


Abstract
We report a 64-year-old woman with a 9-cm liver tumor in the left lateral section. The patient had neither hepatitis B or C virus infection, nor cirrhosis. Carbohydrate antigen 19-9 (CA 19-9) level was 1,889 U/ml. We also suspected bulky hilar lymph node metastasis, and a left lateral sectionectomy without lymph node dissection (R2) was performed. The pathological findings led to diagnosis of combined hepatocellular and cholangiocarcinoma. Three weeks post-operation, the patient underwent hepatic arterial infusion chemotherapy with cisplatin, fluorouracil, and mitomycin C. In addition, a total dose of 45 Gy of irradiation for the hilar lymph node was performed; while oral tegafur-uracil (UFT) has been administered for 10 years at a dose of 400 mg/day. The CA19-9 level of the patient was normalized after hepatectomy, hepatic arterial infusion, irradiation for hilar lymph node, and oral UFT administration. Currently, the patient is alive without any relapse for 12 years post-operation.
- Combined hepatocellular-cholangiocarcinoma
- multidisciplinary therapy
- chemoradiotherapy
- lymph-node metastasis
- long-term survivor
Combined hepatocellular and cholangiocarcinoma (cHCC-CC) is a rare tumor, which accounts for less than 2.0% of primary liver malignancies (1, 2). cHCC-CC has pathological components of both hepatocellular carcinoma (HCC) and cholangiocarcinoma (CC); therefore, cHCC-CC has features of both diseases, including several risk factors, tumor markers, imaging features, and prognostic factors. Conversely, the prognosis of cHCC-CC appears to be worse than that of HCC and comparable to CC (2-4). The most effective treatment for cHCC-CC is surgical resection. In addition, some reports show multidisciplinary treatment using chemotherapy and radiotherapy improves prognosis in patients with cHCC-CC better than surgical resection alone (5-8).
Herein, we report an extremely rare case of cHCC-CC treated with multidisciplinary therapy, whose disease-free survival is about 12 years after hepatectomy.
Case Report
A 64-year-old woman with severe abdominal pain, who was diagnosed as having a huge liver tumor, was referred to our hospital for surgical resection. The patient had neither hepatitis B or C infection, nor cirrhosis. Laboratory tests showed that the serum levels of alpha-fetoprotein (AFP), des-gamma-carboxy prothrombin (DCP), carcinoembryonic antigen (CEA), and carbohydrate antigen 19-9 (CA 19-9) were 4.4 ng/ml, 11 mAU/ml, 1.7 ng/ml, and 1,889 U/ml, respectively. In ultrasonography, the 9-cm diameter tumor was located in the left lateral sector without invasion of the left hepatic vein or left branch of Glisson's sheath. Due to the fact that the tumor was gradually enhanced from the periphery to the inner tumor area, from the arterial to the portal vein phase on enhanced-contrast computed tomography (CT) (Figure 1A and B), and serum CA19-9 level was very high, the tumor was diagnosed preoperatively as an intrahepatic CC (ICC). Moreover, lymph node metastasis was suspected because the lymph nodes along common hepatic artery (#8) and hepatoduodenal ligament (#12) were enlarged (Figure 1C and D), and abnormal accumulation was observed in positron emission tomography.
