


Abstract
Background: We conducted a prospective, multicenter cooperative study to compare two courses of modified intermediate-dose cytarabine (Ara-C) (mIDAC; Ara-C at a dose of 1.0 g/m2 every 12 hours for 5 days) versus high-dose Ara-C (HDAC; Ara-C at a dose of 2.0 g/m2 every 12 hours for 5 days) in post-remission therapy for acute myeloid leukemia (AML) to confirm the post-remission antileukemic efficacy and safety of mIDAC. Patients and Methods: Twenty-six newly diagnosed patients with AML underwent remission induction therapy consisted of behenoyl Ara-C, mitoxantrone, etoposide, and 6-mercaptopurine. Post-remission therapy included four courses of consolidation and four courses of intensification. Patients who achieved complete remission (CR) were randomly assigned to mIDAC or HDAC for the second course of consolidation. The third course of intensification was the same as the second course of consolidation. Other post-remission therapies were the same in each group. Results: Twenty-two patients (84.6%) achieved CR and 21 patients were randomly assigned to receive either mIDAC (n=11) or HDAC (n=10). The predicted 4-year relapse-free survival for the mIDAC group and for the HDAC group were 49% and 56%, respectively (p=0.86). Although HDAC developed severe leukocytopenia compared to mIDAC, there were no significant differences between HDAC and mIDAC in the incidence of ≥grade 3 and ≥grade 4 documented infections. The mean lowest white blood cell count (WBC) after HDAC was significantly lower than that after mIDAC (0.208±0.120×103/mm3 and 0.459±0.333×103/mm3, respectively, p<0.05). The time to WBC recovery to 2.0×103/mm3 after HDAC was significantly longer than that after mIDAC (34.3±12.1 days and 27.1±9.5 days, respectively, p<0.05). Conclusion: This study suggests that mIDAC may have an equivalent post-remission antileukemic efficacy to HDAC with less myelosuppression for AML patients.
Cytarabine (Ara-C) is the key chemotherapeutic agent for acute myeloid leukemia (AML). The complete remission (CR) rate is approximately 60% to 80% in newly diagnosed younger adult patients with AML who were treated with a combination of anthracycline and a conventional dose of Ara-C (1, 2). In post-remission therapy, high-dose Ara-C (HDAC) at a dose of 3.0 g/m2, given twice daily on days 1, 3, and 5, resulted in superior overall survival (OS) and relapse-free survival (RFS) than Ara-C at 100 mg/m2 daily or 400 mg/m2 daily (3). RFS was significantly superior in patients with core-binding factor chromosome abnormalities (4). However, HDAC toxicities are severe, especially in patients over 60 years of age (3). Furthermore, pharmacologically, the plasma Ara-C concentration peak was much higher than the 10 μM required to saturate deoxycytidine kinase for phosphorylating Ara-C to its intracellular active metabolite, Ara-C 5’-triphosphate (5, 6). An intermediate-dose Ara-C (IDAC, Ara-C at a dose of 500 mg/m2, every 12 hours) proposed by van Prooijen et al. was based on the pharmacological finding that this dose was sufficient to achieve a steady-state plasma concentration of about 10 μM (7). The problems with IDAC were an insufficient plasma concentration to overcome Ara-C resistance (8-10) and a low concentration in the cerebrospinal fluid (7). Therefore, we proposed a modified IDAC (mIDAC) using a dose of 1.0 g/m2, given twice daily on days 1-5, for patients with acute leukemia, and previously reported that mIDAC provides a sufficient plasma Ara-C level with a concomitant therapeutic concentration in the cerebrospinal fluid (11). We conducted the present prospective, multicenter cooperative study to compare two courses of mIDAC versus HDAC in post-remission therapy for AML to confirm the post-remission antileukemic efficacy and safety of mIDAC.
Patients and Methods
Patients. From January 2002 to June 2006, 26 newly diagnosed AML patients were registered from four participating institutions belonging to the Hokuriku Hematology Oncology Study Group. AML was diagnosed by the French-American-British (FAB) classification at each institution. M3 was not registered. Eligibility criteria included adequate function of the liver, kidney, heart and lungs. Patients who had prior myelodysplastic syndromes or who received prior chemotherapy for other malignancies were not eligible. The study was approved by Institutional Review Boards at each institution. All patients provided written informed consent in accordance with the Declaration of Helsinki before registration.
