


Abstract
Background: The prognostic value of vascular endothelial growth factor-A (VEGFA) and epithelial cadherin (E-cadherin) expression in patients with metastatic colorectal cancer (mCRC) is controversial. Materials and Methods: In this prospective study, patients diagnosed with mCRC between August 1, 1998, and August 30, 2003, at the Turku University Hospital, Finland were included. Expression of E-cadherin (membranous and cytoplasmic pattern) and VEGFA in tumour samples was assessed by immunohistochemistry. Tumours were classified as E-cadherin expressers if they demonstrated moderate or strong cytoplasmic or membranous staining, while those positive for VEGFA expression showed a moderate or strong cytoplasmic staining. Of particular interest was the association between membranous or cytoplasmic expression of E-cadherin and VEGFA. The value of strong VEGF-A staining and membranous or cytoplasmic expression of E-cadherin as a predictor of disease outcome over a 6-year period was another point of interest in this study. Results: Of the 67 patients with mCRC, 43 (64%) had tumours positive for cytoplasmic E-cadherin, while in 24 cases (36%), E-cadherin expression was membranous. Strong VEGFA staining was present in half of the cases (n=36, 54% of all 67 mCRC cases). VEGFA expression was significantly correlated with cytoplasmic E-cadherin expression in that 28/36 cases of VEGFA-positive tumours were also positive for cytoplasmic E-cadherin (p=0.012). In addition, among the patients with intense VEGFA expression (n=36), those who had positive cytoplasmic E-cadherin in their tumours had a lower response-rate to first-line therapy with irinotecan, fluorouracil and leucovorin regimen: 5 out of 36 (14%) were chemosensitive. This is in contrast to the patients with VEGFA-positive tumours and membranous E-cadherin (8/36, 22% chemosensitive (p=0.004). The former group also had more ominous prognosis (p<0.001). Conclusion: Reduced membranous expression of E-cadherin and increased cytoplasmic E-cadherin expression predict poor survival in mCRC.
Colorectal cancer (CRC) is the third most common cancer (1), and is one of the leading causes of mortality and morbidity worldwide (2). Although comprehensive treatment is available, including curative resection and chemotherapy, the prognosis of CRC is still far from optimal. Several common clinicopathological factors, such as tumour grade, perineural and lymphovascular invasion, microsatellite instability status, Kirsten rat sarcoma viral oncogene (KRAS), neuroblastoma RAS viral oncogene homolog (NRAS), and v-raf murine sarcoma viral oncogene homolog B (BRAF) mutations, circumferential resection margin, and carcino-embryonic antigen (CEA) have been extensively tested as prognostic predictors (3, 4). Some of these factors can be useful in the selection of patients for treatment but most of them are of limited value in predicting the individual response to treatment or overall outcomes. Therefore, the search still continues for new prognostic markers to guide therapy and improve the survival rates of patients with CRC. The idea of finding a single marker suitable for all purposes is obsolete, and the goal should be to move towards a personalizedtherapy of patients, based on prognostic markers that should accurately predict the response to therapy.
E-Cadherin, a metastatic suppressor gene, is a calcium-dependent adhesive protein responsible for epithelial cell cohesion and also participating in cellular signalling, albeit the nature of these intracellular signalling pathways has not been fully elucidated. However, increasing evidence assigns an important role to activation of the WNT signalling pathway and its major mediator cadherin-associated protein, β-catenin, in normal and pathogenic angiogenesis (5). Given that adenomatous polyposis coli (APC) is a tumour suppresser in human colon cancer and its mutation enhances β-catenin gene expression (6, 7), there is increasing evidence to suggest an involvement of the cadherin/catenin complex disruption in a variety of human cancer types (8-10). It was reported that increased cytoplasmic staining of cadherin–catenin complex is an independent predictor of poor survival, whereas expression at the cell membrane is not (11, 12).
Overexpression of β-catenin also produces an increase in cellular vascular endothelial growth factor A (VEGFA) protein (13), a key mediator of angiogenesis (14). VEGFA is regulated by few interacting cellular pathways such as transforming growth factor beta (TGFβ) signalling, WNT/β-catenin, and VEGF pathways that are necessary for embryonic vasculogenesis and angiogenesis (14). In particular, mutation in canonical WNT/β-catenin signalling components including APC, axin, and β-catenin have been reported in gastrointestinal malignancies (15), and results in hyperactivation of the WNT pathway, ultimately increasing proliferation of malignant cells and angiogenesis (13, 14). Experimental studies have demonstrated that β-catenin directly induces VEGFA expression when normal colon epithelial cells were transfected with mutant form of β-catenin gene (13). Therefore, β-catenin is known to have dual effects, regulating cell proliferation when in the nucleus and cell adhesion when at the cell surface, both key mediators of angiogenesis (14). Although the individual prognostic value of E-cadherin and VEGFA in patients with CRC has been studied (16, 17), the combined prognostic value of VEGFA and E-cadherin expression in patients with mCRC has not been evaluated, to our knowledge. In the present study, we analysed the prognostic role of E-cadherin and VEGFA in primary tumours resected from patients with CRC, with special reference to evaluating the association between their immunohistochemical expression pattern and patient outcomes.
