


Abstract
In order to evaluate affected axillary lymph nodes in breast cancer by positron-emission tomography using 18F-fluorodeoxyglucose (FDG-PET), an understanding of FDG avidity is important. In the present study, we examined whether certain factors, including lymphatic spread and size of metastatic lymph nodes, were associated with FDG avidity in order to evaluate the benefits of a FDG-PET assessment of axillary node metastases. We retrospectively investigated the cases of 179 consecutive patients with primary breast cancer who underwent FDG-PET preoperatively. Among the 179 patients, 48 (26.8%) had axillary lymph node metastases. The sensitivity, specificity, overall accuracy, and false-negative rates in the diagnosis of axillary lymph node status by FDG-PET were 47.9%, 98.5%, 84.9%, and 52.1%, respectively. The 48 cases with lymph node metastases were divided into two groups based on the presence or not of FDG uptake in the axillary lesions. Clinicopathological features of the primary tumor, including tumor size, standardized uptake value (SUVmax and biomarkers, were not statistically significant factors; only the clinicopathological features of metastatic lymph nodes, including the size of node metastasis, were significantly associated with FDG uptake in the axillary lymph nodes. Among the eight cases of micrometastasis, seven were not detected by FDG-PET. The number of cases with only one affected node was significantly higher in the group without FDG uptake in the axillary lesion. Although the number of lymph node metastases was relatively higher in the FDG-PET-positive patients, the difference was not statistically significant. FDG-PET may help identify patients with high axillary lymph node burden. Our findings imply that preoperative FDG-PET evaluation of lymph nodes is not sufficient to predict lymphatic spread or micrometastasis because FDG avidity is mainly influenced by the size of the tumor.
Axillary lymph node dissection (ALND) is important for disease control and staging for breast cancer; however, ALND carries the risk of complications such as lymph edema. Sentinel lymph node biopsy (SLNB) has been developed as a minimally invasive operative procedure to precisely determine the presence of axillary lymph node metastases in patients with clinically-negative nodes (1-6). The recent results of the American College of Surgeons Oncology Group Z0011 trial suggested that some women would be safe from recurrence without further axillary treatment if they have fewer than three involved sentinel nodes with no extracapsular spread (7). It may be possible to avoid unnecessary ALND in selected patients. Thus, preoperative axillary lymph node evaluation is considered to be critical.
In recent years, the clinical applications of positron-emission tomography (PET) have undergone explosive growth. PET using 18F-fluorodeoxyglucose (FDG) is a non-invasive whole-body imaging technique used to evaluate various kinds of malignancies, including breast cancer, for tumor staging and re-staging, the detection of recurrence, and monitoring treatment responses (8-11). FDG-PET has been evaluated for its accuracy in the axillary staging of operable primary breast cancer (11-14). These studies have sometimes provided conflicting results, either supporting the possibility of using FDG-PET to select patients who need axillary dissection or questioning whether FDG-PET can accurately assess the axillary status in patients with breast cancer (12, 13). In evaluation of axillary lymph node metastases in patients with breast cancer, FDG-PET is less sensitive (20% to 60%) but more specific (65% to 100%) than other modalities (12, 13). In certain cases with affected lymph nodes, FDG uptake was not detected. For the evaluation of affected axillary lymph nodes in breast cancer by FDG-PET, an understanding of FDG avidity is important. However, there have been relatively few studies assessing the factors associated with FDG avidity of affected axillary lymph nodes. In the present study, we evaluated the usefulness of FDG-PET in detecting metastatic axillary lymph nodes in patients with primary breast cancer. Furthermore, to evaluate the assessment of axillary lymph node metastases provided by FDG-PET, we examined whether certain clinical factors, including lymphatic spread of lymph nodes and the size of lymph node metastases, were associated with FDG avidity.
The sensitivity, specificity, overall accuracy, and false-negative rates in the diagnosis of axillary lymph node status by positron-emission tomography–computed tomography.
