


Abstract
Background/Aim: ALK inhibitors like Crizotinib, Ceritinib and Alectinib are targeted therapies used in patients with anaplastic lymphoma kinase (ALK)-positive, advanced non-small cell lung cancer (NSCLC). Since in this tumor entity radiotherapy is employed sequentially or concomitantly, potential synergistic effects were investigated, which may support the hypothesis of induced radiosensitization by using ALK inhibitors. Materials and Methods: Two cell lines expressing wild-type (WT) or echinoderm microtubule-associated protein-like 4 (EML4)-ALK were treated with ALK inhibitors, followed by irradiation. Cell survival, cell death, cell cycle and phosphorylation of H2A histone family, member X (H2AX) were examined. Results: Combined treatment with ALK-inhibitors plus 10 Gy-irradiation led to effects similar to those of sole radiotherapy, but was more effective than sole drug treatment. Conclusion: There is no clear evidence of sensitization to radiation by treating EML4-ALK mutated cells with ALK inhibitors.
Lung cancer is one of the leading causes of cancer deaths in the world (1). The translocation echinoderm microtubule-associated protein-like 4 (EML4)-anaplastic lymphoma kinase (ALK) is the predominant ALK-fusion in lung cancer and occurs in about 4 to 5% of NSCLC patients, which results in 40,000 new cases per year worldwide (2-4). There is an association of EML4-ALK NSCLC with young age, non- or light-smoking and adenocarcinomas (2, 5, 6).
The kinase domain of ALK is predominantly fused to the N-terminus of EML4 and leads to aberrant and constitutive activation of the ALK tyrosine kinase and the associated downstream signaling (7, 8).
ALK-rearranged lung cancer shows high sensitivity to ALK tyrosine kinase inhibitors (TKI), which suppress the growth of cancer cells and induce apoptosis (2, 9, 10).
Crizotinib, a first-generation ALK-TKI, was accredited in 2011 and is more effective than cytotoxic chemotherapy in advanced ALK-rearranged NSCLC (6, 11). Later, second-generation ALK-TKI such as Ceritinib and Alectinib were developed. They are highly active in advanced, crizotinib-refractory ALKpositive NSCLC (12, 13). In this context, Alectinib is the preferred first-line ALK-TKI (14). However, the development of different resistance mechanisms to several first- and second-generation ALK-TKI generates the need for continuous research (15). Moreover, new third-generation ALK-TKI such as Lorlatinib have been developed, which can be applied when disease progression occurs after treatment with first- or second-generation ALK-TKI (16).
Furthermore, radiotherapy is a standard therapeutic regime in the treatment of NSCLC (17). Crizotinib has been shown to act as a radiation sensitizer in EML4-ALK positive cells (10), and the combined treatment (Crizotinib plus radiotherapy) elicits beneficial effects in ALK-positive NSCLC lines (18).
The aim of our study was to examine whether there is a potential synergy between ALK inhibitors and radiotherapy in NSCLC cells, which may support the hypothesis of inducing radiosensitization by using ALK inhibitors. Two cell lines expressing wild-type (WT) or EML4-ALK were treated with ALK inhibitors followed by irradiation. Three ALK-TKI (Crizotinib, Ceritinib and Alectinib), which are all accredited by the US Food and Drug Administration (FDA) (6) were used. Cell survival, cell death and cell cycle distribution were analyzed as well as the presence of double-strand breaks after treatment.
Materials and Methods
Cell lines. Two human NSCLC cell lines - “ATCC-CCL-185 IG”, with EML4-ALK rearrangement and “ATCC-CLL-185 negative”, without any mutation (both obtained from LGC Standards; Wesel, Germany) - were cultivated in F12K medium (Life Technologies, Darmstadt, Germany), supplemented with 10% heat-inactivated fetal calf serum (Sigma-Aldrich Chemie GmbH, Taufkirchen, Germany) and 20 μg/ml Gentamicin (Biozym, Hessisch Oldendorf, Germany). Experiments were performed in 6-well-plates and cells were plated at a density of about 150,000 cells per well. Cells were harvested using trypsin 24 h after seeding and counted by using CASY system.
ALK-inhibitors and irradiation. Both cell lines were treated with Crizotinib/PF-2341066 (stock concentration 10 mM), Ceritinib/LDK378 (stock concentration 10 mM) or Alectinib/CH5424802 (stock concentration 5 mM), all obtained from Abmole via HÖLZEL Diagnostika (Cologne, Germany).
Dimethylsulfoxide (DMSO; from Sigma-Aldrich Chemie GmbH) was used to dissolve the drugs that were stored at −80°C and further as control treatment.