Materials and Methods
Study population. The material of this study consisted of CRC specimens from 67 patients who had undergone resection at the Turku University Hospital between 1998 and 2003. Of the patients, 43 were men and 24 were women, aged 24-80 years (mean age=57.6 years; Table I). No patients had received irradiation or chemotherapy prior to resection. Forty-two patients were diagnosed as having metastatic disease at time of diagnosis (stage IV), while the remaining 25 patients with stage II (n=11) and III (n=14) developed metastasis later during the follow-up period. Written informed consent to participate in the study was obtained from each patient before surgery. The study was approved by the National Authority for Medico-Legal Affairs Committee, Finland and was conducted in accordance with the declaration of Helsinki.
Baseline characteristics of the study cohort (n=67).
Association between vascular endothelial growth factor A (VEGFA) staining and E-cadherin expression in patients with metastatic colorectal cancer

Overall survival of patients with metastatic colorectal cancer according to vascular endothelial growth factor A (VEGFA) expression.
Immunohistochemical staining. A formalin-fixed, paraffin-embedded primary tumour was obtained from each patient. Sections were cut serially at 5 μm for routine haematoxylin and eosin (HE) staining and for immunohistochemical analysis. An experienced pathologist confirmed all histological diagnoses. Evaluation and scoring of the immunohistochemical slides was carried out without knowledge of the clinical data.
Evaluation of E-cadherin expression. Expression of E-cadherin was studied using monoclonal mouse antibody to E-cadherin (Clone HECD-1, sub-class IgG1; Zymed Laboratories, San Francisco, CA, USA) at a dilution of 1:300 in phosphate-buffered saline containing 1% bovine serum albumin (1:50). Two independent observers assessed the expression of E-cadherin. The slides were first screened for an overview of the general staining pattern. Cytoplasmic expression of E-cadherin was recorded when staining was absent from the cancer cell membrane and preserved in cancer cell cytoplasm and nucleus.
Evaluation of VEGFA expression. For studying VEGFA expression, purified anti-human VEGFA (121, 165, and 189 isoforms) (clone VG-1; Biosite, San Diego, CA, USA) (1:150) was used. The expression of VEGFA in the tumour tissue was assessed according to the expression in the total tumour area. Only cytoplasmic staining was observed, and graded into four categories: negative, no detectable staining; weak but detectable staining; moderate, clearly positive staining; and strong staining, intense throughout the tumour.
Evaluation of patient response to the first-line therapy with irinotecan, fluorouracil and leucovorin IFL. All patient received IFL regiment once they developed metastasis. The IFL treatment was a combination of irinotecan (180-210 mg m−2, administered as a 60- to 90-min intravenous infusion) and 5-fluorouracil (500 mg m−2, i.v. bolus), modulated by leucovorin (60 mg m−2, i.v. bolus). The 5-flurouracil/leucovorin administration was repeated on the following day. This treatment combination was repeated every 2 weeks until disease progression or occurrence of unacceptable toxicity. Tumour response was assessed every 8 weeks by an independent reviewer according to WHO criteria (18, 19).

