


Abstract
Background/Aim: Melanoma tumor cell sub-populations expressing a variety of specific molecular markers have been identified. We hypothesized that expression of CD114, the cell surface receptor for granulocyte-colony stimulating factor (G-CSF), would be associated with melanoma tumor cell growth and response to treatment. Materials and Methods: We determined the expression of CD114 expression in tumor cell lines by flow cytometry. We separated melanoma tumor cells into CD114-positive and - negative populations by fluorescence-activated cell sorting (FACS) and measured cell growth and responses to temozolomide and etoposide and the anticancer agent nifurtimox. Results: All tested cell lines demonstrated a sub-population of cells with CD114 surface expression. CD114-positive sub-populations grew faster than CD114-negative ones and demonstrated resistance to temozolomide, etoposide, and nifurtimox. Conclusion: CD114 expression defines a sub-population of melanoma tumor cells with altered growth and resistance to treatment. Further studies on the role of CD114 in melanoma pathogenesis are warranted.
Melanoma is a neural crest-derived malignancy that is increasing in frequency in the United States, with more than 70,000 new cases diagnosed each year. The incidence of melanoma has been increasing by almost 3% per year (1), leading to an increased awareness of the morbidity and mortality of the disease. However, the diagnosis of melanoma is unfortunately often delayed, leading to increased chances of tumor invasion, disease spread, and poor outcomes.
Current treatment for melanoma includes surgical tumor removal and chemo- and immunotherapy for patients with metastatic and recurrent disease (2, 3). Approximately 50% of melanoma tumors have mutations in the BRAF gene or in genes of other members of the RAS/MAPK signaling pathway (4). Treatment with specific BRAF inhibitors has resulted in increased progression-free survival times for patients with tumors with BRAF mutations (5), but single-agent therapy has not resulted in cure for most patients. Furthermore, even with the addition of these biologically targeted-therapies, melanoma tumors that have spread to distant sites are rarely curable.
Recent studies have identified sub-populations of melanoma cells that demonstrate treatment resistance, and the frequency of these sub-populations correlates with more aggressive disease and poor prognosis (6), suggesting that therapies directed against these melanoma sub-populations are likely to improve patient outcomes. These treatment-resistant populations have been hypothesized to persist in tumors and contribute to disease relapse (7).
A recent study by Hsu and colleagues identified a sub-population of neuroblastoma tumor cells defined by surface expression of CD114 that demonstrates enhanced tumorigenicity and the ability to self-renew (8). However, the relevance and significance of CD114 expression in other neural crest-derived tumors is unknown. We hypothesized that melanoma tumor cells would demonstrate a CD114-positive subpopulation and that CD114 expression would be associated with enhanced tumor cell growth and responses to treatment.
Materials and Methods
Cells and culture conditions. The cell lines used in this study were purchased from American Type Culture Collection (ATCC, www.atcc.org; A375, SK-MEL-28, U87, U373, Daoy, CHLA-02-ATRT, and PFSK-1 cell lines) or were generously provided by Susan Cohn (The University of Chicago Children's Hospital, Chicago, IL; SK-N-SH, SK-N-AS, SH-SY5Y, SH-EP, IMR-32, and SK-N-MC cell lines), John Maris (Children's Hospital of Philadelphia, Philadelphia, PA; CHP-212 and CHP-134 cell lines), Jill Lahti (St. Jude Children's Research Hospital, Memphis, TN; SJ-NB-10 cell line), and Daniel Albert (University of Wisconsin-Madison, Madison, WI; Weri and Y79 cell lines). Cell lines were cultured as previously described (9) or by following the ATCC instructions. All cell lines were authenticated by DNA profiling prior to use.
Therapeutic agents. Nifurtimox was generously provided by MetronomX, Inc. (Houston, TX, USA). A 20 mg/mL stock solution was generated in dimethyl sulfoxide (DMSO) (Sigma-Aldrich, St. Louis, MO, USA) and stored at −20°C. Nifurtimox was diluted in phosphate-bufferred saline (PBS) immediately before use. Temozolomide and etoposide were purchased from R&D Systems (Minneapolis, MN, USA), and were diluted directly in media prior to use.
