


Abstract
Prophylactic vaccination is arguably the most effective medical preventative method. After local inoculation, vaccines induce antigen-specific systemic immunity, protecting the whole body. Systemic antitumour immunity can cure advanced cancer, but will therapeutic vaccination suffice? A vaccine for castration-refractory prostate cancer (CRPC) was approved by regulatory authority, but its evidence is disputed. We critically reviewed the clinical efficacy of therapeutic cancer vaccines for prostate cancer, including the results of 31 clinical studies employing vaccines-only, and another 10 studies combining vaccines with immune co-stimulation. Vaccinations yielded immunological responses, but no study showed evidence for clinically relevant therapeutic improvement. Clinical failure of therapeutic vaccination is discussed in the light of immunological dogmas and mechanisms of antitumour therapies. We propose that cancer immunotherapy might be improved by immunological danger, i.e. disturbing tumour homeostasis by destroying the tumour tissue or inducing local inflammation. Such danger might override immunological tolerance, and thereby allow clinically relevant anticancer results.
Curative treatment options for advanced cancer, e.g. disseminated disease, are very limited. Chemotherapy may prevent and reduce formation of metastases, but it rarely cures patients from advanced metastasized disease. In contrast, the immune system could mount antigen-specific responses against such cancerous lesions. Spontaneous tumour regression in patients with heavy infections has been documented for about a century (1). In the 1950s, the validity of the antitumour immunity concept was shown in animal experiments (2). In the 18th century, vaccines (i.e. weakened antigens) were already being used for efficient clinical protection. Therefore, it seemed logical to search for a vaccine against cancer. A decade ago, experts in the field concluded that half a century of antitumour vaccine research had not yielded any major clinical breakthroughs (3).
Classical vaccine technology holds the golden rule that vaccines should be applied in the prophylactic setting, i.e. prior inoculation with the pathogen. This is why children, but not diseased people, are vaccinated against bacterial and viral pathogens to prevent the development of disease. Prophylactic vaccination also yields good protection against infection with tumourigenic viruses (4-6). Therapeutic vaccination is a different chapter in immunology from prophylactic vaccination. Indeed, microbiologists have often tried therapeutic vaccination, but generally with little if any clinical efficacy. This is in sharp contrast to prophylactic vaccination which has been shown to have invaluable clinical efficacy. In therapeutic settings, the battle against micro-organisms does not include vaccination. Clinicians chose interference with pathogen reproduction by treatment with antibiotics. Such a dual strategy resembles prophylactic vaccination against tumourigenic viruses on the one hand, and applying chemotherapy in tumour-bearing patients. In light of the described efficacy of immunotherapy and the limited efficacy of chemotherapy in advanced disease, therapeutic vaccination for treatment of cancer might be evaluated on its clinical efficacy, despite the apparent lack of efficacy against microbes.
Some commentators regard the approval of the first therapeutic cancer vaccine by the Food and Drug Administration (FDA) of the U.S.A. as clinical proof-of-concept for therapeutic vaccines. They have hailed this approval stating that immunotherapy has earned its spot in the ranks of cancer therapy (7). The studies with therapeutic vaccination using Sipuleucel-T in patients with castration-resistant prostate cancer (CRPC) showed statistically significant results (8, 9). However, the results did not match the criteria for clinically relevant improvement of anticancer therapy, e.g. at least six months prolonged survival compared to standard therapy (10, 11). Moreover, some serious concerns have been raised about the experimental design of these clinical studies. Patients in the control group were not subjected to standard treatment, but also received leukapheresis processing with 1.5-2 times the patient's blood volume. While patients in the Sipuleucel-T treatment group were reinfused with all their mononuclear cells, those in the ‘control’ group actually had a net removal of about 60% of their circulating mononuclear cells. Patients in the ‘control’ group had a decreased survival compared to literature, whereas the treatment group had ‘normal’ survival. Another unexpected finding was that elderly patients had an adverse prognosis in this study, in contrast to general expectations (12). In short, both the controversial study design and lack of clinically relevant results are a serious bloodletting to the evidence for clinical efficacy of therapeutic cancer vaccination.
