


Abstract
Purpose: radical prostatectomy (RP) is affected by urinary incontinence (UI) that, even if temporary, can severely impact patients quality of life. We investigated if a post surgery tutored and personal trained pelvic floor re-educational program improves continence recovery more than pelvic floor exercises performed by patients on their own. Patients and Methods: 332 incontinent (>1 pad/daily) patients (pts) submitted to RP between 2006 and 2008 were prospectively randomized in group A (166 pts) and group B (166 pts). The first group performed an intensive tutored pelvic training program and the second formed the control group. The follow-up was at one year and the self report of recovery of continence was measured every 3, 6 and 12 months. Results: the median time of continence recovery in group A was 44±2 days, while in group B it was 76±4 days. Patients enrolled in the pelvic floor re-educational dedicated program (group A) achieved continence earlier than the control group (group B). In fact, the number of incontinent patients at the different follow-up intervals was higher for the control group than for the treatment group. Conclusion: We have demonstrated that a post RP personal training program of pelvic muscle re-education supported by a physician and nurses expert in continence disorders have a benefit in future continence.
Nowadays, prostate cancer is an endemic disease and consequently its related complications, especially urinary incontinence (UI), are widespread phenomena. Despite the improvements in our knowledge of pelvic floor anatomy, UI resulting from radical prostatectomy (RP) is common and has an important impact on patients' quality of life (1). The literature reports wide ranges of prevalence of incontinence depending on different methods of data collection and definition, with 5 to 60% of patients experiencing mild to severe symptoms and fewer than 5% of patients requiring surgical treatment at less than one year from RP (2-4). However, the global incontinence rates are seen to decrease with time (5-20% at one year since RP) (5). The first objective of all studies on radical prostatectomy is the complete recovery of continence. A secondary objective addresses lowering the grade of UI. The mechanism of UI after RP can be related to many factors such as internal/external sphincter deficiency (SD) induced by either surgical injury or denervation, detrusor instability (DI), or decreased bladder compliance (5, 6). Loss of integrity of the muscle structures and/or an anastomosis stricture can be considered other major causes (2, 7). In order to minimize the effects of such conditions, various treatment modalities are used for their advantages in continence recovery (1). Treatment options are divided into two main categories: conservative and non-conservative management. Literature reports that non-invasive therapy (pelvic floor exercises) must be applied in the first six to twelve months (3). Their rationale is to improve the muscular strength and the blood supply of the external sphincter (5). Even if the role of such exercises is clear, their benefit is not well understood (5, 7). Candidates for physiotherapy are basically patients psychologically motivated to have an early recovery of continence and those with a loss of pelvic floor muscle tone. Since 1948 when Kegel proposed pelvic floor muscle exercises (PFME) for enhancing sphincter tone, urologists and physical therapists have been training post prostatectomy patients to perform pelvic exercises on their own both preoperatively and postoperatively. It is well known that the effectiveness of physiotherapy can depend on psychological support that may have an effect on patient motivation (2). No studies have reported if pelvic training needs to be personalized according to the state and/or the type of incontinence (continuous leakage, leakage induced by stress or complete incontinence). In this study, we investigated if a post-surgical tutored program of pelvic floor re-education improves continence recovery more than pelvic floor exercised executed by patients on their own.
Patients and Methods
Between January 2006 and December 2008, 670 consecutive patients who had undergone retropubic radical prostatectomy either open or laparoscopic for clinical T1c prostate cancer we enrolled. They received oral and written information from a urologist and a urodynamic advisor at the time of urethral catheter removal (16 days after RP), regarding pelvic floor anatomy and on how to correctly contract pelvic muscles in a supine position while relaxing abdominal muscles (Kegel exercises). Pelvic floor muscle endurance was assessed by digital anal control. Patients muscular tone was estimated as low, mild and severe endurance. They were scheduled for the first month to perform exercises at home, consisting in three sets of 30 contractions daily, holding the contraction alternatively 1-2 seconds and 6-7 seconds without gluteal and abdominal muscle involvement. At one month from catheter removal, 512 patients were considered eligible for the study. Exclusion criteria were lack of cooperation (22 patients), pre-operative incontinence and early recovery of continence (158 patients). Moderate to severe incontinence at 30 days after catheter removal was considered the condition for being enrolled. Only 332 incontinent patients met this inclusion criterias and were prospectively randomized into a treatment group (group A), mean age 67 years, or a control group (group B), mean age 66.5 years. The 166 patients of group B were asked to continue performing the same Kegel exercises at home and for the duration of the follow-up period. On the other hand, the 166 patients of group A, were instructed how to correctly continue Kegel exercises at home and followed an intensive guided rehabilitation program. The first treatment session included both a feedback (BF) of correct contraction and instructions as to how to perform voluntary sphincter contractions concomitant to defined and progressive movements named automaticity exercises (AE). During the second session every patient was submitted to 10 sets of pelvic floor electrical stimulation (PFES) lasting 15 minutes each. The rehabilitation program was executed at our Hospital daily for BF and teaching AE session and for a mean period of 2-3 weeks for PFES. On these occasions the urologists and the urodynamics advisors worked one on one with patients to differentiate the type and intensity of muscle training and the size and shape of pads for each reported incontinence condition. The trainers also helped the patients to obtain free pads and had the role of both encouraging them to do exercises and also correcting those patients not performing valid pelvic contractions.
