


Abstract
The prognosis of patients with glioblastoma is extremely poor despite multimodal treatments including surgery, chemotherapy and radiotherapy. Recently, the alkylating agent, temozolomide (TMZ) has been shown to improve survival in patients with malignant gliomas, including those with glioblastoma in some clinical studies, and has become one of the standard modalities for treatment of newly diagnosed and recurrent malignant gliomas. The epigenetic silencing of the DNA repair enzyme O6-methylguanine-DNA-methyltransferase (MGMT) is the strongest predictive marker for favorable outcome in patients treated with TMZ. However, it remains to be determined how patients with tumors lacking MGMT promoter methylation should be treated. Moreover, even patients with TMZ-sensitive glioblastoma cannot avoid eventual recurrence. In this article, we review the mechanism of the effect of TMZ on tumor cells and resistance to TMZ, and provide an overview of the current management and trials for patients with glioblastoma.
Glioblastoma (glioblastoma multiforme, GBM) is the most frequent and malignant subtype of glioma, and is classified into grade IV of the World Health Organization (WHO) grading system (1). Anaplastic astrocytoma, anaplastic oligodendroglioma and anaplastic oligoastrocytoma are classified into grade III; grade III and IV gliomas are designated as high-grade gliomas or malignant gliomas. Despite innovations in neurosurgical techniques, developments of new anticancer drugs and molecular targeted drugs, and advances in radiotherapy over the past decades, malignant gliomas, especially GBM, remain fatal diseases. Although patients with malignant gliomas have been treated with combined radiotherapy and chemotherapy using regimens such as PCV-3 (procarbazine, lomustine, and vincristine) (2), no regimen has demonstrated a significant beneficial improvement of median survival relative to radiotherapy alone. Temozolomide (TMZ) is the only anticancer drug that has been shown in a phase III study to improve survival in GBM when administered with concomitant radiotherapy (3). TMZ is an oral alkylating agent that leads to cell death by alkylation of the O6 position of guanine and subsequent disturbance of DNA replication (4). The DNA repair protein O6-methylguanine-DNA methyltransferase (MGMT) has been implicated in the resistance of tumor cells to alkylating agents (5). MGMT is expressed in gliomas and its contribution to resistance to TMZ has been reported (6-12). To date, many clinical trials have aimed to reduce TMZ resistance. In this article, we review the mechanism of anticancer action and the clinical trials of TMZ, and summarize current concepts of chemotherapy in the context of a multidisciplinary approach to GBM.
Mechanism of Anticancer Action of TMZ
TMZ is an analog of mitozolomide, one of the antitumor imidazotetrazines which were synthesized by Stevens et al. in the 1980s (13). Although mitozolomide showed severe myelosupression in the phase I study (14), a 3-methyl derivative, TMZ showed less toxic effect and broad-spectrum activity in mouse tumors (15). A phase I trial also showed good tolerances and responses in patients with melanoma and patients with recurrent malignant gliomas (16). Orally administered TMZ is converted to 5-(3-methyltriazen-l-yl)imidazole-4-carboximide (MTIC) in water/blood with little or no enzymatic component (4, 17, 18). MTIC is broken down to methyldiazonium cation and 5-aminoimidazole-4-carboxamide (AIC) (18). AIC is excreted via the kidneys and methyldiazonium cations deliver methyl groups to DNA (4, 18). These methyl groups are transferred to the 6th position oxygen atoms of guanine and O6-methylguanines are formed. O6-Methylguanine mispairs with thymine instead of cytosine during DNA replication. The O6-methylguanine:thymine mispair can be recognized by the post-replication mismatch repair system, which removes a daughter strand along with the thymine, leaving the O6-methylguanine to again pair with thymine during gap filling. If replication of the gapped structure occurs, double-strand breaks can form. Unless repaired by the recombination repair pathways, they result in cell death (Figure 1). Because this cytotoxity is replication-dependent, methylating agents including TMZ are more effective on tumor cells than on quiescent cells (18, 19).