The concept of therapeutic vaccination is not invalidated, however, by lack of evidence in a single study. Therapeutic vaccines have been extensively tested for CRPC using a dozen different approaches. From a tumour immunological viewpoint, CRPC is an ideal target since (i) prostate cancer is the most common cancer in men and the second most common cause of cancer-related death among men in Europe and North America (13, 14), (ii) no curative options exist for patients with advanced disease, i.e. disseminated CRPC (15-17), (iii) the overall survival is 28 to 36 months (18), implying sufficient time for effective immunological reactions to develop (iv) various prostate-specific antigens exist (19-22); and (v) the prostate it is not a vital organ, thus limiting the risk of life-threatening autoimmune complications. Keeping in mind, the massive clinical evidence of the efficacy of prophylactic vaccination, and the promises of cancer immunotherapy in general (23), therapeutic vaccination seems a reasonable approach for CRPC.
Forty-one clinical studies were performed that could have rejected the null hypothesis that there is no clinical-relevant effect of therapeutic vaccines. Most of these, 31/41, used therapeutic vaccines only, and 10 studies also used systemic injection of (antibodies against) co-stimulatory molecules (e.g. Cytotoxic T-Lymphocyte Antigen 4; CTLA4). We discuss these therapeutic results in light of cancer immunology, and anticancer therapies, including other immunotherapeutic approaches.
Therapeutic Vaccines Trigger Anticancer Immune Responses
The efficacy of prophylactic vaccination is often determined by measuring the increase in antigen-specific antibody or T-lymphocyte responses as a surrogate for immunological protection. Five studies measured antigen-specific immune responses by increasing levels of antibodies. The vast majority of treated patients, 85% (96 out of 113) had increased levels of tumour-associated antibodies (24-28). In three studies, cytotoxic T-lymphocytes and helper T-cells were counted, and vaccines stimulated antigen-specific T-cell proliferation in all 61 patients (24, 25, 27). This shows that these vaccines were technically effective in that they induced humoral and cellular immune responses in treated patients. No hard rules exist on immunological responses and clinical protection, but the immune responses are generally calibrated to their clinical efficacy. In prophylactic studies, immune protection is measured by pathogen challenge (i.e. in animal experiments) or the odds of developing disease after exposure to the pathogen. A major difference between prophylactic and therapeutic vaccination is that in the therapeutic setting no calibration of immune protection with surrogate immune parameters can be made. Thus the clinical efficacy must be measured directly, by monitoring disease regression and progression after vaccination.
Therapeutic Vaccination Yields No Clinically Relevant Anticancer Effects
Since patients with immunological response had a technically successful intervention, we focused on clinical responses in these patients. Only two out of 96 patients with antibody responses had a complete (CR) or a partial (PR) regression (Table I) (24-28). In addition, only one patient had a CR, and there were no PRs out of 61 patients with vaccine-stimulated antigen-specific T-cell proliferation (24, 25, 27). Although the vaccines were effective in inducing immune responses, they did not induce clinical responses. This therefore confirms earlier conclusions that antibody response and specific T-cell proliferation are not adequate predictors of clinical response to therapeutic vaccines (28, 29).
Clinically relevant parameters are the various measures of survival, i.e. disease-free, overall, and progression-free survival. Many studies also measure immune or biochemical parameters, but these are only important if they can be linked directly to survival of patients.
The Response Evaluation Criteria In Solid Tumours (RECIST) parameters also allow for measurement of tumour size (30). A surrogate parameter for the size of prostate carcinoma can be monitored by measuring Prostate-Specific Antigen (PSA) in serum. Prostate carcinomas shed PSA into the circulation, and a smaller tumour would shed less PSA than a larger one. Changes in PSA are interpreted in two ways, as PSA response and changes in doubling time (DT). Changes in PSA DT are not considered to be a measure of therapeutic efficacy, since the DT implies that PSA is still high and rising (31). It is important to stress that from a clinical point of view, patients with a decrease in PSA DT still have progressive disease (PD).
Immunological responses compared to clinical responses in studies using therapeutic vaccination.
