential role of diet in childhood cancer prevention.
Abbreviations: AICR, American Institute for Cancer Research; CYP, cytochrome P450-dependent monooxygenase, EGCG, epigallocatechin 3-gallate; GI, glycemic index; GL, glycemic load; HAA, heterocyclic aromatic amine; IQ, 2-amino-3-methylimidazo[4,5-f]quinoline; MeIQ, 2-amino-3,4-dimethylimidazo[4,5-f]quinoline; MeIQx, 2-amino-3,8-dimethylimidazo[4,5-f]quinoxaline; n-3, omega-3; n-6, omega-6; ORAC, oxygen radical absorbance capacity; PAH, polycyclic aromatic hydrocarbon; PCB, polychlorinated biphenyl; PhIP, 2-amino-1-methyl-6-phenylimidazo[4,5-b]pyridine; PUFA, polyunsaturated fatty acid; TCDD, 2,3,7,8-tetrachlorodibenzo-p-dioxin, THM, trihalomethane; WCRF, World Cancer Research Fund.
Cancer is the second leading cause of death in the U.S.A. and in most high-income countries (1). Cancer is responsible for 44% of all deaths in Japan, 35% in Australia, 33% in Spain, 33% in the United Kingdom, 30% in Poland, 29% in the U.S.A and in Germany, 22% in China, 20% in South Africa, 20% in Brazil, 18% in Mexico, 15% in India, and 9% in Egypt (2). The most commonly diagnosed cancers worldwide are lung, breast, and colorectal cancers (3). The latest trend analysis shows that overall cancer incidence rates and death rates are decreasing in the U.S.A. (4). In particular, death rates for the most frequent cancer types including colon and rectum, prostate in men and breast in women are decreasing. These figures indicate improved primary prevention, early detection and improved treatment. While these figures are promising, the lifetime probability for the development of cancer in U.S.A. adults is high at 1 in 2 for men and 1 in 3 for women. Furthermore, as populations are aging around the world, cancer is likely to grow as a public health concern.
Although cancer is still relatively rare in childhood, it is the second most common cause of death among U.S.A. children 1 to 14 years of age (5) and it is the leading cause of disease-related death in children and adolescents in the U.S.A. and Canada. Major categories of pediatric cancer include leukemia (34% of all childhood cancers in U.S.A.), brain and other nervous system (27%), neuroblastoma (7%, most common in children younger than 5 years), Wilms tumor (5%), Hodgkin's and non-Hodgkin's lymphoma (4%, each), rhabdomyosarcoma (3%), retinoblastoma (3%, usually occurring in children younger than 5 years), and the bone cancers osteosarcoma (3%) and Ewing sarcoma (1%) (6). Of concern is that unlike the decreased incidence trends seen in adults, incidence rates for childhood cancers are increasing (4). However, progress in treatment has seen reductions in cancer death rates among children since the 1970's. The 5-year survival rates for all childhood cancers in the U.S.A. combined has increased from 58.1% in 1975-77 to 83% for ages 0-4 years; 81.2% for ages 5-9 years; 82.7% for ages 10-14 years; and 82.8% for ages 15-19 years in 2001-2007 (7). Rates vary considerably depending on cancer type and patient characteristics, with the 5-year survival for Hodgkin's lymphoma at 95%, compared with a 70% 5-year survival for brain and other nervous system cancers (6). However, more than 80% of children live in low and middle income countries where the survival rate may be as low as 5%.
The latest figures from the World Cancer Research Fund (WCRF) and the American Institute for Cancer Research (AICR) show that a third of the most common cancers in the world could be prevented by a healthy diet, being physically active and maintaining a healthy body weight (8). The cancers most preventable by appropriate food, nutrition, physical activity, and body fatness include those of the esophagus, mouth, pharynx, and larynx, of colon and rectum and of the breast. Therefore, diet and lifestyle factors are second only to the abstinence of tobacco smoking to reduce the risk of cancer. The role of diet in childhood cancer prevention is less well-understood. It is, therefore, essential to identify the genotoxic risk factors in food and beverages that may have a role in the etiology of major cancers.
In this article, we summarize the current state of knowledge on diet and cancer; however, this article is not a systematic review. The most comprehensive review on this subject is the expert report of WCRF and AICR published in 2007 (2). This report is one of the most authoritative sources on food, nutrition, and cancer prevention available. Our review considers more recent studies published after 2007 together with mechanistic studies and explores in more detail the potential role of diet in childhood cancer prevention. First, we discuss the carcinogenic factors in the diet (Figure 1) and, later on, we review on the protective role of dietary constituents.
Carcinogenic Factors in the Diet
Red meat. Probably the most researched dietary component in relation to cancer risk is red meat. The expert panel concluded there is convincing evidence that red meat is a risk factor for colon and rectal cancer (2). Red meat includes beef, pork, and lamb. Some studies have suggested that it is not the red meat itself, but the high fat intake or the way meat is prepared. Other studies have attributed the association to heme iron, nitrates/nitrites, and heterocyclic aromatic amines (HAAs; cf. Figure 2) (9). It is important to note that so-called food-born carcinogens, notably HAAs, are formed following extensive heating (>180°C) of protein-rich material, including meat from poultry and fish. However, there is no correlation between rectal cancer and poultry or fish consumption (10). Therefore, it is reasonable to search for specific factor(s) that are present in beef, pork, and lamb that might causally be involved in colon cancer formation. Red meat is rich in blood and, therefore, a reasonable hypothesis rests on the finding that heme iron can induce oxidative DNA damage, which is associated with fecal water cytotoxicity (11). Hemoglobin and hemin given in a low-calcium diet to rats have been shown to increase the development of colon cancer (11).
The heme content in freeze-dried feces and fecal water correlates to the red meat (hemoglobin) intake and reaches levels of 19-1,097 μM (12). Evidence from human studies also suggests that increased intake of heme is associated with increased incidences of colon cancer, especially among women who consume alcoholic beverages (13). Heme is supposed to raise lipid peroxidation giving rise to DNA etheno-adducts. It may also contribute to N-nitroso compound formation. The proposed mechanism of mutagenic DNA adducts that result from the metabolism of red and strongly heated (>180°C) meat as well as from nutrients that are involved in protection are outlined in Figure 3.
Processed meat. In addition to red meat, there is convincing evidence that processed meat (including processed fish) is a risk factor for colon and rectal cancer (2). Processed meat has been altered from its natural form to enhance its digestibility, taste, color, or preservation. Examples of processed meat include hotdogs, salami, lunch meat, bacon, breakfast sausage, beef jerky, pepperoni, and sandwich meat. Examples of processing include cooking, smoking, barbecuing, grilling, or using salt, sugar, or chemical ingredients such as nitrates or nitrite. Sodium nitrite is used as a color fixer in meat, and as a preservative. The greatest concern is sodium nitrite, which forms together with secondary amines from proteins carcinogenic nitrosamines in the stomach (14) that enter the bloodstream.
Regarding the HAA concentration in meat and fish, preparation is most important. HAAs are formed at high temperature. In general, barbecued meat will have the highest content, followed by grilled and then pan-fried meat. The type of meat is also important. The highest levels of HAAs are found in well-done chicken (15). Marinating decreases the HAA content (16-17). HAAs (19 of them have been identified thus far) represent presumably the most important mutagenic and genotoxic group of food-born carcinogens. Several HAAs including 2-amino-3-methylimidazo[4,5-f]quinoline (IQ), 2-amino-3,4-dimethylimidazo[4,5-f]quinoline (MeIQ), 2-amino-3,8-dimethylimidazo[4,5-f]quinoxaline (MeIQx), and 2-amino-1-methyl-6-phenylimidazo[4,5-b]pyridine (PhIP) are potent mammary gland carcinogens in rats. PhlP is the most abundant of the various carcinogenic HAAs (present at a level of 0.56 to 69.2 ng/g of cooked meat or fish), followed by MelQx at 0.64 to 6.44 ng/g (18).