Patients and Methods
We retrospectively investigated the cases of 179 consecutive patients with primary breast cancer who underwent FDG-PET preoperatively at the Department of General Surgical Science, Gunma University, Japan, from January 2010 to February 2015. All patients had undergone radical breast surgery. Patients with previously diagnosed breast cancer or incomplete clinical information were excluded, as were male patients. Among the 179 patients, 48 (26.8%) had axillary lymph node metastases. In all 48 cases, the presence of lymph node metastasis was confirmed pathologically. None of the patients had received preoperative chemotherapy. Patients underwent FDG-PET/computed tomography as part of the routine standard-of-care, and no changes to the standard-of-care were made. The maximum standardized uptake value (SUVmax) of primary tumors was calculated in a routine clinical fashion. Informed consent was obtained from all patients.
The details extracted from the hospital database were age, histological type, primary tumor size, lymphatic and vascular invasion, estrogen (ER) and progesterone (PgR) receptor expression status, human epidermal growth factor receptor 2 (HER2) score of the primary tumor, SUVmax of the primary tumor, axillary lymph node status, and visibility of detected lesion(s) by FDG-PET. The ER and PgR status were assessed by ALLRED scores, and an ALLRED score of 3 or higher was defined as ER- and PgR-positive (15, 16).
Statistical analysis. The breast cancer cases with node metastasis were divided into two groups on the basis of the presence or not of FDG uptake in the axillary lesion. We conducted a univariate statistical analysis using Fisher's exact test or the χ2 test with Yates' correction. To compare the two groups, we used Student's t-test. Differences were considered significant when p<0.05.
Results
In total, 179 cases were included in the analysis. In 48 patients (26.8%), the presence of lymph node metastases was diagnosed by histological examination with standard hematoxylin and eosin staining. Among the 48 cases with nodal metastases, eight cases (16.7%) had micrometastases. As shown in Table I, the sensitivity, specificity, overall accuracy, and false-negative rates in the diagnosis of axillary lymph node status by FDG-PET were 47.9%, 98.5%, 84.9%, and 52.1%, respectively. The false-positive rate of FDG-PET evaluation was 1.5%. The mean SUVmax of metastatic lymph nodes was 4.53 (range=0-23.5) overall. The 48 cases with lymph node metastasis were divided into two groups based on the presence or not of FDG uptake in the axillary lesions (Figure 1). Table II shows the patient characteristics and summarizes the results of the univariate analysis conducted to determine the relationship between the clinicopathological variables and FDG uptake in the axillary lesions. As can be seen, none of the clinicopathological features of the primary tumor, including primary tumor size, SUVmax and biomarkers, were significantly associated with FDG uptake. The present analysis revealed that only the clinicopathological features of the metastatic lymph node were significantly associated with FDG uptake in the axillary lymph nodes. The analysis revealed that the size of the nodal metastasis was a statistically significant factor. Out of the eight cases with lymph node micrometastasis, seven (87.5%) were not detected by FDG-PET (Figure 1A). Although the number of lymph node metastases was relatively higher in FDG-PET-positive patients, the difference was not statistically significant. The number of cases with only one metastatic lymph node was significantly higher in the group without FDG uptake in the lymph nodes. The number of cases with lymph node metastases in 1-3 nodes was also significantly higher in the group without FDG uptake in the lymph nodes.
Patient characteristics and clinicopathological features associated with 18F-fluorodeoxyglucose uptake in axillary lymph nodes.