A PSA response, i.e. a significant reduction of PSA value, could be indicative of a clinical response. The drawback is that measuring serum PSA is an indirect measure of the therapeutic effect. PSA levels can rise due to prostatitis and other diseases (32-34). Most relevantly successful immunotherapy of regional cancer, e.g. bladder carcinoma, can significantly increase the PSA levels (35), possibly as a bystander effect of local inflammation. In line with this, current criteria of the Prostate Cancer Working Group (PCWG2) strongly diminish the importance of PSA levels, in favour of measurement of the primary tumour and metastases (36). Considering the effect of tumour load and inflammation, the intended immunological rejection of prostate cancer could cause an increase or a decrease in PSA. The surrogacy of PSA end-points makes it unsuitable as the primary end-point in clinical trials in prostate cancer, especially in testing non-cytotoxic agents such as immunotherapy (37-39).
Clinical relevance of a therapeutic intervention should be evaluated in terms of a clear therapeutic benefit for the patients, and not as a change of a surrogate marker (10, 11). Ideally the benefit should be clinically prolonged survival, however this is not measured in most studies. Therefore, we focused on direct measurement of the therapeutic efficacy, e.g. in terms of CR, PR, stable disease (SD), and PD. Depending on the stage of CRPC, overall or disease-free survival could be monitored. A PSA test is a highly sensitive biochemical measurement for the presence of prostate cells in the body. In this light, progression-free survival might be considered if the included patients only had non-clinically manifest, biochemical disease (i.e. ‘PSA recurrence’) and progression was defined as the first detected metastasis; technically this would be referred to as clinical progression.
Table II summarizes data of 41 clinical studies employing therapeutic vaccination against prostate cancer performed in 2000-2012. These vaccination approaches have used the entire spectrum of modern vaccine technology, including different types of antigen (prostate cancer cells, protein, peptides, DNA, and carbohydrates), different modes of delivery [virus, DNA, and dendritic cells (DCs)], and different adjuvants of co-stimulation (biological response modifiers, cytokines such as Granulocyte-Macrophage Colony Stimulating Factor (GM-CSF) and Interleukin 2 (IL2); co-stimulatory molecules or inhibition of CTLA4). Considering the importance of responses in clinical phase I, II and III studies, it may be assumed that any response, whether complete or partial would be reported. However the state-of-the art vaccination technologies led to only one CR and three PRs out of 1,100 treated patients.
Traditionally, clinical effects against CRPC are not measured by remissions (CRs and PRs), but by determining PSA level. As stated before, this may not be the optimal method since effective immune responses might also induce a rise in PSA. Table III shows the PSA responses for all vaccines together, vaccines-plus-docetaxel, docetaxel-alone and mitoxantrone. The PSA responses for all vaccines were low, with an average of about 2%. Even the best result in a single study yielded less than 13%. This is much lower than studies employing chemotherapy. A small study of the combination of vaccine with docetaxel yielded 21%, and docetaxel alone 48%. Another chemotherapy intervention, mitoxantrone yielded 30% PSA responses.
Taken together both the remissions and the PSA responses do not indicate clinical efficacy of the therapeutic vaccines.
Evaluation of the Lack of Clinical Efficacy
As stated before, prophylactic vaccination against pathogens effectively prevents disease by inducing immunity. Other immunotherapeutic approaches have produced results that suggest that the immune system can also cure cancer and protect from recurrent disease. Why are these results not reflected in the outcomes of 1,100 patients with prostate cancer treated with therapeutic vaccination? Many differences existed within vaccination philosophies and protocols used, and it could be argued that only a few vaccination studies used an effective protocol, blurring the data in the aggregate of 41 studies. One could further reason that a putative effect of vaccination strategy in a small study of 10 to 50 patients would be too small to be seen. But do these arguments suffice for the lack of clinical efficacy that is found after vaccination?
Summarized therapeutic results from studies employing different vaccination strategies.