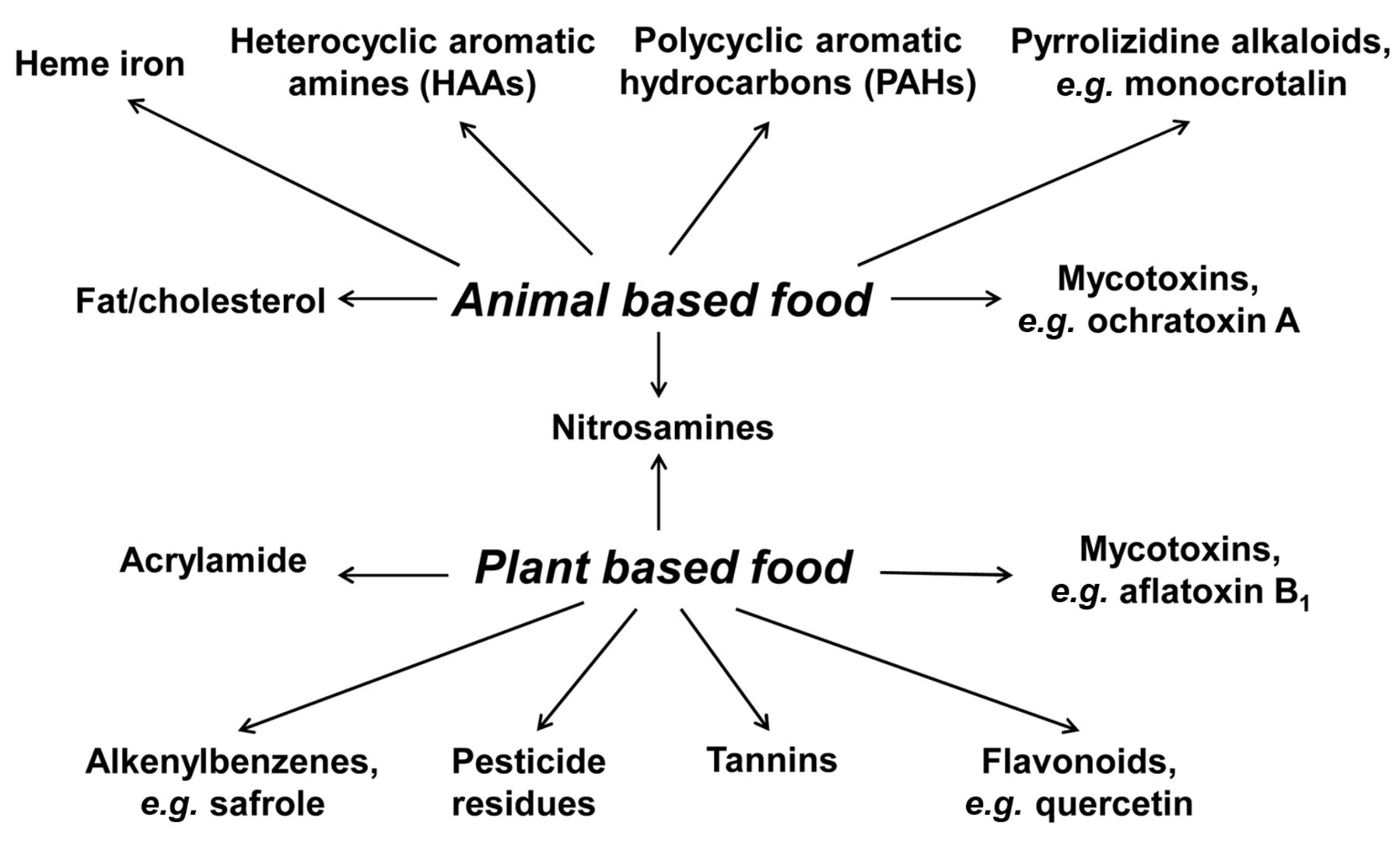
Potential carcinogenic factors in animal and plant based food.
HAAs are stable compounds formed as pyrolysis products of amino acids such as glycin that react with creatine. This happens notably at the surface of heated fish and meat of beef, pork, and poultry at a temperature above 160°C. HAAs are also found in white and red wine, beer and tobacco smoke. It is estimated that the daily intake of these compounds does not exceed 1 μg/person. The metabolism of PhIP has been studied in detail. PhIP is metabolized in the liver by cytochrome P450-dependent monooxygenase (CYP) 1A2 and UDP-glucuronosyl transferase to a glucuronide, which is excreted from the gut into the intestine. There it is further metabolized by bacterial β-glucuronidases and intestinal sulfotransferases and acetyltransferases. The resulting esters can spontaneously form a highly reactive nitrenium ion that has the ability to react with the nucleophilic DNA, giving rise to DNA adducts. Depending on the HAA substrate, several other CYPs can be involved such as CYP1A1, CYP1B1 and to a lesser extent also CYP2C9, CYP2D6, and CYP3A4 (19). However, CYP1A2, a major hepatic CYP, has a high catalytic activity for this activation and, therefore, appears to be the predominant isozyme responsible for HAA metabolic activation (20).
As described above, N-hydroxy-HAAs are weakly reactive and form DNA adducts without further metabolism. However, phase II esterification of N-hydroxy-HAAs by enzymes such as N-acetyltransferase and sulfotransferase produces highly reactive nitrenium ion derivatives that greatly enhance DNA adduct formation (21). Metabolic activation and DNA adduct formation are essential for HAA carcinogenesis. It has been shown that PhIP exerts organotropy, causing breast carcinomas. The mechanism involved is not yet known. It is supposed that it may partly involve alterations in levels of circulating hormones such as prolactin. The increase in serum prolactin secretion by PhIP is further expected to promote tumor development. Alterations in cell signaling and gene expression by PhIP are also likely to be relevant for its effect on cell proliferation and development (21).
Another group of carcinogens formed during the processing of meat at elevated temperature is represented by polycyclic aromatic hydrocarbons (PAHs), which are formed by strong heating of meat and fat (Figure 2). Thus, benzo[a]pyrene has been found in measurable amounts in grilled meat (e.g., 38 ng/g in hamburgers) (22) and other dietary ingredients (23). These carcinogens are chemically stable and will not be decomposed during heating and following ingestion. They are metabolized in the liver forming reactive electrophilic species, notably dihydrodiol epoxides, that bind to DNA. The carcinogenic effect of PAHs is well-known, with N2-guanine adducts playing a significant role in mutagenesis and carcinogenesis (see Diggs et al., 2011, for a recent review on PAHs and digestive tract cancers) (24). DNA adducts of PAHs have been observed in white blood cells of humans after consumption of grilled meat (25).
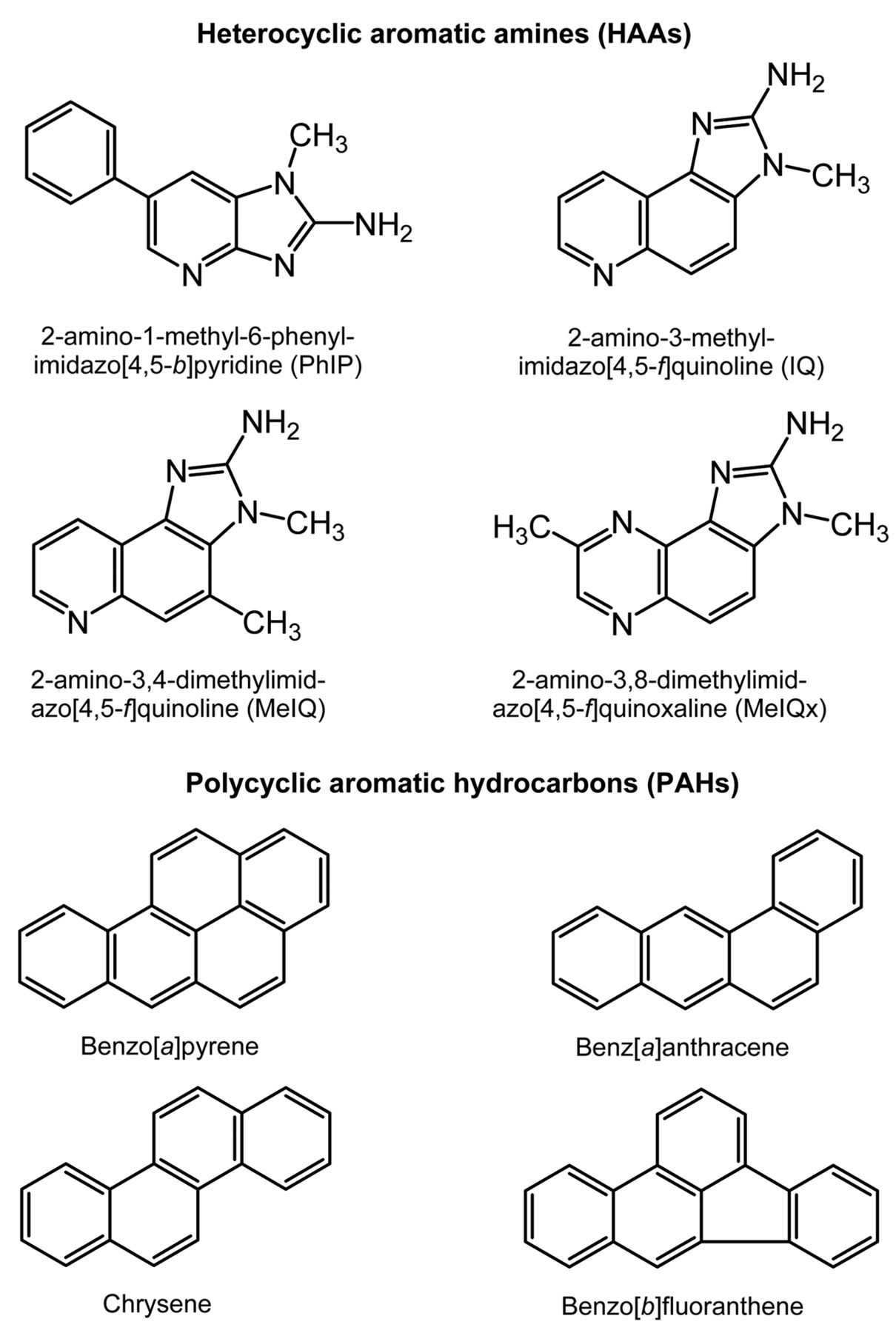
Some heterocyclic aromatic amines and polycyclic aromatic hydrocarbons found in fried and grilled meat.