MGMT Expression and Resistance to TMZ
MGMT is a DNA repair protein which reverses alkylation at the O6 position of guanine to compensate for the effect of alkylating agents (19) (Figure 1). Human MGMT cDNA was isolated from a cDNA library by selection according to the phenotype to tolerate alkylating agents much like for O6-alkylguanine-DNA alkyltransferase of Escherichia coli (20). Expression of MGMT differs according to species, organs, kinds of tumor and cell lines. In the early 1990s, the low-MGMT expressing subsets of cell lines, termed Mer− strains, were investigated to clarify the mechanism of reduced expression of MGMT, and correlation between DNA methylation and expression of MGMT was revealed (21). As deletion, mutation, rearrangement and mRNA instability of the MGMT gene are rare events (22-26), hypermethylation of the CpG island has been reported as the essential mechanism for silencing of MGMT (8-11, 19, 21, 22, 27-29). Esteller et al. described that 40% of GBM cell lines, 50% of anaplastic astrocytoma cases, and 41% of GBM cases showed MGMT promoter methylation (22). The incidence of MGMT promoter methylation in patients with GBM was 45% in the European Organization for Research and Treatment of Cancer (EORTC) trial and the National Cancer Institute of Canada (NCSC) trial (9). These trials revealed that patients with GBM containing a methylated MGMT promoter benefited from TMZ (9). In addition to the aspect regarding TMZ sensitivity, the methylation-mediated silencing of MGMT is important in the biology of GBM cells, as it may cause another mutation of gene involved in tumor progression, such as TP53 and K-ras (30-35).
MGMT protein and mRNA levels in tumor tissues can be evaluated by immunohistochemistry (36), and reverse transcription-PCR (RT-PCR)/real-time RT-PCR (37, 38), respectively. The activity of MGMT is measurable by an enzyme assay (39). The methylation status of the MGMT gene has been assessed with methylation-specific PCR using bisulfite-modificated DNA samples (10). For diagnostic purposes, the methylation-specific PCR is of advantage compared with the measurement of MGMT protein activity or mRNA level because tissue contamination of non-neoplastic cells does not interfere with the detection of genomic methylation in tumor cells (40, 41). Additionally, it is difficult to apply immunohistochemistry to assess MGMT expression for diagnostic purposes as the immunostaining procedures and antibodies might differ between different laboratories. At any rate, a standardized and validated method for the evaluation of MGMT status is required for the diagnosis and the prognostication of gliomas.
Treatment before TMZ
The standard treatment for malignant gliomas is surgery followed by chemotherapy with radiotherapy. Optionally, boost radiotherapy or chemotherapy is added, and stereotactic radiotherapy or chemotherapy is performed as a salvage therapy at recurrence/regrowth (42, 43). Regarding surgery, gross total resection is directly associated with longer survival, compared to subtotal resection (44), and novel modalities such as contrast-enhancing agents (45), navigation systems, and intraoperative monitoring systems (46) improve the performance of surgery. However, quite a few patients with malignant gliomas will have residual tumors because the brain is a vital organ and many tumors are located in eloquent regions of the brain, consequently, complete resection is often unattainable. No matter how the surgical technique develops, patients with malignant gliomas cannot be cured by surgery alone. In the late 1970s, it was reported that the addition of radiotherapy to surgery was more beneficial than surgery alone for patients with malignant gliomas (47), and patients who were treated with 60 Gy-dose radiotherapy showed longer survival than those with lower dose radiotherapy (48). Although many trials of boost fractionation or radiosurgery following conventional radiotherapy were performed, No significant survival improvement was achieved compared with conventional radiotherapy alone (49-52).