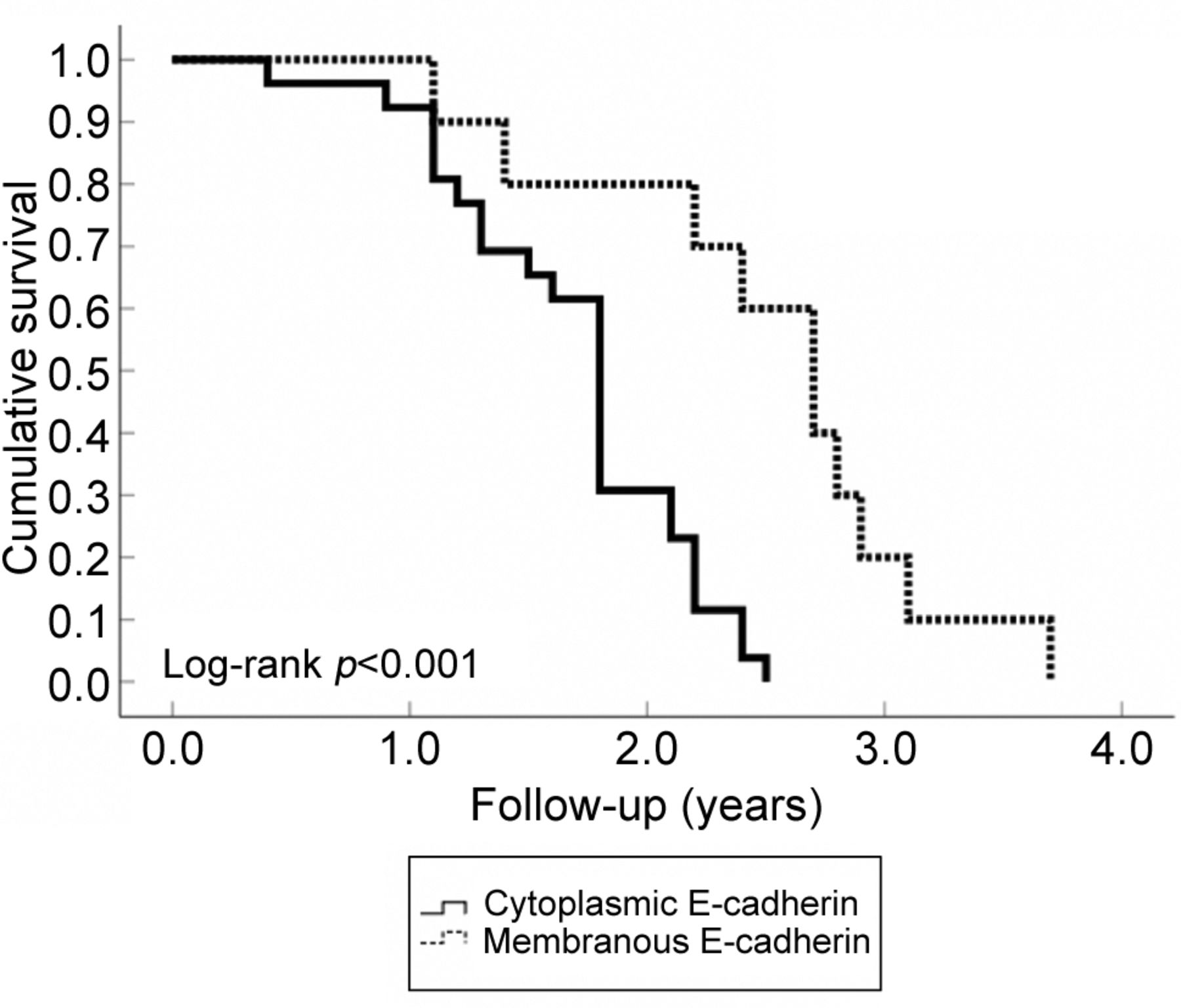
Overall survival of patients with metastatic colorectal cancer according to E-cadherin in patients with tumours with strong vascular endothelial growth factor A (VEGFA) expression.
Statistical analysis. All analyses were performed with SPSS 21.0 (IBM, Armonk, NY, USA), and Sample Power 3.0 (SPSS). Categorical variables are presented herein as percentages, and continuous variable (age) are presented as means (±SD). The age variable was checked for normal distribution using the Kolmogorov–Smirnov test. The expression of E-cadherin was used as a dichotomous variable, where tumours with nuclear, heterogeneous or cytoplasmic expression of E-cadherin were one category (cytoplasmic E-cadherin), and all those with well-localized membranous expression of E-cadherin were grouped into the second category (membranous E-cadherin). The expression of VEGFA was also classified as a binary variable, whereby tumours with negative or weak staining were considered as exhibiting weak VEGFA expression, and those with moderate or strong staining were considered as having strong VEGFA expression. Comparisons of categorical variables were performed using the chi-square test or Fisher's exact test. Survival curves were computed according to Kaplan and Meier; the log-rank test was used to examine the difference between the curves. A p-value of less than 0.05 was accepted as statistically significant for all tests.
Results
Patterns of E-cadherin expression. Of the 67 tumour samples studied, 43 cases (64%) showed cytoplasmic E-cadherin and 24 cases (36%) were positive for membranous E-cadherin. Correlation between VEGFA and E-cadherin expression. VEGFA was significantly correlated with cytoplasmic E-cadherin expression, with 28 out of 36 VEGFA-positive tumours showing cytoplasmic E-cadherin expression and only 8/36 showing membranous E-cadherin expression (Table II) (p=0.012).