Recently, considerable amounts of acrylamide have been detected in carbohydrate-rich foods, especially in heated commercial potato products like French fries and potato chips (26). Since acrylamide is probably carcinogenic to humans (Group 2A) (27), this observation has raised serious health concerns. The cancer risk caused by lifelong intake of acrylamide in foods was calculated to be 0.6×10−3, implying that 6 out of 10,000 individuals may develop cancer due to dietary acrylamide (28).
Poultry. While poultry does not seem to be associated with colon cancer, some studies found a significant link between the risk for prostate cancer progression with post-diagnostic consumption of poultry, but not red meat or fish (29). High consumption of poultry together with high intake of red meat, fat and saturated fatty acids may play a causative role in breast cancer development (30). Excessive poultry consumption was also shown to be associated with an increased risk for endometrial cancer, although the highest association was found with red meat (31). On the other hand, poultry has been associated with a decreased risk for colorectal cancer; especially the consumption of chicken was proposed to be beneficial (32).
Eggs. Few studies have looked separately at the risk or preventive effect of egg consumption on cancer development. Eggs are usually studied together with meat, poultry, and fish. Eggs are a very rich source of selenium, iodine, and vitamin B2, and a rich source of protein, molybdenum, phosphorous, vitamin B5, vitamin B12, and vitamin D (33). Eggs also contain choline (33-34), which has been linked to decreasing inflammation, concentrations of C-reactive protein, interleukin-6, and tumor necrosis factor alpha (35). The major health risk of egg consumption is an allergic reaction (33, 36). Egg yolk is also very high in dietary cholesterol. Overall, there is no clear evidence that egg consumption increases or decreases cancer incidence. However, there is evidence that choline, the essential nutrient found in eggs, decreases the risk of breast cancer (37). Moreover, a choline-devoid diet promotes hepatocarcinogenesis in the rat (38). Finally, an enhanced DNA damage level in human lymphocytes was related to a deficiency in the nutrient choline (39).
Milk and dairy products. Dairy products such as cheese, butter, and yoghurt are made from milk. Their consumption is controversial in regard to human health. There are pros and cons for health to dairy consumption. High consumption of dairy is not necessarily beneficial and can in some cases be harmful to human health, because it contributes excessive cholesterol and fat to the diet, which can increase the risk of diseases, including cancer (40-41). Overall, the evidence for cancer risk related to milk and dairy product intake is mixed, depending on the type of cancer and the dairy product (2). While some studies have found an increased risk for some cancers with high intake of dairy (42-44), others have found a decreased risk (45).
Fiber. A diet low in fiber has been shown to increase the risk for some types of cancers, such as colon cancer (46). The reason is likely the facilitation of gut passage of digested food, which reduces the time of formation of and exposure of gut and other targets in the body to endogenously-formed carcinogens. Therefore, it is recommended to add fiber-containing food to daily diet (47).
Refined grains. Refined grains contain only endosperm. Examples of refined grains are white bread, pasta, white rice, and white flour. In contrast to whole grains, refined grains have been linked to increased risk for some diseases, especially diabetes, metabolic syndrome, obesity, and cancer. For example, refined grains, starches, and sugars are related to an increased risk of colorectal cancer (48). Refined grain, along with its high glycemic index (GI) and glycemic load (GL) (see below) is associated with an increased risk for several types of cancers (49).
Sugar. The World Health Organization and the Food and Agriculture Organization of the United Nations expert report defines free sugars as all mono- and disaccharides added to foods by the manufacturer, cook, or consumer, plus sugars naturally present in honey, syrups, and fruit juices. Foods containing sugar pose a limited – suggestive increased risk for colorectal cancer (2). Additionally, pancreatic cancer can possibly develop when soft drinks and juices are consumed regularly (50).
Lipids/fats. A limited – suggestive increased risk has been found for total fat consumption on the development of lung and post-menopausal breast cancer (2). There is also a limited – suggestive increased risk for foods containing animal fat for the development of colorectal cancer and a limited – suggestive increased risk for butter for the development of lung cancer (2). However, the latest dietary fat and fatty acid intake recommendations suggest that there is probably evidence that total fat has no relation to cancer risk and there is insufficient evidence for cancer risk depending on mon-ounsaturated fatty acids, total polyunsaturated fatty acids (PUFAs), omega-6 (n-6) PUFAs or trans-fatty acid intakes (51).
Results of pooled cohort studies often show no relation between total fat intake or types of dietary fat and cancer development such as breast cancer (52-53), or colorectal cancer (54). However, measurement error of diet is a major problem when examining associations between diet and disease end-points such as cancer. Results of case-control studies, comparisons between and within countries, and using animal models generally show a positive relation between incidence of cancers such as breast cancer and fat consumption (55-56). However, the control of the amount of body fat seems to have a greater influence on breast cancer incidence than the reduction of fat intake (57). Although total fat intake has not been strongly related to higher cancer risk, some evidence suggests that the type of fat may play a crucial role in the development of cancer. In animal models, the tumor-promoting effect of fat intake is primarily observed for poly-unsaturated fats (58-59). However, such association was not supported by the pooled data from large cohort studies. Correlation between fat consumption and cancer risk may be explained by fat stimulating bile acids, which are excreted into the lumen of intestine. In the colon, bile acids are metabolized by bacteria into deoxycholic acid and lithocholic acid that may cause DNA damage and cancer.

Mechanism of red and processed (strongly-heated) meat that contributes to cancer formation (adapted from Bastide et al. (11)).
Dietary supplements. Most recently, two reports were published, highlighting supplements as a cause for a higher incidence of cancer. One was the study by Bjelakovic et al. in 2010 (60) conducted as a meta-analysis of 67 randomized controlled trials which showed that vitamin E, vitamin A, and β-carotene supplements may be associated with an increased incidence of mortality. The α-tocopherol, β-carotene cancer prevention trial (61) found higher incidence of lung cancer (18%) and mortality (8%) among men who received β-carotene compared to those who did not. Another large randomized controlled trial (SELECT) investigating the effect of selenium and vitamin E on risk of prostate cancer and other cancers was stopped in 2008, after reporting statistically non-significant increased incidence of prostate cancer in the vitamin E group (62).
Other dietary factors: Western-diet pattern. Many researchers have concluded that a Western-type diet is a risk factor for cancer development. A Western-type diet is a diet high in animal protein, low in fiber, high in refined grains and processed foods, and high in salt and sugar. Some studies have shown that a Western-type diet elevates plasma levels of sex hormones and decreases the sex hormone-binding globulin concentration, thereby increasing the bioavailability of these steroids (63). This diet also results in low formation of mammalian lignans and isoflavonoid phytoestrogens. These diphenolic compounds seem to affect hormone metabolism and the production and growth of cancer cells by many different mechanisms, making them candidates for a role as cancer protective substances. The precursors of these diphenols are to be found in fiber–rich, unrefined grain products, various seeds, and beans and probably also in pulses, peas, and berries. The sex hormone patterns found in connection with a Western-type diet is a prevailing factor in breast cancer patients, but is only partly a result of the diet (63).