Irradiation was performed at 6 or 10 Gy (generated by a General Electric Isovolt 160 with a dose rate of 4 Gy/min) at the Department of Radiotherapy.
WST-1-assay. Water soluble tetrazolium (WST-1, from Sigma-Aldrich Chemie GmbH) was used to determine viable cells. Wells were filled with 150 μl F12K medium containing 2,500 mutant or WT cells and incubated for 4 h. All experiments were carried out in duplicates. Then, 15 μl diluted ALK-inhibitors (concentration 1 μM) or 15 μl DMSO (diluted 1:500, Sigma-Aldrich Chemie GmbH) were added to the wells. After 20 h the plates were irradiated with 0, 6 or 10 Gy. On that day and the following three days, WST-1-assays were performed adding 15 μl of WST-1-substance and incubating for another 4 h. Absorbance was measured at a wavelength of 450 nm with a Wallac Victor 2 plate reader operated by Wallac 1420 Manager Software.
Cell death. Tissue culture flasks were filled with 250,000 cells in F12K medium. After 4 h ALK-inhibitors or DMSO was added. After 20 h the cells were irradiated with 10 Gy, the next day harvested with trypsin and subsequently counted by using CASY system. Then, double stained for Annexin V using an Annexin V-Kit (eBioscience, San Diego, CA, USA) and propidium iodide (Genaxxon Bioscience, Ulm, Germany). Annexin V staining indicates early apoptotic cells, while additional staining by propidium iodide indicates necrosis.
Cells were identified and counted using BD FACS CANTO II Flow cytometer operated with BD FACS Diva Software. The flow cytometry analyses were illustrated with FlowJo Version 10 software with gating on singlet events.
Cell cycle. The cells were treated with the drugs, then irradiated, harvested with trypsin and counted by using CASY system as described for cell viability above. After the cells were washed with phosphate buffered saline (PBS, Biozym, Hessisch Oldendorf, Germany), cold ethanol (70%) was added and the tubes were put on ice for 30 min. Then, they were washed twice with 1 ml cold PBS, and 50 μl RNase (Qiagen, Hilden, Germany) and 200 μl propidium iodide (Genaxxon Bioscience) were added. The DNA content of the cells was inferred by the amount of propidium iodide binding. It was quantified with BD FACS CANTO II Flow cytometer operated with BD FACS Diva Software. The flow cytometry analyses were illustrated with FlowJo Version 10 software with gating on singlet events.
H2AX. Triggered by double stranded DNA damage, H2A Histone Family, Member X (H2AX) is phosphorylated during DNA repair, which can be visualized by immunofluorescence (19, 20).
The cells were treated with the drugs, then irradiated, harvested with trypsin and counted by using CASY system as described in cell viability above. Fixation solution (Merck Millipore, Darmstadt, Germany) was added and the cells were incubated on ice for 20 min. Afterwards they were washed twice with cold PBS and then Permeabilization solution (Merck Millipore) was added. The cells were split, 3.5 μl anti-phospho-H2AX FITC (Merck Millipore) were added to one half and 3.5 μl normal mouse IgG FITC (Merck Millipore) were added to the other half. The cells were left on ice for 20 min, washed with wash solution (Merck Millipore) and 150 μl PBS was added. The cells were identified and measured using BD FACS CANTO II Flow cytometer operated with BD FACS Diva Software. The flow cytometry analyses were illustrated with FlowJo Version 10 software with gating on singlet events.
Results
EML4-ALK mutated cells were more sensitive to Crizotinib than to Ceritinib and Alectinib. We determined the effects of monotherapy by different ALK-inhibitors on the cell lines CCL-185 IG (mutated) and ATCC CLL-185 negative (WT).
Both cell lines were treated with different concentrations of ALK-inhibitors (Alectinib, Crizotinib and Ceritinib) starting with 0.01 μM up to 3 μM. The mutant cell line was more sensitive than the WT cell line when treated with higher concentrations of Crizotinib (Figure 1C). In detail, there was a slightly higher sensitivity of the mutant cell line at the concentrations of 0.3 μM, 1 μM and 3 μM of Crizotinib compared to the WT line. Ceritinib and Alectinib had no noteworthy effect on both cell lines at concentrations between 0.01 μM and 1 μM compared to vehicle (Figure 1A and B).
For the following experiments we used a drug concentration of 1 μM (for all ALK-inhibitors) based on the plasma concentrations obtained by clinically used doses (12, 21-28).