Flow cytometry assays. Flow cytometry was conducted on an LSR II 5-laser flow cytometer (BD Biosciences, San Jose, CA, USA). Antibodies used included phycoerythrin (PE)-conjugated anti-CD114, allophycocyanin (APC)-conjugated anti-CD114 (BD Biosciences), and APC-conjugated anti-CD133 (Miltenyi Biotech Inc., Auburn, CA, USA). Reactivity to mouse and human Fcγ receptors was blocked by 15-min pre-incubation with mouse Fc-block (1:1, 000; BD Biosciences) and polyclonal human IgG (2 mg/ml; Sigma-Aldrich, St. Louis, MO, USA), respectively. Dead cells were excluded by staining with 4’,6-diamidino-2-phenylindole (DAPI) for 5 min before analysis (Invitrogen Corp., Carlsbad, CA, USA). Fluorochrome- and isotype-matching monoclonal antibodies were used as negative controls. Fluorescence-activated cell sorting (FACS) was conducted on a DAKO Cytomation MoFlo 9-color cell sorter (Beckman Coulter, Brea, CA, USA). BD FACSDiva v6.1.2 (BD Biosciences) was used to analyze flow data and Summit v4.3 (Cytomation; Becton Dickinson, New York, NY, USA) software was used to analyze FACS data.
Cell viability assays. The viability of cells was determined using a modified methyl tetrazolium (MTT; Sigma) assay as previously described (9). CD114-positive and -negative cells were isolated by FACS and 500 cells/well were plated in 96-well plates. 24 h later, temozolomide, etoposide, or nifurtimox was added to each well. After 72 h of continuous drug exposure, MTT assays were performed. Replicates of three wells were used for each drug concentration and assays were repeated on separate days.
Crystal violet staining. Parental melanoma cell lines and CD114-positive and -negative cells isolated by FACS were plated at 103 cells/well in 6-well plates in standard culture medium. After four or seven days of growth, cells were fixed in 4% paraformaldehyde for 20 min and stained with 1% crystal violet (Sigma) for 30 min. Excess stain was washed off with water and photographs taken with a Photometrics Coolsnap microscope camera using RS-Image Version 1.9.2 (Proper Scientific Inc.; Tuscon, AZ, USA) software attached to a Nikon Eclipse TE300 Inverted Fluorescent Microscope (Nikon American, Inc.; Melville, NY, USA).
Results
CD114 expression in tumor cell lines. CD114 surface expression has been identified in subpopulations of neuroblastoma tumor cell lines (8), however, the presence of CD114-positive sub-populations in cell lines from other tumor types is not known. We screened a panel of tumor cell lines by flow cytometry and identified a sub-population of CD114-positive tumor cells in each tested cell line, including the melanoma tumor cell lines A375 and SK-MEL-28 (Table I). Previous reports have identified a sub-population of melanoma tumor cells characterized by CD133 expression that demonstrated treatment resistance (10). We, therefore, sought to determine if CD114 was found to be co-expressed within the CD133-positive sub-population. Analyses of melanoma cell lines by flow cytometry demonstrated that CD114 and CD133 were both expressed in sub-populations of melanoma cells, but that there were no identifiable populations that expressed both markers simultaneously (Table I).
CD114-positive cells in tumor cell lines. A panel of tumor cell lines were screened by flow cytometry for CD114 expression (top). The percentage of cells positive for CD114 are shown for each cell line. Melanoma cell lines were then screened by flow cytometry for CD133 and CD114 expression (bottom). The percentage of cells positive for CD114 alone, CD133 alone, and both CD133 and CD114 are shown for each cell line.