The follow-up for both groups lasted a year and the recovery of continence was measured at 3, 6 and 12 months. Preoperatively and postoperatively at 3, 6 and 12 months, all the patients involved in the study were asked to fill in both the ICIQ-male questionnaire (8) for evaluating lower urinary tract symptoms and their impact on quality of life, and the RAND 36-Item Health Survey (9) that provides an indication of perceived change in health. All patient data were collected by the same urologist expert in urinary disorders with the support of a urodynamics advisor. The self report for the recovery of continence was defined as no use of pads or a mild leakage needing 2 mini-pads a day. At each check up, control the patients were asked to explain if the continence recovery was complete or in case of incontinence the entity of urine loss and the conditions provoking it. Statistical analysis describing patient characteristics and all results was carried out. The analyses were conducted in terms of mean and standard deviation (SD). Student's t-test was used to compare different classes of age (younger than 50 years, between 50 and 70 years and older than 70 years) between the two groups. Multivariate analysis with the chi-square test was performed to test for correlation, within the two groups, relating to the presence of risk factors for incontinence such as any previous surgical treatment of the prostate gland, associated co-morbidities, the type of surgical technique, and the positive surgical margins. P-values less than 0.05 were considered statistically significant. Kaplan-Maier curve was employed to verify differences in persistence of urine loss. A trend analysis was used to show the different recovery of continence in the two groups.
Results
The characteristics of two groups regarding age, prior prostate surgical treatments such as transurethral and transvesical simple prostatectomy, concomitant co-morbidities, surgical approach (open or laparoscopic), the nerve sparing procedure and the presence of positive surgical margins were not found as significantly different factors in the two groups (p>0.05) (Table I). The ICIQ-male and the RAND 36-Item Health Survey questionnaire were correctly filled in and returned by fewer than 10% of the patients. For this reason it was not possible to elaborate the results understanding how post radical prostatectomy incontinence impacted patients' quality of life and the health status. The median time of continence recovery in group A was 44±2 days, while in group B it was 76±4 days. All patients regained continence (0 or 2 minipads/daily) at one year after catheter removal, but the fine to recovery of continence was statistically significantly different for the two groups (p<0.01). In fact, the curve of Figure 1 shows that patients enrolled in the pelvic floor re-educational dedicated program (group A) achieved continence earlier than patients who were not tutored in performing pelvic floor physical therapy (group B).
Discussion
Prostate cancer is a widespread disease mainly diagnosed in those men still of a working age, in which the uncontrolled loss of urine can generate social implications even if only temporary. The extensive use of pads has a economic cost in addition to the risk of local and urinary infection induced by bacterial contamination. The literature reports that several risk factors may play a role in the genesis of incontinence, even if their actual involvement is not clear. In our study, we found that the patients who showed an early recovery of continence were not significantly younger or healthier than the controls. It is widely known that the surgical technique used is one of the most important causes of postsurgery incontinence, due to the loss of integrity of the distal sphincter fibres inducing the inability of urine complete restore. The difference in continence recovery, either as time after catheter removal, or after 6 or 12 months, among RP patients has been attributed to the neurovascular bundle-sparing status and its effect on intraurethral pressure (10). In our experience, patients of the two groups were not significantly different regarding the surgical technique used (open or laparoscopic RP), and the nerve-sparing or non nerve-sparing approach. Since surgical correction of UI represents the last resort because of its invasive modality and poor results, physical therapy is the first approach within 12 months from RP.
Characteristics of the patient population.
Data from a recent Cochrane review showed that the role of conservative management in continence recovery after RP is not clear and unfortunately no trials have tested the efficacy of rehabilitation programs on quality-of-life status (5). Other elements that derived from this complete review are that all the trials considered lacked in methodology and in homogeneity of either continence definition, or sample, or in instruments to measure the severity of the incontinence or in the workout of the rehabilitation program. All literature results derived from the experience of a single institute. The great difference between a re-educational program and Kegel exercises alone performed at home consists in both the technical and psychological support. Recent data of Hofmann et al. indicate that the association of PFES or BF with Kegel exercises is of no additional benefit (11).