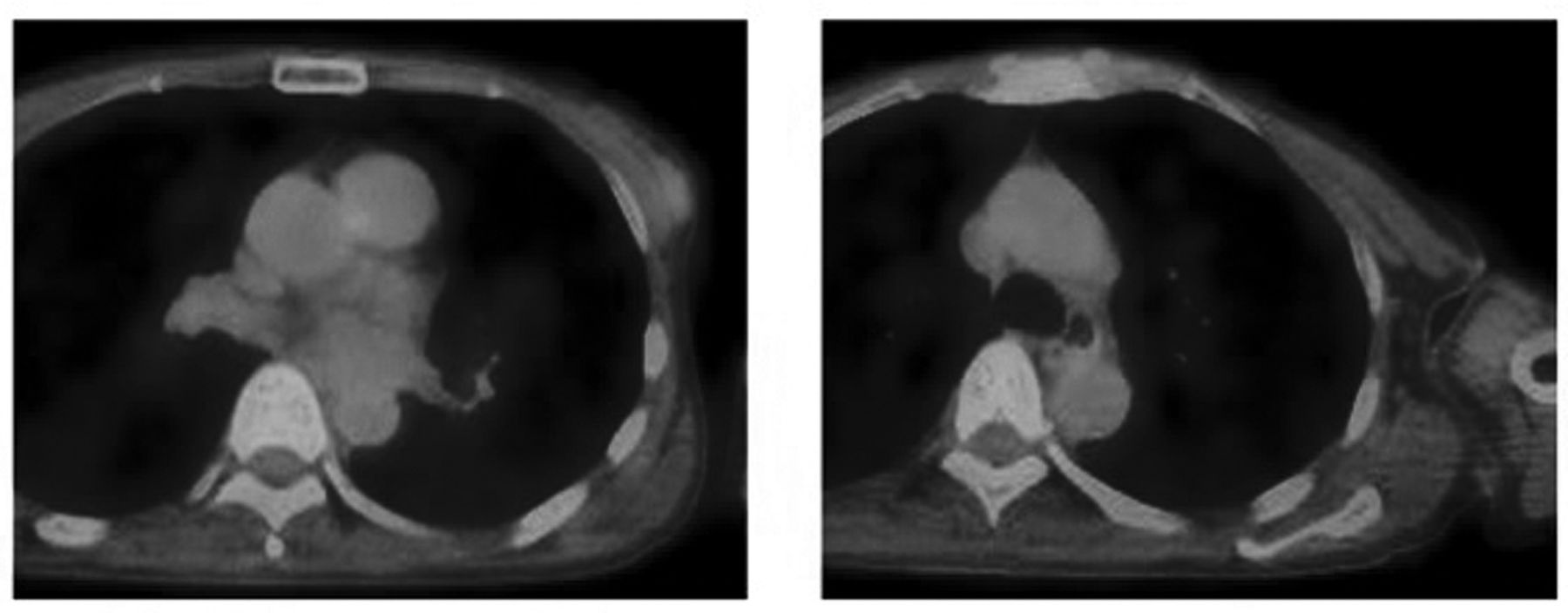
a: Examples of absence of 18F-fluorodeoxyglucose (FDG) uptake in lymph node on positron-emission tomography–computed tomography (PET-CT) in an 83-year-old female. There was FDG uptake in the primary tumor [maximum standardized uptake value (SUVmax) 5.98] but not in lymph nodes. Micrometastasis of lymph node was confirmed histopathologically. b: Examples of FDG uptake in lymph nodes on PET-CT in a 69-year-old female. The SUVmax was 2.96 in the primary tumor and 1.70 in the lymph node. Fifteen lymph node metastases were confirmed histopathologically.