First of all, the PSA responses were much lower, even in the vaccine study most responsive effects compared to docetaxel treatment, e.g. 13% versus 48%, respectively. Thus vaccines seem to be ineffective in inducing PSA response. Alternatively, a single study might induce CR or PR in a substantial group of patients. Various other cancer immunotherapies have yielded such results that are statistically significant and clinically relevant in groups of 10 to 50 patients (40). In order to obtain a p-value <0.05, at least three patients in a study should have a CR or PR. Besides the possibility of being statistically significant, this would also be considered as clinically relevant. We previously discussed the induction of immune responses in 85% to 100% of the patients treated, which correlates nicely with data from prophylactic studies showing that 90 to 100% of the vaccinated people were protected. If three CR or PR responses were obtained in a study with ten to fifty patients, it would be a clinical response of 6 to 30%. Thus, if therapeutic vaccination were clinically effective, such a response should be more than feasible. Reviews of clinical immunotherapeutic studies for eight different forms of both locally advanced and metastasized cancer showed that these yielded on average 50% CRs and PRs. All 15 studies with six to 35 patients had at least three clinical responses in patients with immunotherapy (41). From all these data it is more than reasonable to assume that if similar results had been obtained in any of these 41 studies, these would have arisen at the analysis of PSA responses, or CRs and PRs. Nevertheless, such a result was not found in any of the vaccination studies. It is hard to solely attribute the failure of success to a sub-optimal vaccination strategy, since these studies employed many different vaccination strategies, all being the state-of-the art vaccine technology.
Comparing PSA responses (PSA-R) in studies employing different therapies against castration-resistant prostate cancer (CRPC)
Cancer immunotherapy is not a strategy without clinical results. Although therapeutic vaccination has failed to show clinical efficacy, other forms of cancer immunotherapy did show clinically relevant results (40, 41). Thus the question might be asked is therapeutic vaccination a putative curative therapy of cancer? And if not, how could cancer immunotherapy be improved?
Cutting a long story short, vaccines are most effective in preventing, but not curing, disease. The next question is, can we explain the inefficacy of therapeutic vaccines using immunological dogmas?
Tumour-bearing Patients Are Antigen-specific Tolerant
Patients that bear or bore tumours are not immunologically-naïve, but antigen-specific tolerant to the tumour. Immune tolerance is an active immunological process that involves various T-lymphocyte populations. Helper and cytotoxic T-lymphocytes can differentiate into a variety of effector and tolerogenic functions. Immunologists differentiate between type 1, type 2, type 17 (TH17), and a whole range of suppressor and regulatory T-lymphocytes. Tumour-infiltrating T-cells can become immune suppressive or tolerogenic (42). Regulatory T-lymphocytes were shown to be involved in immune tolerance to murine tumours, and were also demonstrated in various human tumours (43). Tumours induce various kinds of regulatory T-lymphocytes (44). In the blood of patients with prostate cancer, cluster of differentiation 4 (CD4+) T-cells co-expressing CD25high and forkhead box P3 (FOXP3+), e.g. regulatory T-lymphocytes, are increased in number and function (45-47). Locally in the tumour, different types of tolerogenic T-lymphocytes are involved, e.g. TH17 and classical TReg (47, 48). Other studies have pinpointed the involvement of CD8+ regulatory cells in prostate cancer by the markers Foxp3+ or programmed death 1 (PD-1+) (49, 50). The complex roles of different CD4+ and CD8+ T-lymphocytes were further confirmed (51, 52). In the most simplified model from a clinical perspective, two types of T-cells exist: immunogenic and tolerogenic lymphocytes. How does the presence of immunological tolerance affect the efficacy of therapeutic vaccination?
Therapeutic vaccination increases both effector T-lymphocytes and regulatory T-lymphocytes (53). Both types of antigen-specific T-lymphocytes respond to the tumour antigen they recognize and T-cell growth factors (e.g. cytokines such as IL2, and IL15). In the prophylactic setting, the immune system is naïve and has the plasticity to be easily instructed for immunogenic effectors. Any immunological adjuvants will steer the T-lymphocytes to immunogenic responses in the presence of antigen and cytokines. However, in diseased individuals the immune system is not naïve, but tolerant, i.e. ‘instructed’ for tumour tissue protecting responses. These memory T-lymphocytes have transcription factors that enable them to respond similarly to recall antigens as they did before (54-56). Thus once established, immune responses are rather rigid, and do not easily change their nature. Moreover, the antigen-specific tolerogenic T-lymphocytes mostly reside inside the tumour tissue (57). Thus tolerogenic cells do not differ from other memory T-lymphocytes that commonly circulate through the body, spending most time in their target tissue (i.e. tumour). If T-cell growth factors are produced due to the induction of an antitumour immune response, tolerogenic memory T-lymphocytes are activated in the presence of the tumour antigen. These cells divide and respond as determined by the transcriptions factors activated during immunological priming, and thus the recall antigens of vaccination result in more tolerogenic memory cells.