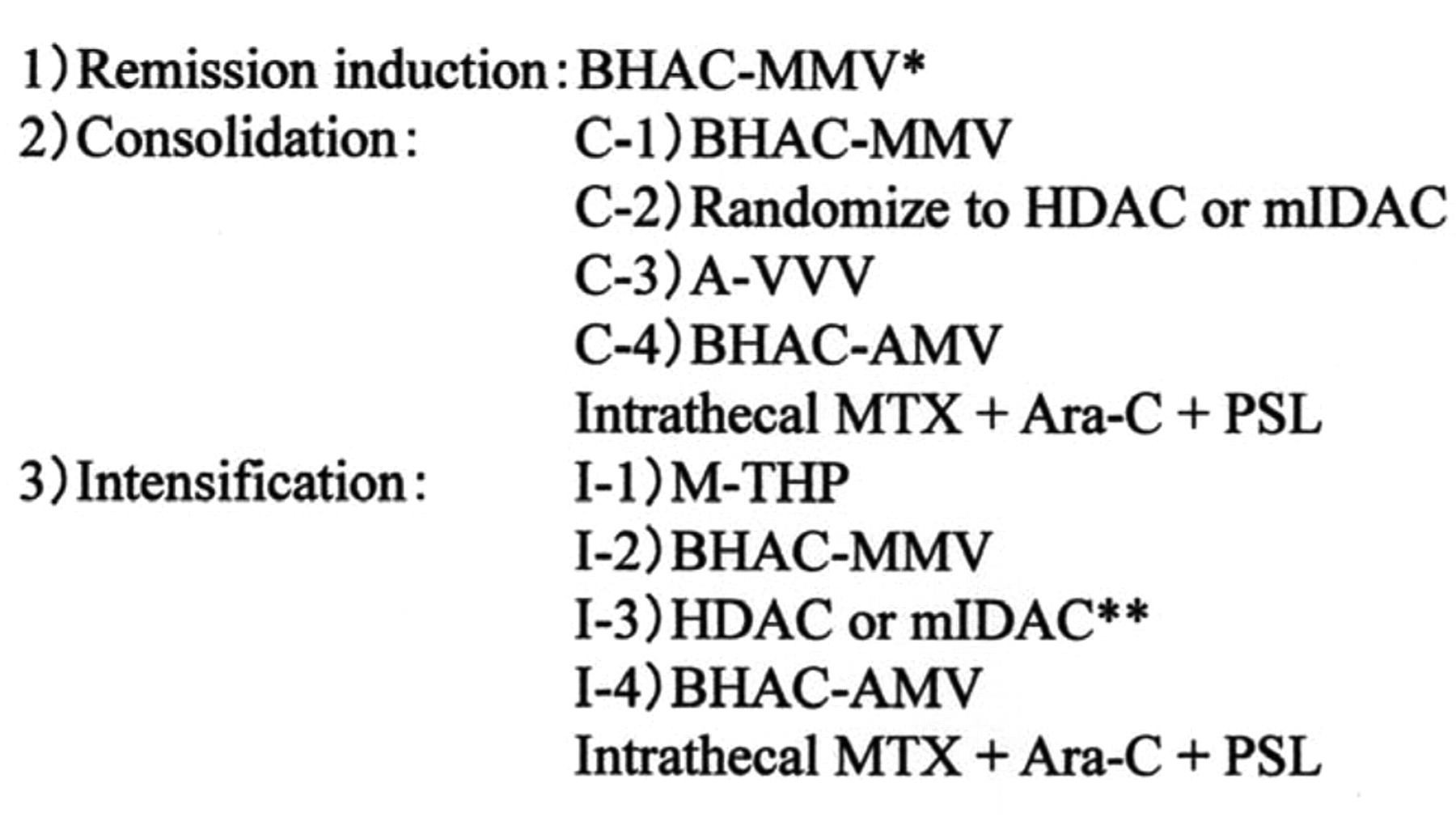
Remission induction and post-remission therapy. The treatment scheme is shown in Figure 1. Remission induction therapy consisted of behenoyl Ara-C (BHAC; 170 mg/m2 for 7 days), mitoxantrone (MIT; 4 mg/m2 for 3 days), etoposide (VP-16; 70 mg/m2 for 4 days), and 6-mercaptopurine (6-MP; 100 mg/m2 for 7 days) (BHAC-MMV). Remission induction therapy was given in a response-oriented individualized manner. BHAC and 6-MP were continued until the bone marrow became severely hypoplastic with blasts fewer than 20%. Additional MIT and VP-16 were given on days 5-7 and on day 7, respectively. If patients did not achieve CR by the first course, the same therapy was repeated. Patients who achieved CR were randomly assigned to mIDAC (Ara-C at a dose of 1.0 g/m2 in one hour infusions every 12 hours for 5 days) or HDAC (Ara-C at a dose of 2.0 g/m2 in one hour infusions every 12 hours for 5 days) at the second course of consolidation. The third course of intensification was the same as the second course of consolidation. Other post-remission therapies were the same in each group. The first course of consolidation and the second course of intensification had the same schedule as the induction therapy. The third course of consolidation consisted of Ara-C (100 mg/m2 for 6 days), VP-16 (70 mg/m2 for 4 days), vincristine (0.8 mg/m2 for 1 day), and vinblastine (6 mg/m2 for 1 day) (A-VVV). The fourth course of consolidation and the fourth course of intensification consisted of BHAC (170 mg/m2 for 7 days), aclarubicin (14 mg/m2 for 7 days), VP-16 (70 mg/m2 for 4 days), and 6-MP (100 mg/m2 for 7 days) (BHAC-AMV). The first course of intensification consisted of methotrexate (MTX; 300 mg/m2 for 1 day) and pirarubicin (30 mg/m2 for 1 day) (M-THP). For the prophylaxis of CNS leukemia, intrathecal Ara-C (30 mg), MTX (10 mg), and prednisolone (10 mg) were given after the fourth course of consolidation and the fourth course of intensification (BHAC-AMV). Each post-remission therapy was started as soon as possible after white blood cells count (WBC) and platelet count (PLT) recovered to more than 3.0×103/mm3 and 80×103/mm3, respectively. During myelosuppression after mIDAC or HDAC, patients were accommodated in laminar air flow rooms to prevent the development of infections. Sufficient supportive care, including prophylactic antibacterial or antifungal agents, and granulocyte colony-stimulating factor (G-CSF) were given if needed.