Alectinib plus radiotherapy led to most cytotoxicity, while Ceritinib plus radiotherapy showed the best synergistic effect. Cell viability of both cell lines treated with ALK-inhibitors with or without subsequent irradiation was quantified by the WST1-assay.
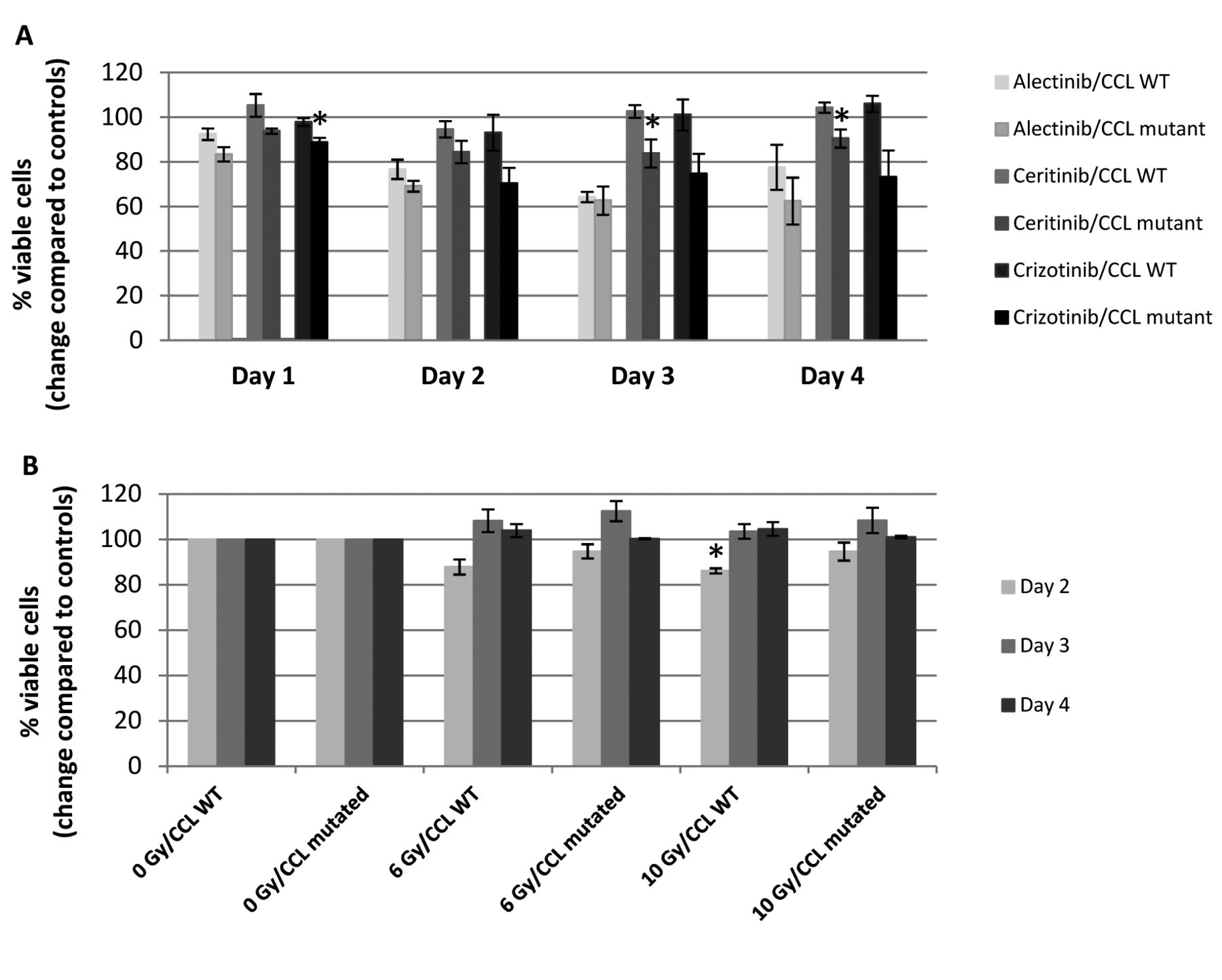
Figure 2A shows that the mutant cell line was more sensitive to the three drugs than the WT cell line when treated with ALK-TKI only. Crizotinib and Ceritinib induced selectively more cytotoxicity in the mutant than in the WT cells. On day 3 after Ceritinib treatment the percentage of viable mutant cells was reduced by 16% and at day 4 by 9% (both results significant (p<0.05), while the values of the viable WT cells were almost equal compared to vehicle at these days (Figure 2A). Alectinib induced more cytotoxicity in both cell lines than Crizotinib or Ceritinib and showed less selectivity between mutated and non-mutated cells on day 2 and 3.