GI and GL of foods. Another important factor in the relationship between carbohydrates and cancer risk is their GI and GL. The GI is a measure of the effects of carbohydrates on blood sugar levels. The GL is a ranking system for carbohydrate content in food portions based on their GI and the portion size. The GI is an experimental system that classifies carbohydrates and carbohydrate-containing foods according to their blood glucose–raising potential. High GI and GL may influence cancer risk via hyperinsulinemia and the insulin-like growth factor axis (64-65). Some studies have shown beneficial effects of a diet containing foods with low GI across a wide spectrum of pathological conditions including obesity and cancer (66). Foods with low GI are usually those with high content of fiber and complex carbohydrates, while high-GI foods are those that are processed, contain white flour, or are high in simple carbohydrates. High-GI foods are those with a GI of 70 or higher (such as candy, potatoes, and white bread); moderate-GI are those with a GI of 56-69 (such as brown rice, apricots, and raisins); and low-GI foods are those with a GI of 55 or less (such as yogurt, cucumbers, and apples). Some studies have shown that low-glycemic and very-low-fat vegan diets alter tumor biology as assessed by changes in tumor gene expression, with a common mechanism perhaps being weight loss. No effect was seen with a traditional low-fat diet (67). A diet with a high GL, but not a high GI, was positively associated with the risk of endometrial cancer, particularly in obese women (68).
Alcohol. While alcohol in moderation is known to decrease the risk for heart disease, even moderate alcohol consumption is not beneficial in terms of cancer. The evidence is convincing that alcohol intake increases the risk of cancers of the mouth, pharynx, larynx, esophagus, colorectal cancer in men, and pre- and post-menopausal breast cancer in women (2). The strength of evidence is probably that alcohol consumption increases risk of liver cancer and colorectal cancer in women (2). Alcohol seems to be one of the most significant dietary risk factors for the development of colorectal cancer; where highest consumers of alcohol have a 60% greater risk of colorectal cancer than non-drinkers and light drinkers (69). Alcohol is also an important factor in the development of breast cancer (70) and was found to be a risk factor for the development of a second primary breast cancer. Regular drinking has been associated with an increased risk of asynchronous contralateral breast cancer, and the risk was shown to increase with duration (71). Recently, a study has found a new and previously unrecognized potential link that may finally explain the relationship between alcohol consumption and breast cancer: the production of reactive oxygen species by ethanol-inducible CYP2E1 (72). The risk of cancer following alcohol consumption is significantly higher when combined with smoking (73). A likely mechanism for this is chronic inflammation that is often found in the esophagus of heavy drinkers, which is considered a tumor-promoting factor (74). In addition, the degradation product of alcohol, acetaldehyde, is able to directly damage DNA leading to mutagenic adducts (75-76). Therefore, alcohol may even be considered as a weak genotoxicant and carcinogen.
Spices and herbs. There are only two known spices that contain natural carcinogens and may stimulate cancer development, if used in high doses: Capsaicin found in chili peppers and safrole occurring in small amounts in black pepper and in nutmeg. High use of these spices may contribute to stomach and liver cancer (77). More research, however, needs to be done to evaluate the effects of herbs and spices on cancer risk.
Drinking water. Additives commonly found in drinking water include chlorine and fluoride. Chlorination of drinking water was found to be associated with increased cancer risk (78-79). Chlorine is used to fight waterborne diseases such as cholera and typhoid to prevent epidemic outbreaks, while fluoride is added to prevent dental caries. However, cancers of the oral cavity and pharynx, colon and rectum, hepato-biliary and urinary organs have been shown to be positively associated with water fluoridation (80). Brain tumors and T-cell system Hodgkin's disease, non-Hodgkin's lymphoma, multiple myeloma, melanoma of the skin, and monocytic leukemia are also correlated with water fluoridation. In a recent review of 36 cancer sites studied in relation to water fluoridation, 23 were positively significant (63.9%), 9 not significant (25.0%), and 4 negatively significant (11.1%) (80). This may indicate a complexity of mechanisms of action of fluoride in the body, especially in view of the co-existing positive and negative correlations with the fluoridation index. The likelihood of fluoride acting as a genetic cause of cancer requires consideration (80). Many high-income European countries stopped water fluoridation several years ago.
Contaminants found in water include polychlorinated biphenyls (PCBs), trihalomethanes (THMs), and heavy metals. Disinfection by-products are formed when disinfectants (chlorine, ozone, chlorine dioxide, or chloramines) react with naturally occurring organic matter in the water, anthropogenic contaminants, bromide, or iodide during the production of drinking water (81). A recent epidemiological study found that an increased risk for bladder cancer was associated with three factors: THM levels, showering/bathing/swimming, and genotype (expressing the GSTT1-1 gene). These findings highlight the importance of dermal/inhalation exposure to the THMs or other possible disinfection by-products and the role of genotype in the risk for drinking-water–associated bladder cancer (81). Arsenic can get into drinking water from natural deposits in the earth or from industrial and agricultural pollution; this contamination poses an increased risk for the development of lung cancer (2).
Food contaminants. Here we will discuss only few environmental contaminants that are diet-related. Carcinogenic agents can be found in herbicides, fungicides, and insecticides. There is suggested evidence of a causal link between pesticides and Hodgkin's lymphoma, non-Hodgkin's lymphoma, multiple myeloma, soft-tissue sarcoma, and cancers of the central nervous system, breast, colon, lung, ovaries, pancreas, kidneys, stomach, and testes (82). Some studies have linked breast cancer to exposure to the pesticide 1,1,1-trichloro-2,2-di(4-chlorophenyl)ethane (dichlorodiphenyltrichloroethane, DDT) prior to puberty; non-Hodgkin's lymphoma to exposure to pesticides and solvents; and prostate cancer to exposure to pesticides (82).
Aflatoxin B1 is a naturally-occurring mycotoxin produced by Aspergillus flavus and Aspergillus parasiticus that can damage the liver and may lead to liver cancer. The fungi that produce aflatoxin B1 grow on crops such as peanuts (especially), wheat, corn, beans, and rice. Aflatoxins become metabolically activated in the liver to epoxides. They are strong carcinogens and pose a convincing increased risk for liver cancer (2, 83-84).
Food may also be contaminated with polychlorinated aromatic compounds like PCBs, polychlorinated dibenzodioxins or dibenzofuranes. In the past, extensive contamination of food with PCBs occurred at several dramatic occasions (85). Currently, PCBs pose a minor nutritional problem since their industrial use was banned in 2001 (86). At present 2,3,7,8-tetrachlorodibenzo-p-dioxine (TCDD) calls for high attention, since it is the most toxic of polychlorinated aromatic compounds (87). TCDD is formed as by-product during the synthesis of certain chlorinated herbicides and during combustion of chlorinated organic compounds for example in incineration plants (88). Contamination of human food with TCDD sporadically occurs by polluted animal feed (89). Because of its lipophilicity, TCDD accumulates in milk and other dairy products, eggs and meat (89). Although TCDD is not mutagenic, it is found to be carcinogenic in animals (88), probably due to its potent tumor promoting activity (90). The International Agency for Research on Cancer concluded that TCDD is carcinogenic to humans (Group 1) (88). Recently however, the health hazard provoked by the carcinogenicity of TCDD has been questioned (91).
Body weight. In 2002, about 41,000 new cases of cancer in the U.S.A. were related to obesity (92). Overweight and obesity were implicated in 20% of deaths in U.S.A. women and 14% in men (93). The World Health Organization estimated that in 2008 1.4 billion adults worldwide were obese (94). Evidence is convincing that greater body fatness is a cause of adenocarcinoma of the esophagus and cancers of the breast (post-menopause), pancreas, kidney, endometrium, and colorectum, as well as a cause of gallbladder cancer, although the level of evidence is lower (2). The evidence that body fatness causes liver cancer is limited. From numerous epidemiological studies, we know that the most important environmental risk factors for breast cancer development are alcohol intake, being overweight, and gaining weight (70). The ideal body/mass index is 21-22 with a range of 18.5-24.9 being generally regarded as healthy (2). Obese people are likely to have more inflammation and an altered immune response, which can influence hematopoietic and lymphoid cell function. Most studies that investigated body/mass index or obesity and non-Hodgkin's lymphoma, multiple myeloma, or leukemia reported a positive statistically significant association (2). Researchers speculate that obesity is related to cancer by raising the body's levels of sex hormones such as estrogen or protein hormones such as insulin and insulin-related growth factors. For example, too much fat around the waist can disrupt insulin metabolism and increase the risk for cancer (95). Insulin receptors are overexpressed in human breast cancer. Thus, insulin stimulates growth of breast cancer cells. There is also an association of breast cancer with insulin resistance and hyperinsulinemia (96).