Treatment scheme. BHAC-MMV indicates behenoyl Ara-C (BHAC), mitoxantrone, etoposide (VP-16) and 6-mercaptopurine (6-MP); HDAC, high-dose Ara-C; mIDAC, modified intermediate-dose Ara-C; A-VVV, Ara-C, VP-16, vincristine and vinblastine; BHAC-AMV, BHAC, aclarubicin, VP-16 and 6-MP; and M-THP, methotrexate and pirarubicin. Patients who achieved CR were randomly assigned to mIDAC or HDAC at the second course of consolidation. *If patients did not achieve complete remission by the first course, the same therapy was repeated. **The third course of intensification was same as the second course of consolidation.
Assessments. Adverse events related to mIDAC or HDAC, the primary endpoint of the randomization, were graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Events, version 2.0 (12). The secondary endpoints were RFS. CR was defined as the presence of all of the following: fewer than 5% blasts in the bone marrow, no leukemia blasts in the peripheral blood, recovery of peripheral neutrophil counts to over 1.0×103/mm3, and PLT to over 100×103/mm3. Relapse was defined as the presence of at least one of the following: recurrence of more than 10% leukemia cells in the bone marrow, any leukemia cells in the peripheral blood, and the appearance of extramedullary leukemia. RFS was calculated from the day when the first CR was achieved to the day of the first relapse. Patients who underwent allogeneic stem cell transplantation were censored on the date of transplantation.
Statistical analysis. The incidences of any adverse events were compared using Fisher's exact test. The lowest WBC and the time to WBC recovery to more than 2.0×103/mm3 after mIDAC or HDAC are expressed as the mean±standard deviation. Differences were analyzed using Student's t-test. Time-to-event analysis was performed according to the Kaplan–Meier method, and the log-rank test was applied to assess differences between subgroups; p<0.05 was considered significant.
Patients' characteristics for the modified intermediate-dose Ara-C (mIDAC) group and high-dose Ara-C (HDAC) group.
Results
Patients' characteristics. The median age of the 26 patients was 52 years (range 20-64 years). Seventeen were male and nine were female. The number of patients belonging to FAB classification subgroups M0, M1, M2, M4, M5, M6, and M7 were 0, 2, 14, 2, 6, 1 and 1, respectively. The number of patients classified with Eastern Cooperative Oncology Group performance status 0, 1, 2 and 3 were 6, 16, 2 and 2, respectively. Karyotype analyses were available for 24 patients: one was classified in the favorable-risk group, 20 were in the intermediate-risk group, and 3 were in the adverse-risk group, according to the Medical Research Council classification (13).
Response to induction therapy and randomization. Twenty-two patients (84.6%) achieved CR; sixteen patients by one course and six patients by two courses. The remaining four patients were refractory to the induction therapy. Of the 22 patients who achieved CR, 21 patients were randomly assigned to receive either mIDAC (n=11) or HDAC (n=10) at the second course of consolidation. The patient characteristics of each group are shown in Table I. One patient did not undergo randomization because he developed another disease (brain tumor) after the first course of consolidation. Four patients received allogeneic stem cell transplantation during the first CR.

Kaplan-Meier curves for relapse-free survival for the modified intermediate-dose Ara-C (mIDAC) group and high-dose Ara-C (HDAC) group.