Figure 1 shows that therapeutic vaccination might amplify cells involved in both tumour tolerance and rejection, which might nullify the therapeutic efficacy. Some studies even suggest that therapeutic vaccination is detrimental (58). Because of the functional stability of (tolerogenic) T-lymphocytes (54, 55, 59), little is expected from subtle blocking of a single co-stimulatory molecule.
When clinical results are small, often the (antigenic) dose is increased or vaccination is repeated in order to induce more powerful responses. Increasing the number of responsive T-lymphocytes, might be accompanied by a higher level of tolerogenic T-cells, because of higher cytokine levels at the target tissue. Therapeutic cancer vaccines induce antibodies and cytotoxic T-lymphocytes against prostate cancer antigens. In the prophylactic setting, these immune responses are a good predictor of protection. However, in the therapeutic setting, vaccine-induced immune responses fail to be clinically effective, presumably because of the ongoing presence of antigen-specific tolerogenic lymphocytes that reside inside and nearby the tumour. A phase III study targeting CTLA4 to deplete regulatory T-cells systemically yielded minimal results with serious toxicity (60). The problem is not simply the presence of tumour at the moment of vaccination, since therapeutic vaccination strategy in patients with cleared tumours also yielded minimal results (61). Considering that tolerogenic lymphocytes are present that specifically are instructed at the immunological recall site, i.e. the vaccine depot, this might not be a complete surprise to immunologists.
In understanding the inefficacy of therapeutic vaccination, we would like to re-visit and deepen some questions. How can it be that vaccination is protective when applied in a prophylactic setting, but is not curative when applied in a therapeutic setting? In other words, what is the difference between immunological intervention in the prophylactic and the therapeutic settings? Tumour-bearing patients differ from healthy persons in two properties, their immunological status and, the presence of tumour as a ‘de novo organ’ that maintains tissue homeostasis. In other words: How can this acquired immune-protected status of the tumour be broken?
Immunotherapy Becoming Effective by Destroying Tumour Homeostasis
Patients with cancer have acquired antigen-specific tolerance. Thus, how can we break tolerance and treat patients in a clinically effective way? Immunological tolerance to organs cannot be broken easily, since if tolerance against organs is lost it would cause autoimmune disorders incompatible with life. Thus, studies should focus on neutralizing antigen-specific tolerance. But how can we do this, knowing the wide spectrum of tumour associated antigens? If only tolerance was broken of one or two antigens on the tumour, the tumour cells would be protected by the remaining tolerogenic T-lymphocytes.