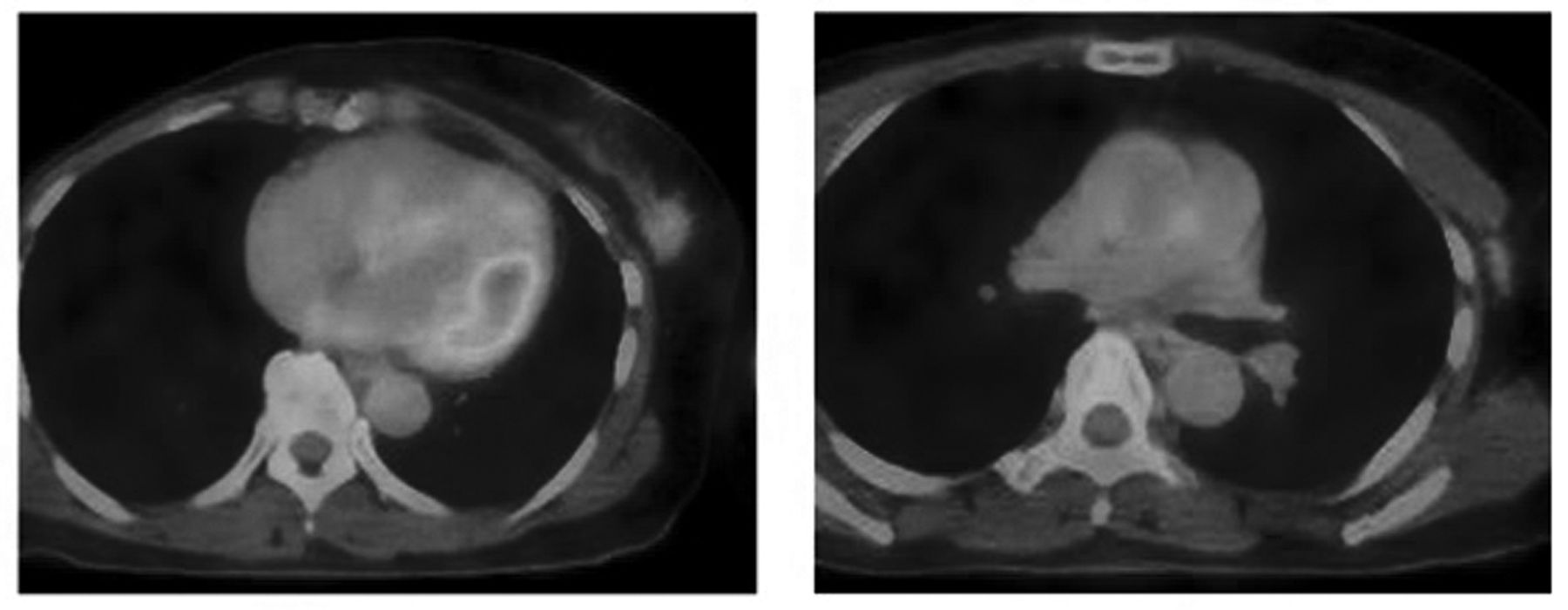
Case of positive 18F-fluorodeoxyglucose uptake in lymph node on positron-emission tomography–computed tomography in a 64-year-old female who had one lymph node metastasis. The maximum standardized uptake value was 2.3 in the primary tumor and 1.7 in the lymph node. Only one lymph node metastasis (17 mm) was confirmed histopathologically.
Case of negative 18F-fluorodeoxyglucose uptake in lymph node on positron-emission tomography–computed tomography in a 54-year-old female who had axillary lymphatic spread. The SUVmax in the primary tumor was 1.51. Seven lymph node metastases (3 mm) were confirmed histopathologically.
Discussion
FDG-PET has been widely used for diagnosing staging and recurrence in various types of cancer; however, its diagnostic utility for cancer is controversial (8-11). Regarding breast cancer, there are many reports of preoperative evaluation with FDG-PET. FDG-PET can differentiate breast cancer from benign lesions with a sensitivity of 66-96% and a specificity of 83-100% (17). In our previous study, the overall sensitivity for detection of all breast cancer was 91.5% (Fujii T, et al. manuscript in submission). The critical role of FDG-PET in evaluating axillary nodal status for initial staging of breast cancer has not yet been well-defined in clinical practice. FDG-PET has high specificity but mediocre sensitivity for identifying axillary lymph node metastases in breast cancer. In our series, positive FDG uptake was a good predictor of axillary disease. However, there have been few studies to assess the factors associated with FDG avidity of affected lymph nodes in breast cancer. Thus, the present study was undertaken to assess the additional benefit of FDG-PET evaluation of lymph node metastases for patients with breast cancer. FDG-PET may help identify patients with high axillary lymph node burden; thus, we evaluated the hypothesis that the FDG avidity of lymph nodes was associated with axillary lymphatic metastatic spread, and evaluated whether FDG-PET could be useful for predicting lymphatic spread. There was a significant correlation between FDG uptake and the size of lymph node metastases; however, the number of lymph node metastases was not correlated with FDG uptake. On the other hand, the number of nodal metastases did not correlate with FDG uptake, however, the numbers of cases with only one lymph node metastasis or 1-3 nodes were significantly higher in the group without FDG uptake in the lymph nodes. These findings reflect the fact that FDG uptake in lymph nodes may be determined mainly by high tumor burden or tumor size. Several studies have reported that FDG uptake correlates with the size of tumor to a certain level according to the resolution of the PET scanner, known as the partial volume effect (18). Tumor size was associated with lymphatic invasion, which may reflect lymphatic spread, but because the size of tumor is the main factor affecting nodal FDG uptake, the number of nodal metastases may fall short of reaching a statistically significant association. In some cases, FDG uptake was detected in the axillary lesion, but there was only one metastatic lymph node metastasis (Figure 2). In other cases, there was marked lymphatic spread regardless of the small size of the metastases (Figure 3). The size of lymph node metastases does not always reflect lymphatic spread. Thus, the FDG-PET evaluation was not sufficient for evaluation of axillary lymphatic spread, suggesting that ALND cannot be avoided, even in cases with negative FDG uptake in axillary lesions by FDG-PET.