Concentration dependent effect of different ALK-Inhibitors. Cell survival response curve of inhibition of non-small cell lung cancer cell lines by different anaplastic lymphoma kinase (ALK)-inhibitors. Wild-type (CCL WT) and echinoderm microtubule-associated protein-like 4 (EML4)-ALK mutated (CCL mutated) cell lines were treated with increasing concentrations of (A) Alectinib, (B) Ceritinib and (C) Crizotinib. Two days after drug treatment viable cells were measured by using water soluble tetrazolium (WST-1)-assay. Data are presented as mean±SEM of 4 separate experiments performed in duplicate.
Following treatment with irradiation only, both cell lines showed the same sensitivity one day after irradiation (day 2), in the sense of detecting fewer viable cells than the following days (days 3 and 4), (Figure 2B). In contrast, on days 3 and 4 the cells grew more in the absence of irradiation (Figure 2B). In addition, the WT cells exhibited higher sensitivity to irradiation (6 Gy as well as 10 Gy) compared to the mutated cells on day 2.
In most cases treatment with drugs plus irradiation led to the lowest numbers of living cells on the 2nd day. The most effective cytotoxic combination was that of Alectinib plus irradiation. As shown in Figure 3A treatment with Alectinib followed by 10 Gy irradiation decreased the number of viable cells of the mutant cell line to 65% and that of the WT line to 72%. Particularly, treatment with Alectinib without irradiation led to 69% viable mutated cells and to 77% viable WT cells on day 2. Combined treatment with Ceritinib and 10 Gy-irradiation resulted in 78% viable mutated cells on the 2nd day versus 85% viable mutated cells on the 2nd day after sole treatment with Ceritinib (Figure 3A). Ceritinib therefore showed the best synergistic effect with radiotherapy in mutated cells.
Sole treatment with Crizotinib led to 70% viable mutated cells, whereas the combined treatment of Crizotinib plus 10 Gy-irradiation resulted in 77% viable mutated cells on the 2nd day, indicating that there was no effect when comparing the two treatments (Figure 3A).
However, the results of the combined treatment were relatively close to those of the drug treatment alone. Also, in comparison to irradiation alone, combined treatment (drugs + 10 Gy) of the mutated cell line resulted in a considerably higher decrease in the number of living cells than the WT line on day 2 (Figure 3B). However, compared to sole irradiation, treatment with Alectinib plus irradiation with 10 Gy led to a statistically significant reduction in the survival of the ALK positive cell line on the 2nd day (Figure 3B).
Drug treatment plus irradiation led to increased necrosis rates. In order to investigate whether treatment with ALK inhibitors -with and without irradiation-triggers apoptosis and/or necrosis, we performed a cell death experiment. The results showed that both cell lines reacted to sole irradiation with increased apoptosis and necrosis rates (Figure 4A and B). Sole drug treatment led to a slight increase in apoptosis and necrosis of both cell lines. Drug treatment in combination with irradiation led to increased apoptotic and necrotic rates of both cell lines compared to vehicle (Figure 4A and B). For instance treatment with Alectinib plus irradiation (10 Gy) resulted in doubling of the necrotic (3% to 7%) and apoptotic (10% to 20%) rates compared to the DMSO response of the WT cell line, while in the mutated cells Alectinib plus irradiation led to a doubling of apoptotic rate (5% to 9%) and to higher than triplication of the necrotic rate (7% to 25%), compared to the DMSO response (Figure 4A and B).