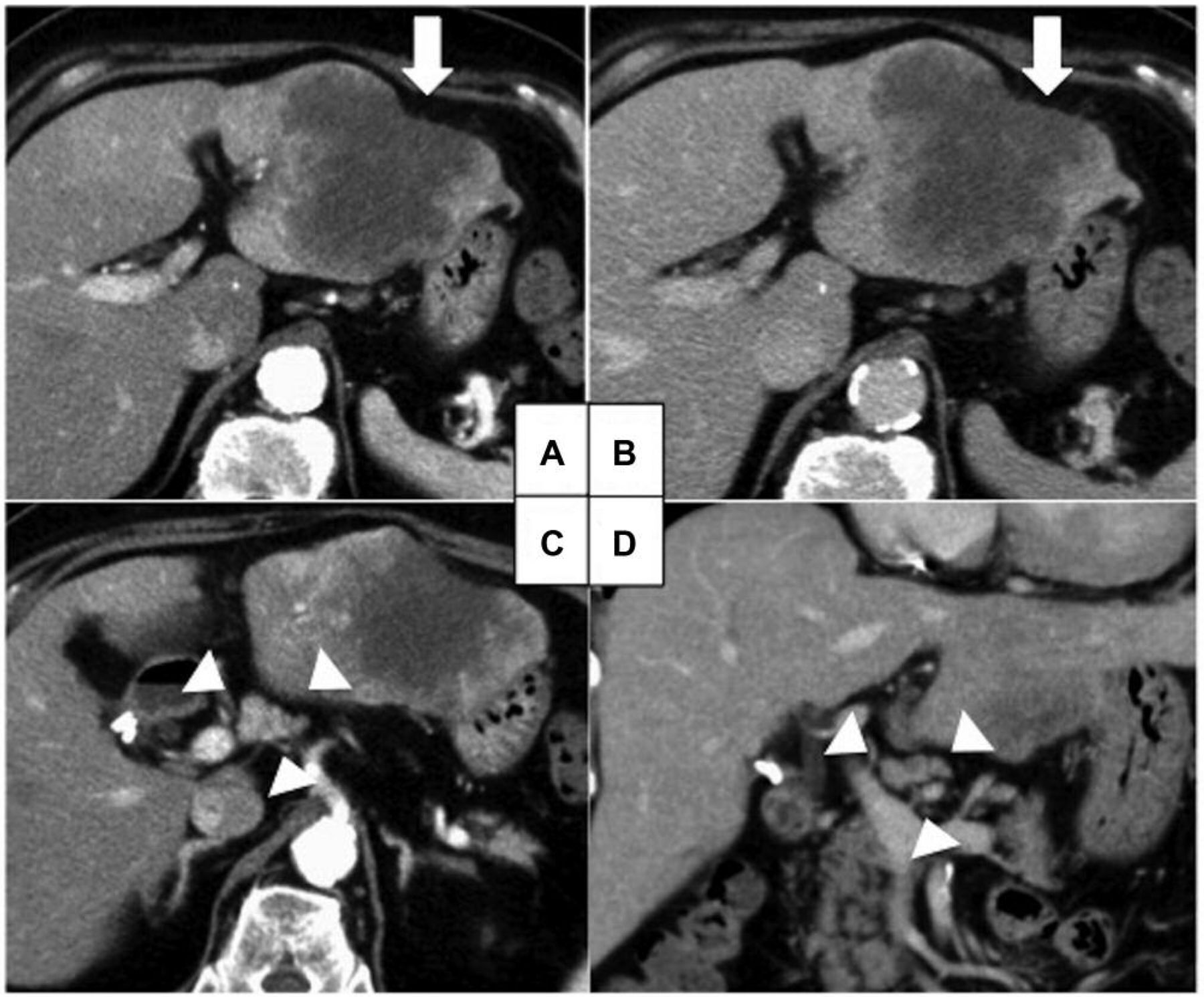
Contrast-enhanced computed tomography images of the cHCC-CC. cHCC-CC was located in left lateral section (arrows). The tumor was gradually enhanced from the periphery to the inner tumor area, from the arterial to the portal vein phase; however, the tumor core showed no enhancement (A, B). Bulky lymph node metastasis was observed in the hepatoduodenal ligament (arrowhead) (C, D).
Regarding surgical strategy, the plan was to perform a left hepatectomy and extrahepatic bile duct resection, in case that radical resection was possible. Otherwise, we planned to perform only a left lateral sectionectomy and chemoradiotherapy (CRT) for lymph node metastasis as soon as possible after the operation. In laparotomy, there was a small amount of ascites; however, cytological diagnosis showed no malignant cells. Peritoneal dissemination was also not detected. The tumor was found on the surface of the left lateral section with greatly enlarged lymph nodes along the lesser curvature of the stomach (#3), the #8, and the #12. Intraoperative ultrasonography examination confirmed a small part of tumor invasion into the umbilical portion, and subsequently, a left lateral sectionectomy without lymph node dissection was performed (Figure 2A and B). The pathological examination revealed that the tumor contained both moderately to poorly differentiated HCC, and well to moderately differentiated CC (Figure 2C and D) with invasion of the second branch of the portal vein (vp2) and the major hepatic vein branch (vv2). No cancer cells were detected in the resection stump of the left hepatic vein. After palliative hepatectomy with macroscopic cancer remnant (R2), the patient recovered steadily and was discharged at 9 days post-operation without any complications.
The patient was re-hospitalized 3 weeks post-operation to undergo hepatic arterial infusion (HAI) chemotherapy with cisplatin (CDDP) at a dose of 75 mg, fluorouracil (5-FU) at a dose of 750 mg, and mitomycin C (MMC) at a dose of 2 mg, due to pathological findings of microvascular invasion. In addition, we performed CRT for the remaining enlarged abdominal lymph nodes after HAI as follows: a total dose of 45 Gy in 15 fractions and 400 mg/day of oral tegafur-uracil (UFT-E combination granule). After discharge from our department, blood tests were conducted once every 2 or 3 months, and CT was performed twice per year. After all, the administration of UFT-E had started as a part of CRT and continued for 10 years as maintenance chemotherapy. Serum CA19-9 levels normalized after hepatectomy, HAI chemotherapy, and CRT. Surprisingly, the patient is still alive without any relapse during the12-year follow-up period (Figure 3).

Macroscopic and pathological findings. The tumor was whitish with a clear border and bulged on the surface of the liver (A, B). Hematoxylin and eosin staining revealed characteristic microscopic features of both HCC (C) and CC (D). Scale bar=100 μm.