In the current series, eight cases had lymph node micrometastasis but seven of them (87.5%) were not detected by FDG-PET (Figure 1A). Nodal FDG uptake may be determined by the size of tumor, and FDG-PET evaluation of lymph node metastasis is not predictive of small metastases or micrometastases. In the current study, the false-positive rate of FDG-PET evaluation of lymph node metastases was only 1.5%. Our findings imply that macrometastasis of lymph nodes can be detected by FDG-PET, and in cases with FDG uptake in lymph nodes, lymph node metastasis may be highly suspected. Therefore, it may be useful for avoiding SLNB in cases with positive FDG uptake in the axillary lesion.
FDG-PET measures glucose metabolism, which reflects the biological aggressiveness of cancer. FDG-PET could provide biological information about the tumor growth potential. In fact, among the 48 patients with positive nodes, three had recurrent disease, and all three cases were in the FDG-positive group. It is interesting to note that FDG uptake in the axillary lesion was not correlated with clinicopathological features of the primary tumor. Statistical significance was only detected in characteristics of axillary lymph node status. These findings may imply the possibility that recurrent disease was caused not only by the primary tumor but also by regional lymph node metastasis, at least in part. This possibility should be investigated in further studies.
This study has several potential limitations, the major ones being that it was a retrospective analysis and the number of cases was relatively small. Additional research is needed to explore other benefits and drawbacks of FDG-PET evaluation of lymph node metastases.
In conclusion, we demonstrated that preoperative FDG-PET evaluation of lymph nodes is effective in predicting macroscopic nodal status but is less effective in predicting nodal metastatic spread. The positive predictive value is high, but our findings imply that preoperative FDG-PET evaluation of lymph nodes is not sufficient to predict lymphatic spread or micrometastasis. Therefore, positive FDG uptake in axillary lesions may be useful for avoiding SLNB, but evaluation of axillary lesions by FDG-PET cannot replace SLNB or ALND due to its unsatisfactory sensitivity.
Acknowledgements
The Authors would like to thank Saitoh Y, Yano T, Matsui Y, Ishida A and Ishikubo A for their secretarial assistance.
Footnotes
Competing Interest Statement
The Authors declare that they have no competing financial interests.
- Received October 19, 2015.
- Revision received November 16, 2015.
- Accepted November 23, 2015.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Relationship Between FDG Uptake and the Platelet/lymphocyte Ratio in Patients With Breast Invasive Ductal Cancer
- Relationship Between FDG Uptake and Neutrophil/Lymphocyte Ratio in Patients with Invasive Ductal Breast Cancer
- Clinicopathological Features of Ductal Carcinoma In Situ from 18F-FDG-PET Findings
- Clinical Significance of 18F-FDG-PET in Invasive Lobular Carcinoma
- Clinicopathological Features of Cases with Primary Breast Cancer not Identified by 18F-FDG-PET
- Prediction of Extracapsular Invasion at Metastatic Sentinel Nodes and Non-sentinel Lymph Nodal Metastases by FDG-PET in Cases with Breast Cancer