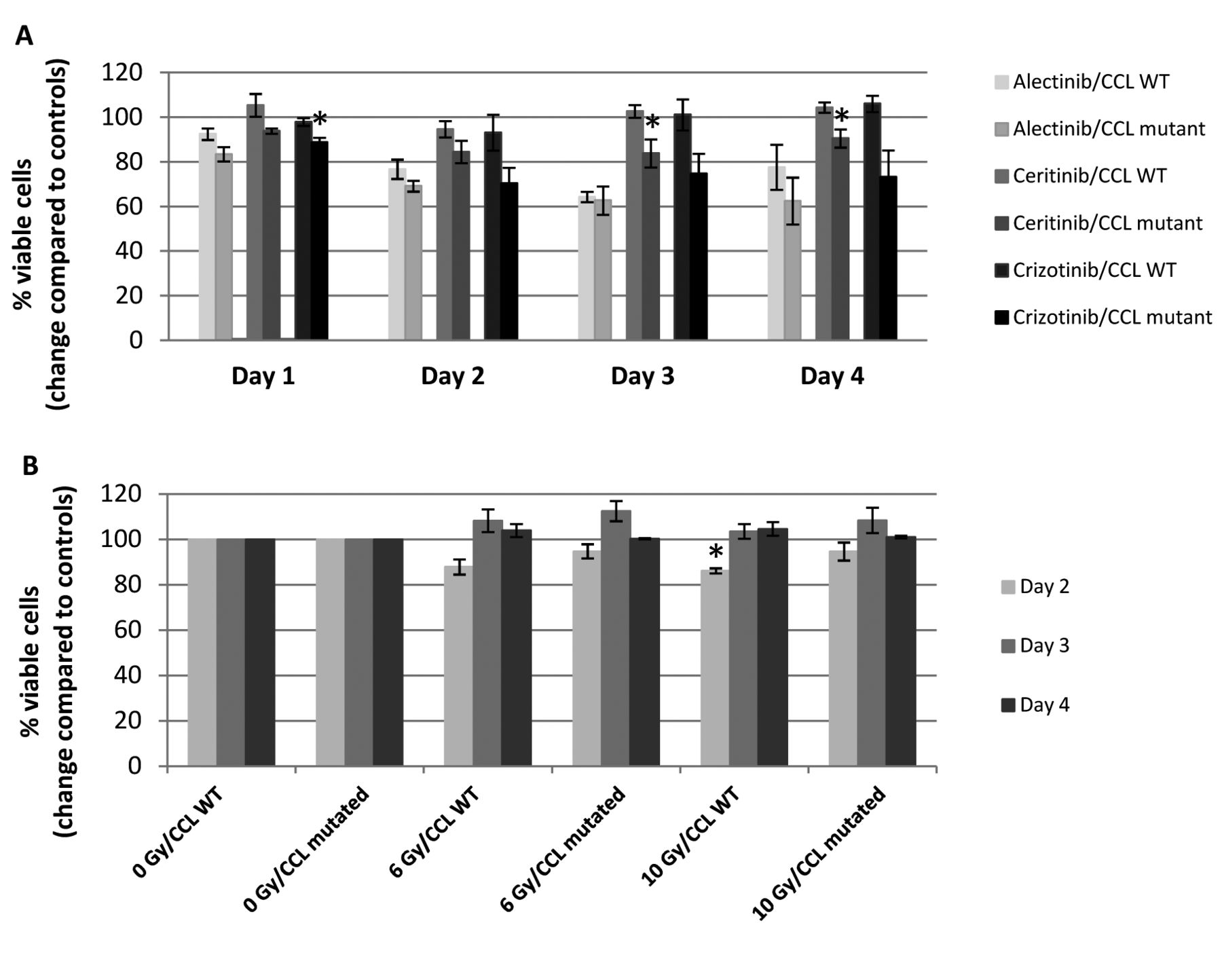
Time-dependent effects of (A) different ALK-Inhibitors and (B) different irradiation doses. Time course of inhibition of lung carcinoma cell lines with (CCL mutated) and without anaplastic lymphoma kinase (ALK)-mutation (CCL WT) by (A) treatment with different ALK-inhibitors and (B) irradiation with 6 Gy and 10 Gy compared to no irradiation. Cell survival responses were assessed by performing water soluble tetrazolium (WST-1)-assay at the indicated time points. Data are presented as mean±SEM of 3 separate experiments performed in duplicate. An unpaired t-test was conducted to examine the effect of (A) drug or (B) irradiation on cell survival. Asterisks indicate statistical significance (p<0.05) of (A) the results of the mutated line compared to the wild-type (WT) line (treated with the same drug and measured on the same time) and of (B) 10 Gy-irradiation compared to no irradiation (same cell line, same indicated time of measurement).
In the mutant cell line combined treatment had no effect on the apoptotic cell death compared to sole radiotherapy or monotherapy with ALK-inhibitors. However necrotic cell death was increased in the mutant cell line by combined treatment compared to sole drug treatment (significant), but had no significant effect compared to sole irradiation (Figure 4B). Combined treatment of the WT cell line showed that apoptotic rates as well as necrotic rates did not differ significantly from those with sole drug treatment or sole irradiation (Figure 4A).