It is well known that if the perineal muscle tone is adequately developed, continence can be recovered by enhancing the paraurethral support. In this context, Kegel exercises, consecutive voluntary contraction and relaxation of pelvic muscles, have a target role. In fact, even if the sphincter is partially deficient, the external support of the elevatore ani muscle can contribute to continence control. The external sphincter activity and its ability to cope with and adapt to the stress of exercise is partially regulated by a reflex mechanism. To create an autonomic pelvic floor contraction to prevent a stress event through the activation of voluntary muscle contraction in response to increasing abdominal pressure, is one of the most difficult exerciseas for patient to do, but in our experience, it is demonstrated to help continence recovery. The difficulties in such exercise are mainly due to the lack of knowledge of which muscles are involved and which fibres need to be contracted and also because it is not easy to coordinate the urethral closing pressure in a uncontrolled urine leakage situation concomitant to increasing abdominal pressure. The majority of patients reported that they had a very difficult time in performing such contractions, gaining movement control about one and a half months after they started the re-education program.
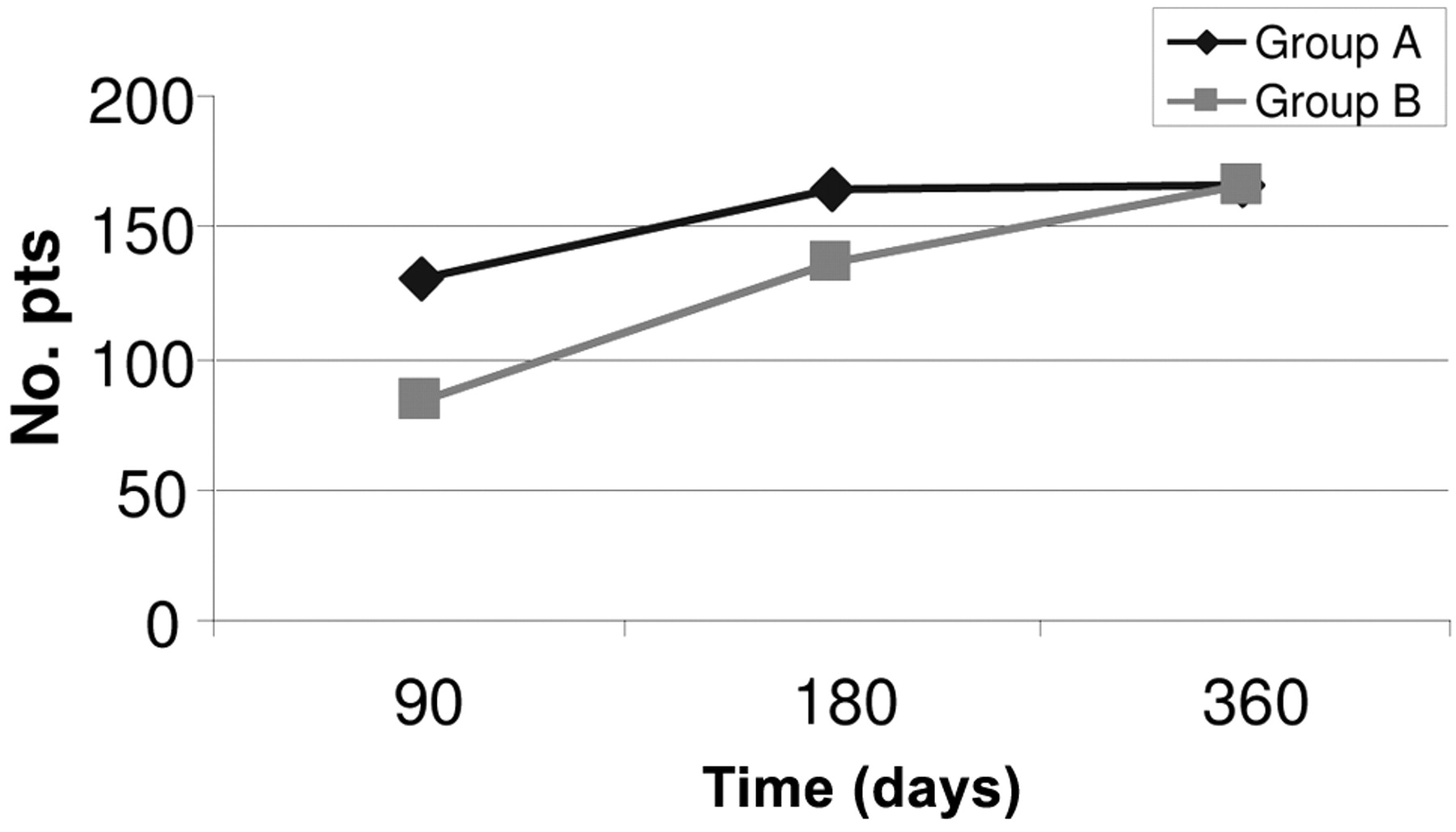
The patients of group A can be seen to have achieved continence significantly earlier than those of group B.