Correlation between VEGFA and E-cadherin expression in relation with response to first line IFL and overall survival (OS). During the 6-year follow-up, 31 out of 67 patients responded to IFL regimen: 18 out of 31 were patients with weak VEGFA tumour staining, and 13 were patients with strong VEGFA tumour staining. Patients with strong VEGFA tumour staining had a lower OS rate following the first-line IFL regimen (all 36 had died, as compared to the patients with weak VEGFA tumour staining (28; 90% died) (p<0.001) (Figure 1). Among the patients with strong VEGFA tumour staining (n=36), those who had cytoplasmic E-cadherin-positive tumours had a lower response rate to the first-line IFL regimen (5/36, 14% were chemosensitive) as compared to those with VEGFA tumours with membranous E-cadherin expression (8/36, 22%; p=0.004). The former also had much worse prognosis (p<0.001; Figure 2).
Discussion
The present study provides new insights into the role of cytoplasmic E-cadherin as a marker of treatment response in mCRC. In the present series of 67 patients with mCRC, there was a significant association between cytoplasmic E-cadherin and VEGFA expression. Compared to the patients with tumours positive for membranous E-cadherin, the patients with cytoplasmic E-cadherin expression had a higher level of VEGFA co-expression, a lower response rate to the first-line IFL, and a poorer prognosis during the 6-year follow-up.
In this study, the cytoplasmic localization of E-cadherin was co-expressed with VEGFA, suggesting that loss of membranous E-cadherin promotes tumour angiogenesis. Similarly, Ceteci et al. who studied the role of E-cadherin in early development of lung cancer revealed that disruption of E-cadherin up-regulates angiogenesis target genes VEGFA and VEGFC, leading to massive intratumoural vessels formation in the early phase of tumour induction in RAF-driven murine lung cancer (20). In their study, β-catenin was identified as an effector of E-cadherin disruption. The simple fact is that E-cadherin traps β-catenin at the cytoplasm and loss of this interaction enables nuclear translocation of β-catenin and angiogenesis through WNT pathway activation (21). Moreover, in their study induction of VEGFA, not VEGFC was β-catenin-dependent (20). Consistent with data reported by Zhang et al., who demonstrated that VEGFA promotor activity could be stimulated by oncogenic β-catenin in HeLa cells (22), and by Easwaran et al., who described VEGFA as a direct target gene of β-catenin in human colorectal cancer cell lines (13). The reasonable explanation for these findings could be a signalling cascade connecting E-cadherin disruption via β-catenin with angiogenesis target gene VEGFA that can be considered as a hallmark of cancer progression.
Another noteworthy finding in our study is that among the patients with strong VEGFA expression, positive cytoplasmic E-cadherin expression was a predictor of chemotherapy-refractory status and more ominous prognosis, whereas membranous E-cadherin expression had no such associations. Consistent with other studies on different human cancer types, loss of membranous expression of E-cadherin was significantly associated with a lower response to chemotherapy and lower OS rate (23-25). There are several possible reasons associated with the chemotherapy-refractory status, one is loss of membranous E-cadherin or cell–cell junction efficiency in cancer cells resulting in derailed endocytosis of surface receptors and reduced effectiveness of chemotherapy drugs (26). Another involves disruption of E-cadherin activation of β-catenin signalling (20), which can profoundly affect the genetic composition of the tumour cells (5) and influence the response to chemotherapy. As an example, recent observations point to the fact that when the tumour-suppressor gene p53 is overexpressed as a defence mechanism against tumour growth, the oncogenic capabilities of β-catenin are reduced. There is a selective pressure for the tumours to inactivate p53 in order to sustain activation of the β-catenin signalling (27, 28). Therefore, this could be responsible for the lower response rate to irinotecan-based regimen because it has been demonstrated that irinotecan-induced apoptosis was inhibited by reduced p53 expression (29).
In conclusion, E-cadherin and VEGFA combination might be used as a prognostic marker in mCRC. Reduction in membranous expression of E-cadherin and increased cytoplasmic E-cadherin expression seem to predict poor survival in mCRC.
Footnotes
Authors' Contributions
Study design and experimental work: R.B.; Analysis and article writing: F.S.S. and N.S.S.; analysis and article revision: K.S. and S.P.
This article is freely accessible online.
Conflicts of Interest
There are no conflicts of interest regarding this study.
- Received January 22, 2019.
- Revision received March 9, 2019.
- Accepted March 13, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}