Cancer-prevention by Diet
Role of animal- and plant-based nutrition. The protein content in the human diet consists of animal-based and of plant-based proteins. Animal protein occurs in red meat, poultry, fish, eggs, milk, and cheese. Examples of plant-based proteins are legumes, vegetables, soy products, nuts, and seeds. In terms of cancer risk, research has not been consistent in proving that a vegetarian diet is healthier than a well-balanced diet not excluding animal products. The European Prospective Investigation into Cancer and Nutrition (EPIC) study found that vegetarians have lower cancer rate in general but higher rate for colorectal cancer (97). Some studies have suggested that long-term (≥two decades) low consumption of meat (<once per week) is associated with life extension (98). Some researchers suspect that the reason vegetarians have a lower incidence of chronic diseases, including cancer, is not due to meat exclusion but due to high consumption of fruits and vegetables in combination with food restriction (99). Others suggest that the reason for longevity in some vegetarians may be the low methionine content of a vegetarian diet. Recent studies confirmed that dietary methionine restriction increases both the mean and maximal lifespan of rats and mice (100). Other studies are investigating why high consumption of meat may be poor for health, examining such factors as its high iron content, contaminants, processing, and preparation (see section: Carcinogenic factors in the diet).
Poultry. Poultry is the meat from domestic fowl, such as chickens, turkeys, ducks, or geese. Chicken is a very rich source of niacin, which is a cancer-protective B vitamin that is required by components of DNA (101). Chicken is also a rich source of selenium, which has cancer-protective benefits, including enhancement of DNA repair (101). Overall the evidence for poultry meat intake and cancer is limited (2). Processing of poultry meat can result in the same risk factors found in processed red meat.
Fish. Consumption of fish is believed to be beneficial for health, especially due to its high content of omega-3 (n-3) PUFAs; n-3 PUFAs are discussed separately in the fat section (see below). The American Heart Association recommends eating fish at least twice a week due to its n-3 PUFAs content (102). Fish and hence a diet rich in n-3 PUFAs is associated with decreased risk for developing cancer (103-104). The health risks and benefits of eating fish vary based on the stage of life, where children and pregnant women should avoid shark, swordfish, king mackerel and tilefish, because they may contain high levels of mercury, PCBs, dioxins, and other contaminants. Fish consumption is associated with a reduced risk of colorectal cancer (2, 105). The possible mechanism by which fish consumption could decrease colorectal cancer risk is by reducing inflammation. Serum C-reactive protein levels were found to be lower in people consuming fish than in controls (106). The protective effect of fish consumption against some cancers can be also be attributed to the high vitamin D content in fatty fish, while vitamin D deficiency is associated with increased risk for cancer development (107). Vitamin D is discussed further in the vitamins section. The World Cancer Research Fund/American Institute for Cancer Research expert panel conclude that there is limited evidence that fish (and also food containing vitamin D) protects against cancer (2). Because of the high salt content, there is a probable increased risk from Cantonese-style salted fish consumption for nasopharyngeal cancer (2).
Milk and dairy products. Dairy products contain several potentially anticancerogenic components, such as calcium, vitamin D, butyric acid, conjugated linoleic acid, sphingolipids, and probiotic bacteria (in fermented products such as yogurt) (108). Some studies have found an inverse association of melanoma with greater consumption of dairy foods or other dietary sources of vitamin D (109). The benefit of vitamin D is discussed further in the vitamin section. Preliminary data from the European Prospective Investigation into Cancer and Nutrition (EPIC) study revealed that an intake of 35 g of dairy a day (~1 ounce of cheese) doubled the risk of breast cancer in women compared with a daily intake of 10 g or less (105). In contrast, bovine lactoferrin (isolated by dairy technology) has been shown to inhibit carcinogenesis in addition to its preventive and therapeutic effects on infection and inflammation (110).
Most adults will naturally lose the ability to digest milk by lactase, if not exposed to it regularly. One study looked at the association between developing cancer and lactose digestion (111). Phenotypically, the population can be divided into those who can assimilate lactose and those who cannot. This study found a statistically significant increase in risk for colorectal and prostate cancer and ulcerative colitis among those who could digest dairy food and a statistically significant decreased risk for stomach cancer. In the group that could not assimilate lactose, the stomach cancer risk increased. Thus, in further studies it may be important to distinguish between those who are able or unable to assimilate lactose (111).
The WCRF/AICR expert panel concluded that the evidence for milk intake suggests a probable protective effect on colon and rectum cancers and a limited – suggestive decreased risk for bladder cancer (2). However, there is a probable increased risk for prostate cancer from a diet high in calcium (2). Furthermore, there is limited – suggestive evidence of an increased risk for prostate cancer from milk and dairy products. An updated systematic review and meta-analysis of 10 cohort studies showed that a 200 g/day increase in milk intake was associated with a significant reduction in colon cancer (45). In terms of dairy products, cheese has been suggested to be linked to a limited increase in colorectal cancer (2). Results from a recently published meta-analysis suggest that dairy products reduce colorectal cancer, while higher intakes of cheese were not associated with colorectal cancer (45).
Pulses and legumes. Pulses are leguminous crops harvested for their dried seeds, which excludes vegetable crops and other legumes that are grown mainly for oil extraction. Legumes include alfalfa, clover, peas, beans, lentils, lupines, mesquite, carob, soy, and peanuts. Legumes are low in fat and are excellent sources of protein, dietary fiber, and a variety of micronutrients and phytochemicals. Pulses contain a rich variety of compounds that, if consumed in sufficient quantities, may help reduce tumor risk (112). There is a limited – suggestive protective effect of pulses for prevention of stomach and prostate cancers (2, 113). Soybeans are unique legumes, because they are a concentrated source of isoflavones (114). These compounds have weak estrogenic properties and the isoflavone genistein influences signal transduction (114). Isoflavones and soy products have received significant attention for their potential role in preventing and treating cancer and osteoporosis (114). In addition, beans (as well as berries) are one of the best sources of dietary antioxidants (115).
Cereals (grains). Whole grains are cereals that contain the entire grain kernel (bran, germ, and endosperm) including brown rice, bulgur, oatmeal, and whole-wheat flour. The benefit of whole-grain for health and cancer prevention is primarily due to its dietary fiber content. For most epithelial cancers, whole grains together with vegetables, fruit, and fish were associated with a decreased risk for cancer development (116).
Gluten intolerance (celiac disease) is quite common in the population and markedly under-diagnosed. People with gluten intolerance have higher risk for the development of malignancies, especially if the intolerance is diagnosed late in the clinical course of the disease (117). Gluten is present in both whole- and processed wheat products.
Fiber. Dietary fiber is the indigestible portion of plant food. It consists of soluble and insoluble parts. Foods high in fiber include whole grains, nuts, seeds, fruits, and vegetables. Chemically, dietary fibers are non-starch polysaccharides such as arabinoxylans, cellulose and other plant components such as dextrins, lignin, pectin. As fiber moves through the intestinal tract, it helps to move waste out of the body.
Dietary fiber intake is important from a metabolic viewpoint, acting as a prebiotic to support microbiota health in preventing colon cancer (118). Fiber can bind bile acids, which produce carcinogenic metabolites, and fermented fiber produces volatile fatty acids that can protect against colon cancer (119). Foods containing fiber confer a limited – suggestive decreased risk for the development of esophageal cancer and a probable decreased risk for the development of colorectal cancer (2, 105).
Fruit and vegetables. The benefits of fruit and vegetable consumption are numerous. Fruit and vegetables contain many vitamins and minerals and phytochemicals that have antioxidant activities. Phytochemicals include salicylates, flavonoids, glucosinolates, terpenes, lignans, and isoflavones (2). These groups of compounds have been shown either in humans or laboratory experiments to have potential health benefits when included in the diet (2). Studies have shown consistent inverse association between cancer risk and the consumption of fruit and vegetables, β-carotene, vitamin C, and selected flavonoids (120). Some studies have focused on the examination of foods containing specific vitamins or phytochemicals, while others have focused on the consumption of fruit and vegetables in general. There have been no adverse effects reported from consuming fruit and vegetables. Non-starchy vegetables, such as lettuce, cucumbers, and celery, are associated with a probable decreased risk of mouth, pharynx, larynx, esophageal, and stomach cancers (2); there is a limited – suggestive decreased risk for nasopharyngeal, lung, colorectal, ovarian, and endometrial cancers (2). Allium vegetables, such as onion and garlic, are associated with a probable decreased risk of stomach cancer, and garlic-alone is associated with a probable decreased risk of colorectal cancer (2). Carrot consumption has a limited – suggestive decreased risk for the development of cervix cancer (2)
Fruit consumption is associated with a probable decreased risk for mouth, pharynx, larynx, esophageal, lung, and stomach cancers and has a limited – suggestive decreased risk for nasopharyngeal, pancreatic, liver, and colorectal cancers (2, 105). Cruciferous vegetables, carrots, fruits and the selenium content of these foods have been associated with a decreased risk of bladder cancer (121).