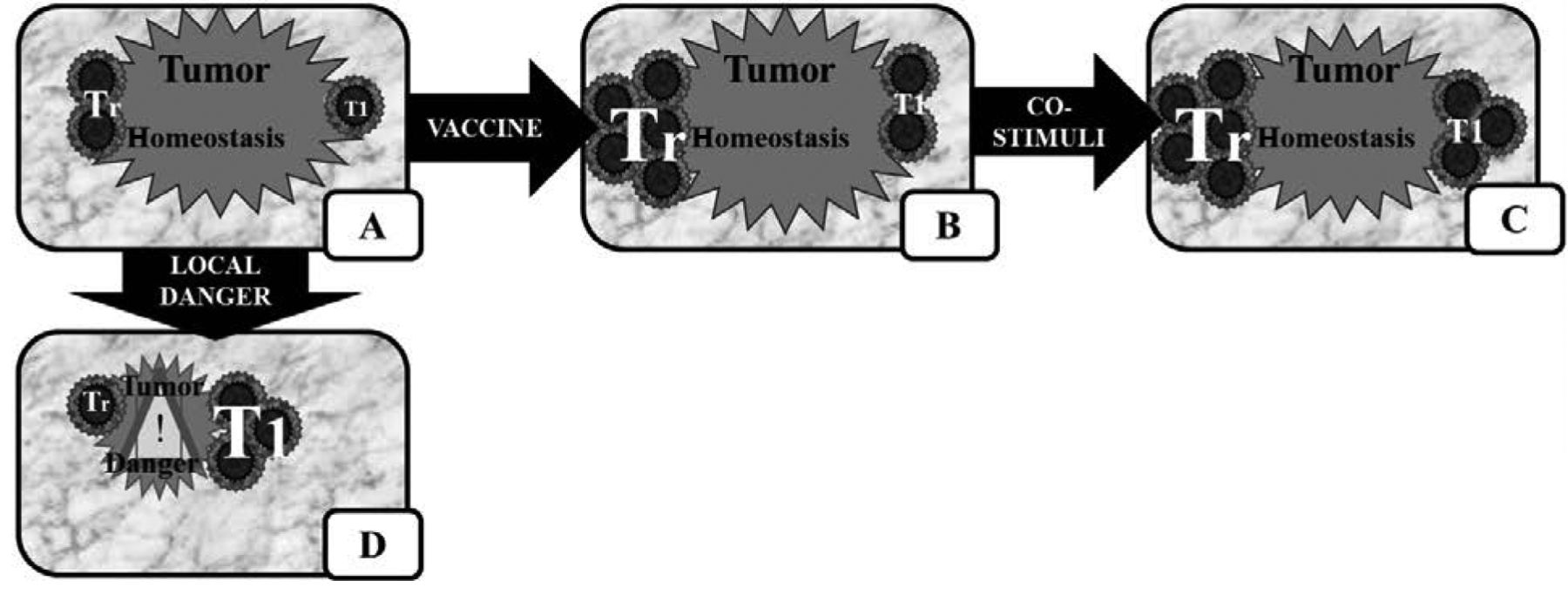
A: Default immune status at a tumour. B: Immune status after vaccination. C: Immune status after vaccination and co-stimulation. D: Immune status after local ‘danger’ therapy. Tr, Regulatory or suppressive T (tolerogenic) lymphocytes; T1, type 1 helper or cytotoxic T-lymphocytes. Within tumour homeostasis regulatory T-lymphocytes actively protect the tissue from (immunological) harm (A). When a patient is vaccinated (B) tolerogenic and effector responses both increase. The effector responses are the direct result of the vaccination, but the presence of antigen plus T-cell growth factors (Interleukin-2, and - 15) also increases the number of tolerogenic cells. Since both tolerogenic and effector cells are increased in number and activity, the immunological awareness of the tumour is increased. Nevertheless, the tumour tissue remains actively protected. Similarly when co-stimulated, both tolerogenic and immunogenic lymphocytes are amplified to a similar extent, since both populations are activated in the same environment (i.e. at the tumour site) with the same T-cell growth factors (i.e. cytokines). Thus populations of both cells will increase (C). The effective option seems to be to induce local inflammation signals, either directly by cytokines, or indirectly by inducing local ‘danger’ in the tissue (D). Tumour cell killing releases antigen in the presence of danger signals, e.g. due to dying cells. The tolerogenic T-lymphocytes are destroyed or re-instructed to become effector cells, allowing the installation of tumour immunity.
Antigen-specific T-lymphocytes home preferentially to their target tissue (62, 63). They are crucial in maintaining tissue homeostasis (56) and depend on tissue homeostasis and antigens. In the case of tumour-bearing patients the antigen-specific T-lymphocytes are tolerogenic cells. Thus if their target tissue is destroyed, these tolerogenic cells might be open for immunological reinstruction or destruction.
Many studies indicate that cancer immunotherapy other than therapeutic vaccination can lead to clinically relevant effects [reviewed in (40)]. The crux to understanding tumour immunology resides in understanding the mechanisms evoked by effective therapies. From a physiological point of view the tumour is a de novo organ, with quite normal homeostasis and absence of immunological danger (64, 65). The presence of danger is the key instruction for the immune system to discriminate between tolerogenic and immunogenic responses towards antigens. In the case of cancer the immune system recognizes danger by endogenous danger signals, i.e. the induction of cell death or inflammation. Thus immunological danger could be induced in two different ways.