Irradiation increased G2 cell-cycle arrest, while ALK-inhibitors had no significant effects on the cell-cycle. Cell cycle analysis provides information regarding the distribution of the cells in the various phases (G1, S or G2). The aim was to investigate which changes result from treatment with ALK inhibitors and radiation alone or their combination. Sole Irradiation led to increased number of cells in the G2 -cell-cycle phase in both cell lines, and simultaneously, to decreased numbers of cells in the G1- und S- phases. In detail, the percentage of cells in the G2-phase increased from 18% before irradiation (initial percentage of both cell lines) to 41% (WT) or 40% (EML4-ALK) after irradiation (Figure 5A and B). Treatment with ALK-inhibitors only was not significantly different in comparison to treatment with vehicle in both cell lines (Figure 5A and B). Compared to sole drug treatment, the combined treatment led to higher numbers of cells in the G2-phase in both cell lines. Treatment with drugs plus irradiation compared to sole irradiation had no significant effects on the G2-phase. However, treatment of the mutated cell line with Alectinib plus irradiation showed similar G2-cell-cycle arrest compared to sole radiotherapy, while treatment with Ceritinib or Crizotinib plus irradiation led to less G2-cell-cycle arrest compared to sole radiotherapy (Figure 5A and B).
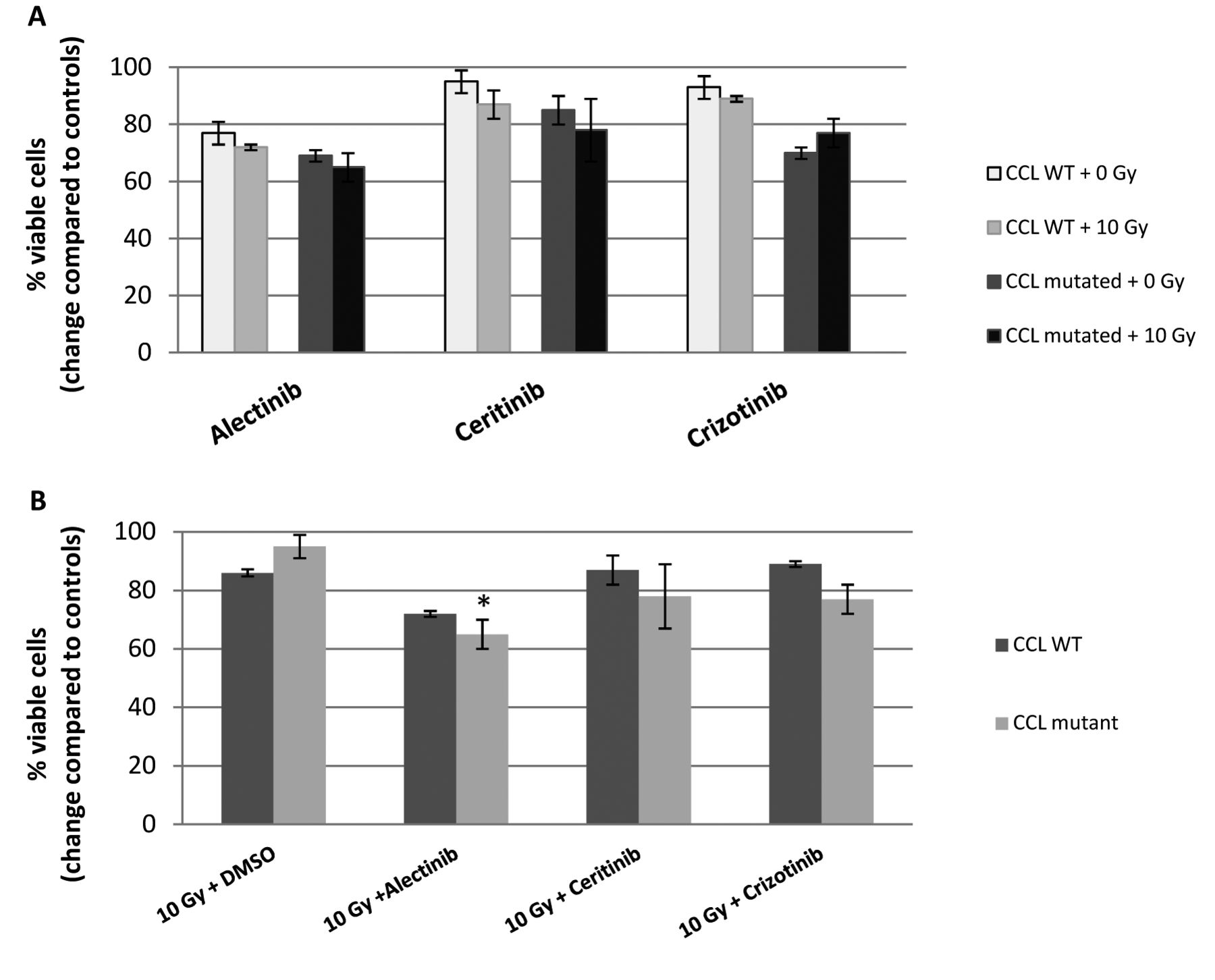
Treatment with ALK-inhibitors plus irradiation - results of day 2 (A) Effect of combined treatment with different anaplastic lymphoma kinase-inhibitors (Alectinib, Ceritinib, Crizotinib), followed by irradiation of the mutated cell line (CCL mutated) and the wild-type cell line (CCL WT). [Exemplary data for irradiation with 10 Gy compared to 0 Gy and cell viability measured using water soluble tetrazolium (WST-1) 2 days after drug treatment.] (B) Comparison of treatment with vehicle (DMSO) followed by irradiation versus combined treatment with different anaplastic lymphoma kinase-inhibitors (Alectinib, Ceritinib, Crizotinib) followed by irradiation of the mutated cell line (CCL mutated) and the wild-type cell line (CCL WT) [Exemplary data for irradiation with 10 Gy and cell viability measured using water soluble tetrazolium (WST-1) 2 days after drug treatment.] Data are presented as mean±SEM of 3 separate experiments performed in duplicate. An unpaired t test was conducted to examine the effect of drug treatment and irradiation on cell survival. There was no statistically significant (p<0.05) differences of the effects of 10 Gy-irradiation compared to no irradiation (A). Asterisks indicate statistically significant (p<0.05) differences between (B) the results of treatment with ALK-inhibitors followed by irradiation and those of treatment with vehicle (DMSO) followed by irradiation.