The recognized effect of consuming fruit and vegetables on lowering the risk of colon cancer may be partly attributed to salicylates in plant-based foods. Salicylic acid is widely present in plants and functions as a hormonal mediator of the systemic acquired resistance response to pathogen attack and environmental stress (122). Berries are thought to reduce cancer incidence, probably due to its high content of dietary antioxidant. In general, fruit and vegetables consumption decreases cancer risk probably due to high fiber content, high antioxidant activity mediated by flavonoids and salicylic acid content (122).
Lipids/fats. Consumption of mono-unsaturated fats (olive oil) is inversely associated with cancer risk (123). It has been hypothesized that the anticancer actions of olive oil is based on the ability of its mono-unsaturated fatty acid, oleic acid, to regulate oncogenes (119). The available prospective data from epidemiological studies and intervention trials do not support the overall hypothesis that high fat intake is a relevant risk factor for breast cancer development. In fact, the relative distribution of various fatty acids seems to be more important (124). Experimental data have shown that the influence of dietary fats on cancer depends on the quantity and the type of lipids. According to the “Joint FAO/WHO Expert Consultation on Fats and Fatty Acids” there is insufficient evidence that high intake of n-6 PUFAs and saturated fat has tumor-enhancing effects (51). On the other side, n-3 PUFAs, conjugated linoleic acid, and gamma linoleic acid have inhibitory effects (125). Rather than a single fatty acid, a composite indicator combining elevated mono-unsaturated and low n-6/n-3 PUFA ratios seems to be associated with breast cancer protection (126). Instead of the inaccurate assessment of the exact composition of fat intake it is suggested to determine the fatty acid composition of white adipose tissue as a biomarker of past lipid intake (126). This lipid profile, called the lipidome, may become the template for identifying breast cancer risk related to diet and for designing proper dietary modifications to delay the occurrence of breast cancer (126). Dietary sources of n-3 PUFAs include fish, chicken, eggs, canola oil, and soybean oil. Most Americans do not consume the recommended nutrient intakes of fats. The mean n-3 PUFAs consumption for Midwestern American women during pregnancy is only 78% of the recommendation from the “Canadian Recommended Nutrient Intake” and women at risk for breast cancer consume only 50% of the recommended dietary intake (127). Both n-3 PUFAs and n-6 PUFAs are essential fatty acids necessary for human health. Currently, the Western diet contains a disproportionately high amount of n-6 PUFAs and a low amount of n-3 PUFAs, and the resulting high n-6/n-3 PUFA ratio is thought to contribute to cardiovascular disease, inflammation, and cancer (128). Some studies suggest that this ratio is not a useful measure as it is not related to the absolute amounts (129). The n-3 PUFAs found in fish inhibit the growth in vitro of colon, breast, and prostate cancer cells lines (128). Olive oil and other mono-unsaturated and poly-unsaturated fats appear to have preventive effects on the development of breast, ovarian, colorectal, and upper aerodigestive tract cancers (123). It is suggested that olive oil can contribute to the reduced risks of breast cancer, possibly due to its high content of monounsaturated fat and antioxidants (130).
Antioxidants. Oxidative stress is referred to as an imbalance in the body of pro-oxidants over antioxidants (131). Pro-oxidant is a substance that can produce reactive oxygen species that can possibly damage cells. Oxidative stress produced by free radicals gives rise to DNA damage, including the highly mutagenic adduct 8-oxo-guanine (132), and the development of several diseases, including cancer (133). Antioxidants can counteract the damaging effects of oxidative species and are commonly added to food products such as vegetable oils and prepared foods to prevent or delay their oxidative deterioration during storage. Antioxidants are vitamins (such as β-carotene, vitamin C, and vitamin E), vitamin co-factors and minerals (such as co-enzyme Q10 and manganese), hormones (such as melatonin), carotenoids (such as α- and β-carotene), flavonoid polyphenols (such as quercetin and catechin), phenolic acids and their esters (such as chicoric acid and gallic acid), other non-flavonoid phenolics (such as curcumin, eugenol, and resveratrol), and other potential organic antioxidants (such as bilirubin, citric and oxalic acids). The best dietary sources of antioxidants are vegetables, beans, fruit, teas, spices, and herbs. Generally, antioxidant activity can be determined by oxygen radical absorbance capacity (ORAC), a method of measuring antioxidant capacities in biological samples in vitro and providing an artificial index of antioxidative strength (134). Recently however, the Nutrient Data Laboratory of the United States Department of Agriculture removed the “ORAC Database for Selected Foods” from its website due to increasing evidence that the values indicating antioxidant capacity have no relevance to the effects of specific bioactive compounds in foods on human health (135). Even though the mechanism of how flavonoids and other polyphenols work in vivo is unknown, epidemiological studies have clearly shown that consumption of foods high in dietary antioxidants has preventive effects against the development of many diseases, including cardiovascular diseases and cancer (136). Antioxidants such as vitamin E, β-carotene, lycopene, and selenium have been associated with reduced side-effects of chemotherapy when ingested by prostate cancer patients (137). Increasing concentrations of serum α- and γ-tocopherols, and higher dietary intakes of dark green and deep yellow vegetables and fruit, were associated with a nearly 50% decreased risk of cervical intraepithelial neoplasia grade 3 (138). These findings support the evidence that a healthy and balanced diet that provides high serum levels of antioxidants may reduce the risk of cervical neoplasia, one of the most common cancers in women living in low-income countries (138).
Vitamins and minerals. Vitamin D/calcium: The role of vitamin D in cancer prevention is well-documented in the literature (139-140). Vitamin D deficiency is common and is linked to cancer (141). The most understood functions of vitamin D are maintaining calcium and phosphorus homeostasis. Vitamin D insufficiency is linked to an increased risk of osteoporosis, diabetes, autoimmune disorders, and cancer. Sun exposure is the best way to obtain sufficient vitamin D (142), dietary sources are usually insufficient (143). However, excessive sunlight exposure carries an increased risk for skin cancer (144). A suggested way to increase dietary vitamin D is to fortify staple foods, use dietary supplements, and change dietary patterns to consume more fish (107). Vitamin D and dietary sources of vitamin D are inversely associated with the development of melanoma (109). Concerning calcium, the result of two cohort studies suggested an increased risk for prostate cancer at very high calcium intakes (>2,000 mg/day) (113). On the other side, calcium supplements pose a probable decreased risk for the development of colorectal cancer (2). Calcium and vitamin D are important agents for the primary prevention of colorectal neoplasia (48). We especially associate dairy with the benefit of dietary calcium. Even though milk is a rich source of calcium, it is not the only source. Vegetables like turnip greens or cooked turnips, watercress, broccoli, seeds and nuts and sardines are also rich in calcium (145). Consumption of food containing vitamin D has a limited – suggestive decreased risk for development of colorectal cancer (2).
Vitamin E (tocopherol): Dietary sources of vitamin E are poly-unsaturated plant oils, leafy green vegetables, whole grains, eggs, nuts, and seeds. The evidence for foods high in vitamin E is limited – suggestive for a decreased risk for the development of esophageal cancer (2). Vitamin E seems also to have a protective effect against the development of prostate cancer (113). α-Tocopherol supplements confer a limited – suggestive decreased risk for the development of prostate cancer (2, 113). Many large-scale intervention studies with α-tocopherol have not shown a strong cancer prevention effect. One possible explanation is that high doses of α-tocopherol decrease the blood and tissue levels of γ- and δ-tocopherol (146). While both α- and γ-tocopherol are potent antioxidants, γ-tocopherol has a unique function. Because of its different chemical structure, γ-tocopherol scavenges reactive nitrogen species, which, like reactive oxygen species, can damage proteins, lipids, and DNA. γ-Tocopherol, due to its anti-inflammatory activity, may be the most effective form of vitamin E in cancer prevention. A mixture of tocopherols rich in γ-tocopherol inhibits colon, prostate, mammary, and lung tumorigenesis in animal studies, suggesting that this mixture may have a strong potential for applications in the prevention of human cancer (146).
Vitamin A and β-carotene: Retinol (a form of vitamin A) is present only in animal-based foods, while β-carotene (a precursor of vitamin A) is found in plant-based food. Rich dietary sources of vitamin A include cheese, eggs, and liver; rich sources of β-carotene include leafy green vegetables, broccoli, cantaloupe, sweet potatoes, and carrots. Evidence suggests that foods containing carotenoids or β-carotene pose a probable decreased risk for cancers of the mouth, pharynx, larynx, esophagus, and lung (2). In contrast, the evidence is convincing that β-carotene dietary supplements increase risk for lung cancer (2). Retinol supplements have only limited – suggestive evidence for an increased risk for lung cancer and a decreased risk for skin cancer (2). Lycopene, a carotene found in tomatoes, has no vitamin A activity but does have a protective effect against prostate cancer (2, 113).