Adverse events. There were no significant differences between mIDAC and HDAC in the incidence ≥grade 3 (10/11 and 9/10, respectively, p=1) and ≥grade 4 documented infections (1/11 and 0/10, respectively, p=0.47). Another ≥grade 3 non-hematological adverse event (gastrointestinal event) developed in only one patient who received mIDAC. Central nervous toxicities over grade 3 were not seen in any group. HDAC induced severe leukocytopenia compared with mIDAC. The mean lowest WBC after HDAC was significantly lower than that after mIDAC (0.208±0.120×103/mm3 and 0.459±0.333 ×103/mm3, respectively, p<0.05). The time to WBC recovery to 2.0×103/mm3 after HDAC was significant longer than that after mIDAC (34.3±12.1 days and 27.1±9.5 days, respectively, p<0.05).
RFS. The median follow-up from starting the induction therapy was 20 months (range 5-60 months) in surviving patients. The predicted 4-year RFS for the mIDAC group and for the HDAC group were 49% and 56%, respectively (p=0.86, Figure 2).
Discussion
Our study demonstrated that mIDAC may have an equivalent post-remission antileukemic efficacy to HDAC with less myelosuppression for AML patients.
Based on the results of the Cancer and Leukemia Group B (CALGB) study (3), HDAC is generally used as a postremisson therapy for AML, especially in patients with core-binding factor chromosome abnormalities (4). CALGB also reported that patients with RAS mutations benefit more from a higher Ara-C dose of consolidation therapy than patients with wild-type RAS (14). Kern and Estey reported that although induction with HDAC did not improve the CR rate, long-term disease control and OS improved in three randomized trials which compared HDAC with a conventional dose of Ara-C (15).
On the other hand, there are some contrary reports. The Dutch-Belgian Cooperative Trial Group for Hemato-Oncology (HOVON) and the Swiss Group for Clinical Cancer Research (SAKK) compared the efficacy of IDAC to HDAC as a remission induction therapy (16). In the IDAC group, patients received 200 mg/m2 Ara-C by continuous intravenous infusion for 24 hours in cycle 1, and 1 g/m2 Ara-C by 3-hour infusion twice daily in cycle 2. In the HDAC group, patients received 1 g/m2 Ara-C by 3-hour infusion every 12 hours in cycle 1, and 2 g/m2 Ara-C by 6-hour infusion twice daily in cycle 2. At a median follow-up of 5 years, no significant differences in CR rates, event-free survival, or OS were noted between IDAC and HDAC. It was concluded that increasing the dose of Ara-C to more than 1 g/m2 provides no greater antileukemia activity. Cycle 2 of the remission-induction therapy of the HOVON-SAKK study is similar to the consolidation therapy because about 60% of patients had already obtained CR before cycle 2. Furthermore, the Ara-C dose per administration of IDAC and HDAC in cycle 2 of the HOVON-SAKK study was equal to that of the mIDAC and HDAC in post-remission therapy of the present study. Accordingly, our results almost completely coincide with those of the HOVON-SAKK study. The Australasian Leukaemia and Lymphoma Group AML trial number 7 protocol indicated that HDAC did not confer additional benefits compared to a conventional dose of Ara-C for consolidation (17). The Japan Adult Leukemia Study Group AML201 study compared four courses of multi-agent chemotherapy with three courses of HDAC for consolidation. Multi-agent chemotherapy was as effective as HDAC in disease-free survival and OS. The HDAC regimen resulted in a beneficial effect on disease-free survival only in the favorable cytogenetic group (18).
Almost all studies demonstrated that HDAC is more toxic than a conventional dose of Ara-C or IDAC. Severe hematological and non-hematological toxicities sometimes induce the delay or discontinuation of chemotherapy. For example, the HOVON-SAKK study revealed that the number of deaths in the first three months was greater in the HDAC group (16). The therapy-related toxicities of HDAC may result in insufficient effects on the improvement of OS. In our study, there were no differences between the two groups regarding developments of ≥grade 3 documented infection, although HDAC led to a more severe leukocytopenia than did mIDAC. Laminar air flow rooms, prophylactic antibacterial or antifungal agents, and G-CSF may be effective to prevent the aggravation of documented infections.
In conclusion, mIDAC may have an equivalent post-remission antileukemic efficacy to that of HDAC, with less myelosuppression for AML patients. Larger scale prospective trials comparing HDAC, mIDAC and a conventional dose of Ara-C should be conducted to confirm the optimal dose of Ara-C or the best post-remission therapy for AML.
Acknowledgements
The Authors would like to thank the clinicians from the four institutions who entered their patients into this study and provided data.
Footnotes
-
This article is freely accessible online.
-
Conflict of interest
The Authors declare no conflicts of interest.
- Received November 3, 2011.
- Revision received December 12, 2011.
- Accepted December 13, 2011.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.