Chemotherapy is expected not only to be a cytotoxic modality for malignant gliomas but also to sensitize the tumor cells to radiation effects. Before TMZ, hydroxyurea, nitrosoureas such as carmustine (BCNU), lomustine (CCNU) and nimustine (ACNU), and procarbazine were used for adjuvant chemotherapy for patients with malignant glioma (43). Nitrosoureas (alkylating agents like TMZ) and procarbazine were commonly used. The Brain Tumor Study Group revealed that intra-arterial administration of BCNU does not yield more favorable results than intravenous administration (53). PCV-3 was only a combination chemotherapy regimen, which showed more beneficial survival and time to progression in patients with anaplastic astrocytoma than single agent and radiotherapy alone (2, 54). The median survival of patients with anaplastic astrocytoma treated with PCV-3 was 157 weeks and that of those treated with BCNU was 82.1 weeks; time to progression was also doubled. On the other hand, there was no statistically significant difference in survival of patients with GBM (median survival duration, 50.4 weeks with PCV and 57.4 weeks with BCNU) (2). In spite of the results in GBM, PCV-3 has been used most extensively for treatment of malignant gliomas for a long time. As recent studies have demonstrated that loss of heterozygosity (LOH) on chromosome 1p and 19q in anaplastic oligodendroglioma predicts sensitivity to chemotherapy and better overall survival (55, 56), PCV-3 is preferably used for patients with malignant gliomas with oligodendroglial components. In Japan, some groups perform IAR (interferon-β, ACNU and radiation) therapy for malignant gliomas, which is designed as an antitumor therapy with biological modulation. Although no data of any randomized large-scale clinical study are available for this therapy at present, a certain degree of improvement appears to be observed compared with the previous outcome (57, 58). Until the phase III trial of radiotherapy plus TMZ showed the median survival benefit (14.6 months), the median survival of GBM had been less than one year (3).
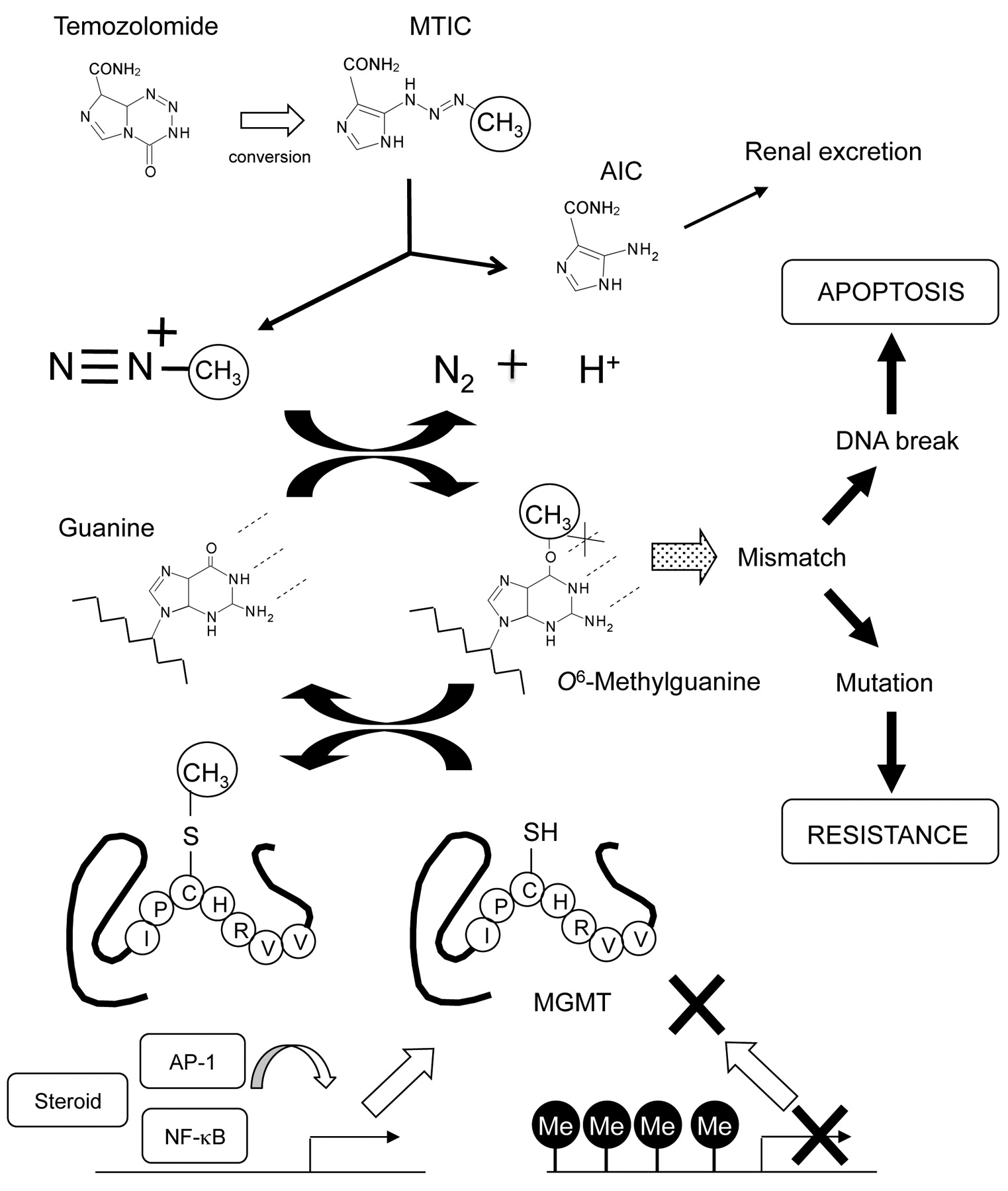
TMZ is converted to 5-(3-methyltriazen-l-yl)imidazole-4-carboximide (MTIC) in water/blood with little or no enzymatic component. MTIC is broken down to methyldiazonium cation and 5-aminoimidazole-4-carboxamide (AIC). AIC is excreted via the kidneys and methyldiazonium cations deliver methyl groups to DNA. Methyl groups are transferred to the 6th position oxygen atoms of guanine and O6-methylguanines are formed. O6-Methylguanine mispairs with thymine instead of cytosine during DNA replication. The O6-methylguanine causes DNA break and apoptosis. MGMT removes methyl groups from O6-methylguanines to repair the genome. The expression of MGMT is epigenetically controlled by some kinds of transcription factors or hormones. If the promoter region is methylated, the expression of MGMT is kept at a low level. Abbreviations, MTIC, 5-(3-Methyltriazen-l-yl)imidazole-4-carboximide; AIC, 5-aminoimidazole-4-carboxamide; MGMT, O6-methylguanine-DNA methyltransferase; Me, methyl group; AP-1, activator protein-1; NF-κB, nuclear factor kappa B.
Clinical Studies of TMZ and Chemoresistance to TMZ