Irradiation led to double strand breaks. In order to determine whether irradiation (and ALK-inhibitors) led to double strand breaks, we investigated the cell response by examining the phosphorylation of H2AX.
There was an obvious increase of phosphorylated H2AX after irradiation, while both cell lines reacted similarly as measured by median fluorescence intensity. However combined treatment led to similar results for both cell lines than sole irradiation (Table I).
Discussion
The results showed that the mutant cell line was more sensitive than the WT cell line when treated with higher concentrations of Crizotinib. However, sole treatment with different concentrations of Ceritinib or Alectinib did not alter the percentage of living cells in both cell lines.

Cell death. Cell death following treatment with different anaplastic lymphoma kinase -inhibitors (Alectinib, Ceritinib, Crizotinib) or vehicle (DMSO) followed by irradiation (0 Gy or 10 Gy) of (A) the wild-type and (B) mutated non-small cell lung cancer cell line was measured by flow cytometry. Early apoptosis indicated by Annexin+ /propidium iodide-singlet events (light grey) and necrosis indicated by propidium iodide+ singlet events (dark grey) are illustrated as percentages of the total cell population. Data are presented as mean ±SEM of 3 separate experiments. A one-way ANOVA was conducted to examine the effect of drug treatment and irradiation on cell death. Asterisks indicate statistically significant (p<0.05) differences between the combined treatment (drug + 10 Gy) and drug treatment only (same cell line), or of the sole irradiation (DMSO + 10 Gy) and control (DMSO+0 Gy), all referring to necrosis.
H2A Histone family member X (H2AX) measurements.

Cell-cycle analyses. Cell-cycle analyses after treatment with different anaplastic lymphoma kinase -inhibitors (Alectinib, Ceritinib, Crizotinib) or vehicle (DMSO) followed by irradiation (0 Gy or 10 Gy) of (A) the wild-type and (B) the mutant non-small cell lung cancer cell line. Data are presented as mean ±SEM of 4 separate experiments. An unpaired t-test was conducted to examine the effect of drug treatment and irradiation on the distribution of cells in the cell cycle. Asterisks indicate statistically significant (p<0.05) differences between the combined treatment (drug + irradiation) and the sole drug treatment (same cell line) or of the sole irradiation (DMSO + 10Gy) and the control (DMSO+0Gy), all referring to G2-phase.
In the experiment of cell viability, Crizotinib and Ceritinib induced selectively more cytotoxicity in the mutant than in the WT cells. Alectinib showed less selectivity between the mutated and non-mutated cells but induced more cytotoxicity in both cell lines than the other drugs. Sole irradiation led to fewer live mutated and WT cells on the following day. The most effective combination in inducing cytotoxicity was Alectinib plus irradiation, whereas Ceritinib had the best synergistic effect with radiotherapy.