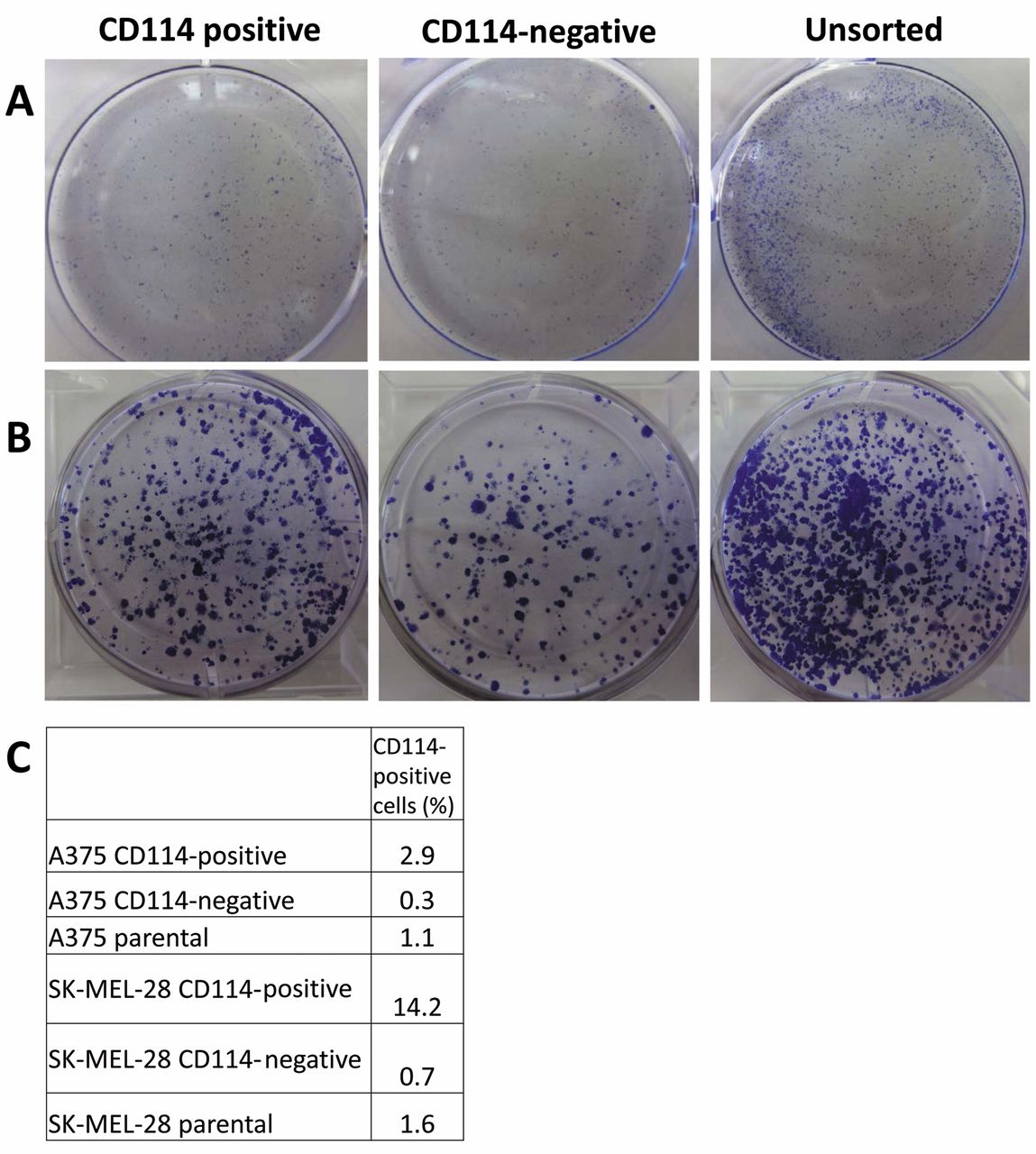
CD114-positive cells demonstrate more rapid growth compared to CD114-negative cells. To determine the association of C114 expression with tumor cell proliferation, melanoma cell lines were sorted by FACS into CD114-positive and -negative populations and allowed to proliferate separately in culture. Crystal violet staining of viable cells demonstrated that the CD114-positive sub-population proliferated more rapidly than the CD114-negative one, although the parental mixed cell line proliferated more rapidly than either separate sub-population alone (Figure 1), suggesting that interactions between the sub-populations may induce more rapid cell growth.

Melanoma cell line growth after sorting into CD114-positive and -negative sub-populations. A375 melanoma cells were sorted into CD114-positive and CD114-negative sub-populations and 103 cells of each sub-population and 103 mixed parental cells were plated and allowed to grow for 7 days. Cells were stained with crystal violet at 4 days (A) and 7 days (B). After 7 days, cell populations were then screened again for CD114 expression by flow cytometry. The percentage of cells positive for CD114 after 7 days are shown for each cell line (C).