Discussion
cHCC-CC is a rare primary liver cancer with poor prognosis (1, 3, 4). In a study of 26 cHCC-C it was reported that the 5-year survival rate and mean survival time of them were 11.5% and 1.8 years, respectively (9). Moreover, cHCC-CC tumors were significantly more invasive to the portal vein than the HCC tumors; however, they were comparable to the CC (9). Although surgical resection is the best way to improve patient prognosis, the effectiveness of surgical resection alone is limited because of high rate of recurrence (10). High serum CA19-9 level, large tumor size, vascular invasion, lymph node metastasis, and satellite lesions are reported as poor prognostic factors in cHCC-CC following hepatectomy (11-13). Therefore, to improve patient prognosis, not only liver resection but also additional therapies should be considered for cHCC-CC patients with poor prognosis.
HAI is an effective therapy following hepatectomy in liver cancers. Nitta et al. suggested that HAI for HCC patients with vascular invasion might reduce the risk of recurrence (14). Boehm et al. also showed that HAI treatment was more effective than transcatheter arterial chemoembolization (TACE), drug-eluting bead TACE (DEB-TACE), and yttrium-90 radioembolization (Y-90) for unresectable ICC (15). Although the usefulness of HAI in cHCC-CC treatment is still unclear, based on previous reports, it should be considered as a therapeutic option following hepatectomy for advanced cHCC-CC. The present case had vascular invasion such as vp2 and vv2; therefore, we decided to perform HAI with IA call and 5-FU.

Change of CA19-9 during multidisciplinary therapy. CA19-9 rapidly decreased after hepatectomy, and further decreased after hepatic arterial infusion and irradiation. Furthermore, it is maintained within the normal range by UFT oral administration for 10 years. UFT, Tegafur-uracil; CA 19-9, carbohydrate antigen 19-9; HAI, hepatic arterial infusion; RT, radiotherapy; CDDP, cisplatin; 5-FU, fluorouracil; MMC, mitomycin.
The post-hepatectomy prognosis of cHCC-CC patients with lymph node metastasis is quite poor (13). As in CC, the effect of lymph node dissection for cHCC-CC still remains unclear (2). Because the present case also had bulky lymph node metastasis, we could easily predict a macroscopic remnant tumor after lymph node dissection. Therefore, we did not perform lymph node dissection and planed to perform local treatment with postoperative radiotherapy (RT). In fact, the efficacy of CRT in cHCC-CC with lymph node metastasis, has already been reported. Hayashi et al. presented a patient who survived 42 months disease-free after adjuvant chemotherapy (UFT) and RT following hepatectomy (6). For unresectable ICC, in a study with 2,842 patients, CRT was reported to prolong patient survival significantly longer than chemotherapy alone (16). Some studies have shown that CRT induces anticancer immunity by CD8 positive T cells in both the tumor (17) and the stroma (18). In addition, RT has been associated with a number of anti-tumor mechanisms such as (i) improved antigen cross-presentation, (ii) increased Type I interferon release, and (iii) enhanced major histocompatibility complex (MHC) class I expression on tumor cells (19, 20). Therefore, as a treatment strategy of cHCC-CC with massive lymph node metastasis like the present case, CRT after palliative hepatectomy may be considered an effective treatment option.
A standard systemic chemotherapy regimen has not yet been established for unresectable cHCC-CCs, while the effect of systemic chemotherapy remains unclear with unfavorable outcomes (21, 22). In a retrospective analysis of 7 patients, Rogers et al. showed that disease control was achieved in 3 patients who received gemcitabine plus platinum with or without bevacizumab as the first or second line of treatment (22). A recent multicenter retrospective analysis involving 36 patients showed the efficacy of platinum-containing regimens (23). These results suggest that platinum-containing regimens seem to be more effective than other available treatments. There have also been reports on the utility of UFT in advanced liver cancer (6, 7, 24). In the present case, we referred to the literature and selected UFT by oral administration. Several reports on systemic chemotherapy for cHCC-CC suggest that it can be efficacious when used alone; however, prospective trials are needed to identify a standard of care for unresectable cHCC-CCs.
In conclusion, we experienced a case of cHCC-CC with bulky hilar lymph node metastasis who survived for 12 years without relapse. The multidisciplinary treatment consists of left lateral sectionectomy and HAI for liver tumor in combination with CRT for lymph node metastasis followed by UFT administration as maintenance adjuvant chemotherapy. We suggest this treatment strategy as an option to improve prognosis in patients with advanced cHCC-CCs.
Footnotes
Authors' Contributions
Conception and design: T. Miyata, T. Beppu; Acquisition of data: T. Miyata, Y. Imamura, T. Beppu; Writing, review, and/or revision of the manuscript: All authors; Supervision: Hideo Baba.
Compliance with Ethical Standards
Informed consent was obtained from the patient.
Conflicts of Interest
The Authors declare that they have no conflict of interest.
- Received February 18, 2019.
- Revision received March 20, 2019.
- Accepted March 20, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.