The TMZ therapy according to the regimen of Stupp et al. (3) is a standard first-line chemotherapy of malignant gliomas. In addition, various new attempts have been performed to overcome TMZ chemoresistance. Recent phase II and III studies of first-line treatment for GBM (59-69) and of treatment for the recurrent GBM (70-83) are shown in Tables I and II, respectively.
Gliadel wafer is a polymer implant conjugated with BCNU, which is used for local delivery of BCNU to the resection surface intraoperatively. Surgery with Gliadel wafers followed by standard TMZ administration plus radiotherapy may show relatively favorable outcome, but the scale of the clinical trials is small and not double-blind studies (60, 62). Epidermal growth factor receptor (EGFR) amplification is observed 34% of GBM, and the mutation or amplification of EGFR plays important roles in progression of GBM (84). Erlotinib is a tyrosine kinase inhibitor and inhibits EGFR selectively. Although no adverse event occurred even with TMZ therapy (63), apparent benefit was not detected in overall survival (61, 63, 73). Erlotinib has insufficient effects on unselected GBM cases. Imatinib is also a tyrosine kinase inhibitor and shows a favorable effect only on subsets of patients (82). Bevacizumab is also a tyrosin kinase inhibitor which represses vascular endothelial growth factor selectively. A small-scale study showed favorable efficacy of bevacizumab on GBM when combined with TMZ and radiotherapy (64). Although thalidomide and celecoxib were also expected to have an antiangiogenesis effect on tumors, no beneficial effect on survival has been observed (66).
It had been reported that combinations of alkylating agents such as TMZ and BCNU depleted MGMT activity and increased antitumor activity of each other (85). However, a phase II trial revealed that BCNU plus TMZ had only a modest effect, with significant toxicity, and appeared to be no more effective than single-agent TMZ (83). Anticancer drugs with different mechanisms of action from TMZ, such as cisplatinum, irinotecan, teniposide, procarbazine, and hydroxyurea, biomodulator (polyinosineic-polycytidylic acid stabilized with polykysine and carboxymethylcellulose and interferon), and matrix metalloprotease inhibitor (marimastat) were used as investigational agents, however, no satisfactory benefit was obtained. The enzyme activity of MGMT is the most important mechanism underlying the resistance to TMZ. However, other unknown mechanisms may exist because some cell lines with low MGMT expression still show significant resistance to TMZ. Disturbance of the mismatch repair system is one of the mechanisms of TMZ resistance (86-88). Moreover, nucleotide excision repair system may also be involved in TMZ resistance. Some human tumor cells treated by TMZ show increased expression of chromatin-associated gene poly(ADP-ribose) polymerase-1 (PARP), which is involved in nucleotide excision repair (89). PARP inhibitor enhanced sensitivity to TMZ both in vitro (90, 91) and in vivo (92, 93), thus the clinical usefulness of this compound should be evaluated. An ATP-competitive small-molecule inhibitor (94) and a gastrin-releasing peptide receptor antagonist (95) also showed antitumor effects in combination with TMZ in vitro and in vivo experiments. Interleukin-24 is reported to have the ability to inhibit MGMT in human melanoma cells (96).