In order to determine whether sorted sub-populations were able to maintain their CD114 expression pattern, melanoma tumor cell CD114-positive and -negative sub-populations were analyzed by flow cytometry for CD114 expression after seven days in culture. The percentage of CD114-positive cells in the sorted CD114-positive sub-population decreased significantly and approached the percentage in the unsorted parental population, while the CD114-negative sub-population acquired a small percentage of CD114-positive cells (Figure 1), suggesting interconversion of CD114-positive and -negative tumor cell sub-populations, as previously observed (8).

Cell viability of CD114-positive, CD114-negative, and parental cell lines after anticancer therapy. A375 (left) and SK-MEL-28 (right) melanoma cell lines were sorted into CD114-positive and CD114-negative sub-populations and exposed to temozolomide (top) and etoposide (middle) and the anticancer agent nifurtimox (bottom) at different concentrations. Cell viability was measured after 72 h of drug exposure.
CD114-positive cells demonstrate resistance to treatment. To evaluate the relative responses of CD114-positive and -negative sub-populations to treatment, melanoma tumor cell lines were sorted into CD114-positive and -negative sub-populations and exposed to chemotherapy agents etoposide and temozolomide and the anticancer agent nifurtimox (11-13). In each case, the CD114-positive sub-population demonstrated increased cell viability after treatment, while the responses of the CD114-negative sub-population mirrored the responses of the parental mixed tumor cell lines (Figure 2), suggesting that CD114 expression is a marker for a chemoresistant sub-population in melanoma cell lines.
Discussion
Melanoma is a neural crest-derived malignancy that is increasing in frequency and, despite aggressive treatment strategies, melanoma tumors that have spread to distant sites are rarely curable. We have demonstrated that expression of the cell surface marker CD114 is limited to a sub-population of melanoma tumor cells that demonstrate altered growth and resistance to treatment, suggesting that CD114 expression may be a marker to identify melanoma tumor cells that contribute to disease relapse and poor patient outcomes.
CD114, which serves as the cell surface receptor for G-CSF, promotes neurogenesis and is expressed on neuronal and neural crest-derived cells (14, 15). In addition, signaling through CD114 promotes the survival and proliferation of neural stem cells (15), and may promote neural tissue regeneration after injury (16). CD114 expression is also implicated in the pathogenesis of multiple tumor types including ovarian, bladder, and squamous cell cancer (17-19), but the role of CD114 in melanoma, however, is unknown.
Hsu and colleagues demonstrated the presence of CD114-positive tumor cells in primary neuroblastoma tumor samples (8); our findings also need to be confirmed in tumor specimens from patients with melanoma. Our data on melanoma tumor cell lines suggest that CD114 may serve as a marker for a treatment-resistant cancer stem cell-like sub-population in melanoma as well as other tumor types that warrants further investigation.
Our results have demonstrated that CD114-positive melanoma tumor cells demonstrate altered growth and treatment resistance. The functional consequences of CD114 expression in melanoma tumor cells, however, are unknown. G-CSF treatment of neuroblastoma tumor cells leads to an increased percentage of CD114-positive cells, which can be blocked with STAT3 inhibition (8). STAT3 is a transcription factor activated in response to numerous signaling pathways, including G-CSF-mediated activation of CD114, and STAT3 has been implicated in melanoma metastasis and immune evasion (20, 21). We are currently investigating the efficacy of STAT3 inhibition in melanoma cells, and our data also suggest that specific targeting of the G-CSF-mediated activation of CD114 may also be effective against melanoma tumors.
We have demonstrated that expression of the cell surface marker CD114 defines a sub-population of melanoma tumor cells with altered growth and resistance to treatment. Our data also suggest a potential functional role for CD114 expression in melanoma tumor cell growth and responses to therapy, and further studies of the role of CD114 in melanoma tumors are warranted.
Footnotes
Conflicts of Interest
All Authors declare that they have no conflicts of interest with regard to this study.
- Received April 15, 2015.
- Revision received May 9, 2015.
- Accepted May 11, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.