Another theory on which we based our re-educational program is that muscle fibres can be divided into two main types: slow twitch (type I) fibres, efficient in extended muscle contraction over a long time before they fatigue, and fast twitch fibres (type II). The latter are much better at generating short and swift contractions at the expense of much energy. Type I pelvic floor fibres are those preserving the urethral closure in a static condition by coping with external/internal sphincter muscle basal tone, which, in the case of deficiency, generally gives rise to the clinical condition of continuous leakage. Type II fibres are conversely activated in response to stress (leakage under stress if these fibres are damaged). In order to improve performance, it would be more useful to train different fibres for the different clinical conditions. The literature contains many articles regarding physical therapy after orthopaedic surgery and many protocols exist for arm, leg, knee and shoulder muscle tone recovery. Unfortunately, no study has addressed this theory for pelvic floor muscles and rehabilitation of perineal muscles is still an empirical matter. The right time to start a pelvic floor training after surgery and the amount and type of exercises for each session is still unclear. In our research, before starting intensive training, we allowed time for patients to recover continence on their own by performing Kegel exercises at home (no one was submitted to any intensive exercise prior to a month after surgery). In fact, intensive training with, for example, more than 30 pelvic contractions and for more than 3 times a day can determine severe pelvic and sovrapubic pain after exercise. In any event, muscular tone and strength inhibition induced by surgery through partial tissue ischemia and fibre damage isusually restored with time (7). For this reason, we developed a program with a progressive enhancement of pelvic muscle work and established that the appropiate time to start intensive exercises was at 40 days after surgery. In our trial, we found advantages in continence recovery in accordance with the experience of Willie et al. (12). The success of this pelvic training may also be associated with the activation of the different muscle fibres. For this reason, we personalized the muscular exercises to recovery of slow or fast twitch fibres. Patients also experienced a positive interaction with nurses expert in urodynamics and with the physician regarding psychological, medical and technical support. In fact, all patients involved in the program were strictly monitored during their exercises. The result of our re-educational program is the advantageous effects on the early recovery of continence for two main reasons: patient quality of life and the economic impact of incontinence. The goal of all existing trials is to find a standard protocol for the management of post radical prostatectomy incontinence in which all parameters such as time to start and workout are defined. This would certainly have an impact on urinary control and on psychological behaviour. In accordance with all literature data, our study demonstrates that the rate and the time to continence is shortened if patients are submitted to a postoperative personal training program of pelvic muscle re-education supported by physicians and nurses experienced in continence disorders.
Conclusion
The damage caused by RP is still an important issue, especially for patients who at the time of catheter removal complain of losing urine. Patients usually present different attitudes, either falling into depression and completely retiring at home, or taking an aggressive behaviour with their own surgeon. Neither of these behaviours help to resolve their condition. It is essential to investigate the genesis of postsurgical incontinence and consequently to involve patients in a personal re-educational program before considering any invasive treatment. In fact, according to the literature and to our experience, it seems that continence recovery can be achieved sooner with dedicated re-educational physical therapy. Nowadays, patients expectations are not only focused on urological outcomes but also on functional recovery both of continence and erectile function. We believe that our results further confirm that a targeted conservative re-educational therapy needs to be applied in clinical practice and that patients encouraged to achieve pelvic floor control themselves in order to recover continence early. Additional randomized studies, with a homogeneous sample, are still required.
Acknowledgements
We express a special thanks to our urodynamics advisors Mrs Ambra Mazzini and Mrs Marina Tura for their unique contribution to the development of this study and for the devotion they showed in training patients and always supporting them with their kind words. Thanks are also due to Dr. Roberta Ceccarelli for her support in interpreting data and reviewing statistical analysis.
Footnotes
- Received June 18, 2009.
- Revision received December 2, 2009.
- Accepted January 4, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Acupuncture for postprostatectomy incontinence: a systematic review
- First RAND-36-Item Health Survey in Three-dimensional Laparoscopy Cholecystectomy: A Prospective Randomized Study
- A Finnish Version of RAND-36-Item Health Survey Versus Structured Interview 8 Years Postoperatively
- Factors Associated With Treatment Satisfaction After Robot-assisted Radical Prostatectomy
- RAND-36-Item Health Survey: A Comprehensive Test for Long-term Outcome and Health Status Following Surgery