Firstly, direct destruction of (a part of) the tumour would be read as immunological danger. Radiotherapy and chemotherapy are cytotoxic and destroy tumour homeostasis. Cell death induces the maturation of DCs in vitro, ex vivo and in vivo (66-68). DCs are crucial in initiating immune responses (69, 70). Animal models show that radiotherapy and chemotherapy may aid immunotherapy (71-76) and local radiotherapy can synergize with systemic anticancer treatment (77), as in prostate cancer (78). Chemotherapy, radiotherapy and hormone therapy induce antibodies and cellular immune responses against prostate cancer (76, 79, 80) and other tumours (74). A preliminary study has shown a therapeutic effect in preventing cancer recurrence by the combination of vaccination and irradiation (81). Induction of immunity could be important in the synergy between radiotherapy and chemotherapy with immunotherapy observed in the clinic for other tumour types (82-87). Research in an autologous animal model suggests that chemotherapy with cyclophosphamide could synergize with immunotherapy (76), this was confirmed by a phase II clinical trial (88).
Secondly, causing local inflammation can be seen as immunological danger. Local initiation is crucial in the normal development of immune responses. Many tumours deploy local immune inhibition to maintain physiology (89); inflammatory killing of tumour cells could break this status quo (90, 91). Deliberate induction of intra-tumoural inflammation can induce T-lymphocytes (92, 93) or reprogram regulatory T-lymphocytes in situ (59). Thus inducing intra-tumoural inflammation can be clinically effective against cancer (94, 95). The principle of inducing inflammation against cancer has been successfully employed by Bacillus Calmette–Guérin (BCG) therapy for bladder carcinoma (96-100). Systemic BCG therapy would cause a life-threatening disease, thus BCG is only applied locally. BCG induces inflammation (101) by local mediators such as IL2 (102, 103). Local, rather than systemic IL2 is active against bladder cancer (104-107) and other forms of cancer (40, 41, 98, 108, 109). These effects of IL2 are not attributable to systemic IL2, since only local treatment shows clinically relevant efficacy against nasopharyngeal carcinoma (83, 110) and metastasized melanoma (111-115). Local, rather than systemic immune stimulation is effective, as systemic immune stimulation induces immunosuppressive feedback loops (40).
Conclusion
Vaccination has shown its clinical efficacy in the prophylactic setting, but not in the therapeutic setting. Therapeutic vaccination stimulates both immunogenic and tolerogenic responses, thereby nullifying its overall clinical efficacy. Thus, vaccination might have immunological effects, but little therapeutic effect. We hypothesize that immune protection might be due to tumour homeostasis, likely controlled by tolerogenic T-lymphocytes, such as regulatory and suppressor T-cells. Tumour homeostasis might be overruled by immunological danger in two different mechanisms. The first mechanism is by induction of tumour death by locally-applied cytotoxic anticancer therapy; the second is by induction of inflammation inside the tumour. Initiating local immune responses in the tumour seems to be required for effective anticancer immunotherapy. Several studies have shown that this is a possible approach in the pre-clinical and clinical setting for a variety of tumour types.
Acknowledgements
JJLJ acknowledges a grant from Stichting Nationaal Fonds tegen kanker (SNFK), Amsterdam, the Netherlands.
Footnotes
-
This article is freely accessible online.
- Received March 14, 2014.
- Revision received May 4, 2014.
- Accepted May 6, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
- Article
- Abstract
- Therapeutic Vaccines Trigger Anticancer Immune Responses
- Therapeutic Vaccination Yields No Clinically Relevant Anticancer Effects
- Evaluation of the Lack of Clinical Efficacy
- Tumour-bearing Patients Are Antigen-specific Tolerant
- Immunotherapy Becoming Effective by Destroying Tumour Homeostasis
- Conclusion
- Acknowledgements
- Footnotes
- References
- Figures & Data
- Info & Metrics