Vitamin C: Foods rich in vitamin C include citrus fruit, cabbage, dark green vegetables, cantaloupe, strawberries, and potatoes. These foods confer a probable decreased risk for esophageal cancer (2, 147) and have a borderline inverse association with prostate cancer (148). Vitamin C has a controversial history in cancer treatment: In the mid-late 1970s, Cameron and Pauling conducted a study on 100 patients with cancer demonstrating that vitamin C consumption at high doses of typically 10 g/day by intravenous infusion for about 10 days increased the average survival of advanced cancer patients (149). Later on, in the mid-1980s, three large placebo-controlled trials of only oral vitamin C were conducted in the Mayo clinic and found no positive effect of vitamin C in cancer patients (150-151). An explanation for the earlier results could be that the intravenous administration was found to increase plasma ascorbate concentrations by an order of magnitude compared to what should be achieved orally.
Vitamin C found at much higher doses than those in fruits and vegetables has been shown to cause increased cell death because of pro-oxidative effects at high concentrations. In the evaluation of antioxidant supplement safety, some effects of oxidative stress are natural and beneficial, like signal transduction via modulation of kinases or phosphatases and transcription factor activation leading to cell growth, proliferation and apoptosis. Moreover, there are naturally-occurring situations where pro-oxidative effects and reactive oxygen species are beneficial to the organism: the destruction of pathogens by the immune system, the detoxification of exogenous chemicals and the action of some chemotherapeutic agents which destroy rapidly dividing cancer cells (131).
The mechanism by which vitamin C can act as a pro-oxidant may be possibly due to its ability to regenerate vitamin E, which in excess can cause displacement of other important antioxidants, interference with essential defense mechanisms, such as apoptosis, damage to essential lipids and competition for absorption of other essential compounds. Ascorbic acid has been shown to reduce transition metals, such as ferric to ferrous and cupric to cuprous ions, whereby the ascorbate molecule is converted to dehydroascorbate via the Fenton reaction (131): Fe2+ + H2O2 → Fe3+ + OH• + OH−; 2 Fe3+ + ascorbate → 2 Fe2+ + dehydroascorbate + 2 H+.
In vitro experiments indicate that, in the presence of transition metals, ascorbic acid can readily switch from an antioxidant to a pro-oxidant. The concentrations at which this occurs will depend on the concentrations of metal and ascorbic acid in the solution. Potentially, in low ascorbate situations, this could lead to generation of superoxide and other reactive oxygen species. High concentration of transition metals will increase pro-oxidation by ascorbic acid. However, in vivo there usually are no free transition metals since they are bound to proteins, e.g. transferrin, lactoferrin, and ferritin in the case of iron (152). Patients with iron overload often have abnormal low contents of ascorbic acid in blood and tissues. Feeding them with ascorbate in the absence of the iron chelator desferoxamine can produce lethal consequences. Thalassemic patients with conditions of iron overload have died after ingestion of a high dose of vitamin C (152).
Other vitamins and minerals. Folate: Foods high in folate include fortified cereals, black-eyed peas, lentils, beans, spinach, asparagus, and broccoli (153). Foods containing folate are associated with a probable decreased risk for pancreatic cancer and a limited – suggestive decreased risk for the development of esophageal and colorectal cancer (2). Some studies suggest that diets high in folate or folic acid supplementation during pregnancy may reduce the risk of suffering from some childhood cancers (154-155). Suprisingly, in women taking high doses of folate throughout pregnancy a slight increase of the incidence of breast cancer was observed (156).
Pyridoxine: Foods containing pyridoxine (vitamin B6) were associated with a limited – suggestive decreased risk effect of esophageal cancer (2).
Selenium: Selenium is found as selenate/selenide in soil, thus vegetables and whole grains grown in areas where selenate/selenide in the soil is abundant will be a rich source of selenium. Other rich sources are seafood and meat. Selenium has cancer-preventive and cytoprotective activities in humans. It has roles in redox regulation, antioxidation, membrane integrity, energy metabolism, and DNA damage protection. Recent clinical trials also showed the importance of selenium in clinical oncology (157). There is sufficient evidence that food containing selenium probably decreases risk for the development of prostate cancer (113) while evidence is limited – suggestive for a decreased risk in the development of lung, stomach, and colorectal cancers (2). Supplements were found to have similar effects as foods high in selenium.
Many other vitamins and minerals are currently being studied in relation to cancer prevention and cancer risk, but the studies are not yet conclusive. A diet that includes fruits and vegetables contains vitamins, minerals and other bioactive nutrients. In recent years, with the use of advanced manufacturing technology such as isolation and purification, these vitamins and minerals have been made available in the form of dietary supplements. Approximately 47% of males and 59% of females in the US commonly use dietary supplements (158).
Beneficial effect of black and green tea. Tea is the most commonly consumed beverage around the world. Only limited evidence exists to show that green tea can reduce the incidence of liver cancer. The evidence for esophageal, gastric, colon, rectal, and pancreatic cancer is conflicting. There is a decreased risk for prostate cancer from observational studies for people consuming higher quantities of green tea or green tea extracts. There is limited to moderate evidence that the consumption of green tea reduces the risk of lung cancer, especially in men; and there is conflicting evidence regarding whether it reduces or increases the risk of urinary bladder cancer (159). Mate, a tea that is popular in Central and South America, may be drunk as a regular tea but is most commonly consumed highly concentrated and extremely hot. Drinking mate poses a probable increased risk for esophageal cancer and a limited – suggestive increased risk for mouth, pharynx, and larynx cancer (2).
Epigallocatechin 3-gallate (EGCG), a major catechin found in green tea, possibly plays a role in chemoprevention and chemotherapy of various types of cancers, mainly prostate cancer (160), and colon cancer (161). In vitro studies show that EGCG at high concentrations (10 to 1,000 μM) inhibits a wide range of biomedically-relevant molecular targets and disease-related cellular processes, including anticancer molecular targets (162-164). A smaller number of studies have shown that EGCG inhibits certain biomedically important molecular targets such as DNA methyltransferases, anti-apoptotic Bcl-2 protein and vascular endothelial growth factor receptor (VEGFR) signaling at lower concentrations (<10 μM) (165). EGCG may also help in protecting the skin from ultraviolet radiation-induced genotoxic damage and tumor formation (166). EGCG from green tea and supplements is now acknowledged as a cancer preventive in Japan and the concept of a cancer preventive beverage has been established (167). Pharmacokinetic studies conducted in humans show that the physiologically relevant serum concentrations of EGCG may be in the high nanomolar range (168). Therefore, high micromolar plasma concentrations of EGCG, necessary to cause the beneficial effects observed in vitro, are unlikely to be reached in the blood of individuals who drink tea (or ingest two to three 200 mg capsules of green tea extract each day) (168). Interestingly, the bioavailability of EGCG could be increased by peracetylation (169) of the catechin or by inhibition of enzymatic methylation (170) responsible for the metabolic inactivation of EGCG.
The discrepancies between in vitro and in vivo studies on the concentrations of EGCG consumed and their clinical effects can be linked to one of the following explanations: (i) The effects of EGCG may be more synergistic when it is combined with other catechins (171); (ii) EGCG and other tea catechins may be metabolically activated to form more potent bioactive compounds; (iii) EGCG could accumulate in tissues over time (172) to produce cellular concentrations that are higher than those observed in clinical serum samples; (iv) The observed effects of EGCG at high concentrations could be simply experimental artifacts that reflect the ability of catechins and other polyphenolic substances to act as metal chelators and bind to proteins in a nonselective manner.
The molecular mechanisms of the inhibitory effects of EGCG are not entirely clear. EGCG is a radical scavenger and, therefore, it is reasonable to suppose that it reduces endogenous oxidative stress. However, the effect might be much more complex. Thus, in a study by Shim et al. (173), it is reported that EGCG from green tea or the theaflavins from black tea inhibit tumor promoter-induced AP-1, NF-κB and MAP kinase activation as well as cell transformation. It was also shown that these two compounds have an inhibitory effect on UVB-induced STAT1 (Ser727), ERK, JNK, PDK1 and p90RSK2 phosphorylation. Recently, the intermediate filament protein, vimentin, and insulin-like growth factor receptor 1 (IGF-1R) were found to be novel EGCG-binding proteins. Vimentin has an important functional involvement in cell division and proliferation. EGCG has been reported to inhibit cell proliferation in a variety of cell lines and, when vimentin expression was suppressed, cell growth was inhibited (174). Thus, the anticancer effect of EGCG is likely based on a complex mechanism that involves radical scavenging and attenuation of signaling pathways that control cell proliferation and apoptosis.