Chemoresistance and Glioma Stem Cells
Recently, evidence supporting the cancer stem cell concept has been increasingly provided. A relationship between the chemoresistance of cancer cells and stemness has been suggested repeatedly. Cancer stem cells show multidrug-resistant phenotype by overexpressing drug transporters such as adenosine triphosphate-binding cassette (ABC) superfamily, vaults such as lung resistance-related protein/major vault protein (LRP/MVP), and anti-apoptotic protein such as B-cell lymphoma/leukemia-2 (bcl-2). Glioma stem cells are also believed to exist and show the multidrug-resistant phenotype, and thus would be important therapeutic targets (reviewed in 97). Analysis of neural stem cells and sorted cells using neural stem cell marker CD133 revealed the existence and features of brain tumor stem cells (or glioma stem cells) (98). It is reported that one of the ABC superfamily, multidrug resistance 1 (MDR1), plays an important role in the chemoresistance of GBM independent of MGMT status, and a single nucleotide polymorphism status of the MDR1 gene dictates TMZ sensitivity (99). CD133 expression as a signature of stem cell phenotype is reported to be a candidate predictor for poor survival in patients with GBM treated with concomitant TMZ chemoradiotherapy (100). On the other hand, it has been reported that TMZ administration can reduce the number of glioma stem cells (101).
Recent phase II and III studies of first-line treatment of glioblastoma.
Recent phase II studies of recurrent glioblastoma.
TMZ Sensitivity and p53
P53 is a pleiotropic molecule and plays an important role in DNA repair and apoptosis with a different mechanism from MGMT. Wild-type p53 can reduce the level of MGMT in cells in vitro (102). Conversely, in another report, p53 directly induced MGMT expression in murine astrocytic glioma cells (103). Moreover, p53 inhibitor enhanced the effect of TMZ in a mouse intracranial tumor implantation model, suggesting that p53 may induce MGMT to regulate TMZ sensitivity negatively (104). Although p53 plays a protective role against cell death on treatment with chloroethylating agents, this is not the case in the treatment with methylating agent (105). Collectively, the roles of p53 are complicated and diverse depending on cell type, status of p53 (wild or mutant) and the kind of antitumor agent used.
Conclusion
Although the improvement of outcome of GBM patients by the new alkylating agent TMZ has an impact on treatment of malignant gliomas, GBM is still an incurable disease. Breakthrough is required for therapeutic modalities. Much remains to be clarified; the mechanism of chemoresistance and the roles of related molecules including MGMT, mismatch repair enzymes, DNA excision repair enzymes, PARP, p53, ABC superfamily, and apoptosis-related factors. Not only approaches to increase sensitivity to TMZ but also understanding the cellular biology underlying chemoresistance and the stem cell phenotype will lead us to a complete cure of GBM.
Acknowledgements
This work was supported by Grant-in-Aid for Young Scientists (B) No. 20790307 and Grant-in-Aid for Scientific Research (B) No.20390114 from the Ministry of Education, Culture, Sports, Science, and Technology, Japan.
- Received April 28, 2009.
- Revision received July 20, 2009.
- Accepted August 13, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- A Cancer Research UK First Time in Human Phase I Trial of IMA950 (Novel Multipeptide Therapeutic Vaccine) in Patients with Newly Diagnosed Glioblastoma
- NEO212, Temozolomide Conjugated to Perillyl Alcohol, Is a Novel Drug for Effective Treatment of a Broad Range of Temozolomide-Resistant Gliomas
- Apparent Diffusion Coefficient Histogram Analysis Stratifies Progression-Free Survival in Newly Diagnosed Bevacizumab-Treated Glioblastoma