Drug treatment in combination with irradiation led to increased necrotic rates at least in the mutated cell line, while apoptotic rates did not differ or were even slightly smaller compared to those of sole irradiation. Treatment of the mutated cell line with Alectinib plus irradiation showed a similar G2-cell-cycle arrest, while treatment with Ceritinib or Crizotinib plus irradiation led to less G2-cell-cycle arrest compared to sole radiotherapy. ALK-inhibitors did not show any effect on cell-cycle. Irradiation led to double strand breaks in the mutated as well as in the WT cells, while no effect was observed when cells were treated with ALK-inhibitors only.
In conclusion, there was no clear evidence of sensitization to radiation of the EML4-ALK mutated cell line. The results showed that sole radiotherapy and the combined treatment with ALK-inhibitors plus 10 Gy-irradiation led to similar, not significantly different effects. None of the experiments we performed showed radiosensitization by using ALK-inhibitors in EML4-ALK mutated cells. However, nearly all of our experiments showed that the combined treatment was more effective than sole drug treatment in the mutated cells. Moreover, it should not be neglected that the WT cells often responded to the combined treatment in a way similar to that of the mutated cells.
A previous in vitro study has demonstrated that Crizotinib inhibits the growth of cells harboring EML4-ALK in a dose-dependent manner and, together with additional radiotherapy induced also apoptosis in these cells (10). In addition it was reported that Crizotinib combined with irradiation decreases cell proliferation of EML4-ALK positive cells more than sole radiotherapy and causes a doubling of apoptosis compared to sole Crizotinib treatment (18).
Moreover, both studies explored whether Crizotinib sensitizes EML4-ALK mutated cells to radiation (10, 18). Compared to our findings, the inhibition of the growth of mutated cells by Crizotinib was not as prominent, but induced apoptosis in combination with radiotherapy. However, combined treatment (Crizotinib followed by radiotherapy) led to an increase in the growth of the mutated cells and finally there was no evidence of radiosensitization. The differences in results between the different studies can be due to variations in the assays, the number of repetitions of the experiments, as well as the characteristics of the human cancer cells.
Furthermore, the higher sensitivity of the cells to treatment with Alectinib may be the underlying mechanism of the longer progression-free survival observed in the Global Phase III ALEX Study of Alectinib compared to Crizotinib (29, 30).
Several clinical trials have investigated the use of the second-generation ALK-inhibitors Ceritinib or Alectinib following a failure of the desired clinical response by treatment with the other (due to acquired resistance) in order to improve clinical outcome (31, 32). In this context it would be interesting to discover whether combined radiotherapy would lead to similar or even enhanced results and furthermore may delay the development of different resistance mechanisms.
Conclusion
In summary, there is no indication for radiation sensitization of the EML4-ALK mutated cells after treatment with the used ALK-inhibitors. Our results support the hypothesis that the combined treatment of EML4-ALK mutated NSCLC with ALK-inhibitors and irradiation will have a beneficial effect.
However, it should not be neglected, that there is a potentially damaging effect of this combined or sequential treatment of TKI and radiation, especially in the brain. Alectinib may accumulate in the brain (e.g. in contrast to Crizotinib), because it is not a substrat of efflux transporters like P-glycoprotein, has a high CNS tissue penetration and may lead to a brain injury as a possible consequence (13, 33, 34). In addition, we would like to emphasize that our findings, which were performed in vitro, are not directly transferable in vivo.
Acknowledgements
This work was supported by Novartis Pharma GmbH (Nuremberg, Germany). The Authors thank Waltraud Fröhlich for excellent technical support and Luitpold Distel for use of the radiation chamber. Kathrin Fleschutz performed the present work in fulfillment of the requirements of the Friedrich-Alexander-University Erlangen-Nuremberg (FAU) for obtaining the degree “Dr. med.”.
Footnotes
Authors' Contributions
Lucie Heinzerling, Lisa Walter and Kathrin Fleschutz conceived the project and designed the experiments. Kathrin Fleschutz and Lisa Walter executed the experiments an analyzed the data. All Authors wrote and approved the manuscript.
Conflicts of Interest
The Authors Kathrin Fleschutz, Lisa Walter and Rumo Leistner do not have any conflicts of interest in relation to this study.
Lucie Heinzerling indicates conflict of interests in relation to fees for consultancy activities she received from Novartis, Roche, BMS, MSD, Curevac and Amgen.
This work was supported by Novartis Pharma GmbH (Nuremberg, Germany). Novartis Pharma GmbH had no involvement in study design, the collection, analysis and interpretation of data, in the writing of the report and in the decision to submit the article for publication.
- Received June 24, 2020.
- Revision received July 20, 2020.
- Accepted July 21, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.