Spices and herbs. Many spices and herbs or their bioactive components have medicinal properties, including cancer risk reduction due to their antimicrobial, antioxidant, or antitumorigenic properties, as well as direct suppressive effects on carcinogen bioactivation (175). Many of today's potent anticancer drugs originate from plants, especially plant alkaloids and terpenoids. These alkaloids block cell division by interfering with microtubule function or by inhibiting topoisomerase II. The main examples are vinca alkaloids (e.g. vincristine, vinblastine) from the Madagascar Periwinkle (Catharanthus roseus), taxanes (e.g. paclitaxel) from the Pacific yew (Taxus brevifolia) or glycosides of podophyllotoxin (e.g. etoposide, tenoposide) derived from the mayapple (Podophyllum peltatum) (176).
There are many studies currently in progress focusing on the preventive and possible curative effects of some herbs and spices. Herbs and spices can modify microbiota, which can stimulate growth within organisms that protect against cancer or within microorganisms that may increase cancer risk. Culinary herbs and spices generally serve as antioxidants but may also serve as pro-oxidants at higher exposures. Curcumin, a derivative of the Indian spice turmeric (Curcuma longa), shows promise in treating patients with head and neck cancer (177). In addition, recent findings show that curcumin could be used for breast cancer patients as a novel anticancer therapeutic (178). Finally, curcumin induces autophagy and shows promise in treating glioblastoma (179) and oesophageal cancer (180).

Diagram of food pyramid modified in respect to cancer prevention.
Recently, saffron (Crocus sativus), the most expensive spice in the world, by weight known for its anti-cancer properties, has attracted much attention in cancer prevention. It has been shown that saffron has a potent chemopreventive effect against hepatocellular carcinoma through the induction of apoptosis (181). Moreover, saffron shows toxicity in different types of malignant cells, in which programmed cell death plays an important role (182-184). Saffron thus holds the potential of treating cervical, liver, breast, and lung cancer. Finally, crocetin, a compound derived from saffron, showed a substantial antitumorigenic effect on pancreatic cancer in vitro and in vivo in mice (185).
Another natural product, silibinin, a compound derived from the milk thistle (Silybum marianum), potently reduced the growth of human hepatocellular carcinoma xenografts in nude mice (186). Moreover, xanthohumol, a chalcone present in hops (Humulus lupulus L.), exceeded silibinin's effectiveness in inhibiting the proliferation of hepatocellular carcinoma cell lines (187). A study presented in 2007 showed antiproliferative and apoptotic effects of chamomile (Matricaria chamomilla), a popular herb, in various human cancer cells (188). Recently, carvacrol, a chemical present in the popular seasoning oregano (Origanum vulgare) was identified to cause apoptosis in hepatocellular carcinoma cells (189).
The Mediterranean herb rosemary (Rosmarinus officinalis) was found to suppress skin tumorigenesis in mice (190). In addition, rosemary extracts inhibit the growth of human cancer cell lines of lung, prostate, liver, breast, and myeloid leukemia (191). Moreover, carnosol, responsible for 90% of the antioxidant activity of rosemary, shows inhibitory effects in human prostate cancer cells (192). Finally, the review of all studies on the protective effects of rosemary, published from 1996-2010, prompted the authors to suggest the use of rosemary and its active constituents in clinical cancer chemoprevention trials (193).
Ginger (Zingiber officinale) exhibited potential as a colon cancer preventive agent (194). In addition, ginger extracts induced apoptosis in hepatoma HEp-2 cells mediated by reactive oxygen species (195) and inhibited growth of ovarian cancer cells (196). Taiwanese researchers investigated the anticancer effect of 6-shogaol, an active constituent of dietary ginger, in human non-small lung cancer A549 cells and found that this phenol induces autophagic cell death (197).
Fenugreek (Trigonella foenum graecum), a vegetable and spice known for more than 8,000 years, showed significant chemopreventive effects against breast cancer in rats (198). Moreover, the chloroform extract of fenugreek plant killed MCF-7 human breast cancer cells (199). Extracts of fenugreek seeds inhibited the growth of breast, pancreatic and prostate cancer cell lines (200) and had substantial inhibitory effects against human acute T lymphoblastic leukemia cell lines (201). Finally, the fenugreek constituent diosgenin showed potential as a novel colon cancer preventive agent (202).
Thymoquinone derived from the spice black caraway (Nigella sativa) inhibited tumor angiogenesis and tumor growth (203), induced apoptosis in various cancer cell lines (204) and revealed cytotoxic effects on hepatocellular carcinoma (HepG2) cells (205).
Caloric Restriction
It is well-known that caloric restriction in laboratory animals effectively decreases cancer risk by 40% and extends life span (206). Studies on humans are under way. One of these studies is the “Comprehensive Assessment of Long-term Effects of Reducing Intake of Energy”. This study has already confirmed that caloric restriction has a protective effect on risk factors of cardiovascular disease (207). Effects on cancer risk are not yet known.
Food and Childhood Cancer
In this last paragraph we wish to discuss briefly the role of food in childhood cancer formation and prevention. Cancer is the most common cause of disease-related death of children in the U.S.A. (208-209). Pediatric cancers are not generally thought to be environmentally induced (210); however, recent studies have focused on the protective effects of mothers consuming certain vitamins, especially folate (154-155) as well as vegetables and fruits (211-212) during pregnancy. Furthermore, breastfeeding, which is widely known to be the optimal method of providing adequate nutrition to an infant, may also be associated with prevention of certain types of cancers (213-215). As with obese adults, obese children are at higher risk for the development of cancer (216). Cancer prevention recommendations for children are similar to those for adults: keep weight in the healthy range, consume a healthy diet rich in fruit and vegetables, and maintain a lifestyle high in physical activity and low in environmental contaminants. Children are more susceptible than adults to environmental contaminants, because of their rapid development of organs and nervous system. Furthermore, children are potentially exposed to higher levels of carcinogens in food due to the higher requirements of calories per kilogram of their weight and, therefore, consuming higher amount of food per kilogram.
Conclusion
When we talk about prevention of cancer, we have to realize that complete prevention is impossible. Prevention with regard to cancer usually means postponing the beginning of cancer development; this is of particular concern as the aging population is growing and life expectancy is improving. Age is one of the strongest risk factors for cancer development. People who live longer have an increased risk of developing cancer later in their life. For example, Japan has the highest death rate related to cancer, but the Japanese also have one of the longest life spans. Therefore, even though the incidence is high, the onset is delayed to older age.
No single dietary factor can prevent or delay the occurrence of cancer (Figure 4). A comprehensive lifestyle change is important, including optimal diet, avoidance of smoking and alcohol consumption, prevention of weight gain, and maintenance of a reasonable level of physical activity. From limited published research, we know that the incidence of some childhood cancers can be decreased by breastfeeding and proper maternal nutrition during gestation, including a diet rich in fruit and vegetables in addition to vitamin supplementation including folic acid. Regarding adult cancer and diet, the amount of research is overwhelming, and some of the evidence is convincing that diet plays an important role in cancer development in adulthood. The most significant diet-related risk factor for cancer development is obesity. There is more evidence about the benefits of some food groups than about the risk of other food groups (for a compilation see Table I). Cancer incidence is lower in people consuming mainly a plant-based diet, including high intake of fruits and vegetables, whole grains, and fish with a low n-6/n-3 PUFA ratio. In contrast, people consuming a diet high in meat, especially processed meat, and high in fat, sodium, and alcohol tend to have a higher incidence of cancers. People with a low body mass index and women breastfeeding their children tend to have lower cancer risk than people who are overweight or obese and women who did not breastfeed. The most significant diet-related prevention factor is keeping weight within a healthy range, meaning a body mass index between 18.5-24.9 kg/m2 during their adult life. Dietary changes are one of the most important and at the same time cheapest prevention tools we have regarding modification of cancer risk. More attention should be paid toward prevention of cancer by educating the public about the importance of diet in cancer development and research on how diet influences its development.
Categories of food with the most prominent anticarcinogens.
Acknowledegments/Disclosures
The Authors report no conflicts of interest in this work. This article was sponsored by the American Lebanese Syrian Associated Charities of St. Jude Children's Research Hospital. The Authors would like to acknowledge David Galloway, Senior Scientific Editor at St. Jude Children's Research Hospital, for editing. Thanks are also due to Angelika Will for valuable help in the literature search.
Footnotes
-
This article is freely accessible online.
- Received August 29, 2012.
- Accepted September 10, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The relationship between diet, plasma glucose, and cancer prevalence across vertebrates
- The ecology of cancer prevalence across species: Cancer prevalence is highest in desert species and high trophic levels
- Plant-Based and Plant-Rich Diet Patterns during Gestation: Beneficial Effects and Possible Shortcomings
- 3,6-Dihydroxyflavone Suppresses Breast Carcinogenesis by Epigenetically Regulating miR-34a and miR-21