


Abstract
Background: Wnt/β-catenin signaling plays an important role in colorectal cancer (CRC). Wnt has many sub-types and it is uncertain which of them affect progression of CRC. Patients and Methods: We analysed 201 patients who underwent curative surgery for CRC. We investigated the relationship between the expression of Wnt and β-catenin proteins and prognosis using immunohistochemistry. Results: The high expression of Wnt1 correlated with high expression of nuclear and cytoplasmic β-catenin (p=0.0004, p=0.02). The high expression of Wnt5a also correlated with high expression of membrane β-catenin (p=0.03). In multivariate analysis, lymph node metastasis (p=0.046) and high expression of nuclear β-catenin (p=0.04) were independent prognostic factors for survival. Conclusion: The expression of nuclear β-catenin is a useful predictive marker in CRC. It is suggested that Wnt1 may be the main activator of the β-catenin signaling pathway and that Wnt5a may stabilize adherens junctions, thereby suppressing the epithelial-mesenchymal transition.
Colorectal cancer (CRC) is one of the most common types of cancer in the world (1). Treatments for CRC have evolved remarkably; however, patients often have recurrence after curative surgery. It is important to predict the postoperative prognosis and choose for appropriate adjuvant therapy, especially in Stage II or III CRC. Although various clinicopathological factors, including preoperative tumor markers and tumor-node-metastasis (TNM) factors, have been reported as prognostic factors, it is not easy to identify patients with high risk of recurrence. Recently, there has been a focus on molecular markers as predictive prognostic markers in CRC (2). The wingless-type mouse mammary tumor virus integration site family (Wnt) signaling pathway, which plays an important role in maintaining normal cell homeostasis and embryonic development, is known to be associated with CRC progression. (3) Wnt proteins are secreted glycoproteins and the ligands of the Wnt signaling pathway. Wnt proteins bind to Frizzled (Fz) receptors, which are seven-pass transmembrane receptors, and activate an intracellular signaling cascade, thereby affecting various cellular functions, including cell motility, polarity and proliferation (4-6). There are many reports showing that aberrant Wnt signaling pathway activation is associated with the progression of various cancers and autoimmune diseases (7). There are three different Wnt signaling pathways: (i) the β-catenin pathway, (ii) the calcium-dependent pathway and (iii) the planar cell polarity (PCP) pathway. The three Wnt signaling pathways are further divided into canonical and non-canonical signaling pathways (8, 9). The β-catenin pathway, which belongs to the canonical pathway, promotes cell growth and proliferation. The calcium-dependent and PCP pathways, which are non-canonical pathways, govern cell motility and polarity. Fz has ten sub-types and Wnt has nineteen sub-types that share genetic structural homology with each other (10). Individual Wnt ligands and Fz receptors can activate either canonical or non-canonical pathways in different diseases (5). Therefore, Wnt signaling pathways are very complicated. In the present study, we focused on the β-catenin pathway. In the absence of Wnt ligands, free intra-cytoplasmic β-catenin is phosphorylated by a protein complex consisting of adenomatous polyposis coli, glycogen synthase kinase-3β and casein kinase I. Phosphorylated β-catenin is subsequently ubiquitinated by the ubiquitin ligase β-transducing-repeat-containing protein and degraded in the proteasome, thus keeping intra-cytoplasmic β-catenin levels very low. However, binding of the Wnt ligand to the complex receptor formed by Fz and low-density lipoprotein (LDL) receptor-related protein 5 and 6 inactivates the complex phosphorylating intra-cytoplasmic β-catenin. In this manner, intra-cytoplasmic β-catenin avoids degradation by the proteasome, is stabilized and enters the nucleus. There, nuclear β-catenin along with T-cell factor/lymphoid enhancer factor (TCF/LEF) causes aberrant expression of genes responsible for cell-cycle regulation and cell proliferation, such as cyclin D1 (CCND1), matrix metalloproteinase 7 (MMP7), c-MYC, and survivin (BIRC5) (11). β-catenin is a multi-functional protein that plays key roles in the Wnt/β-catenin signaling pathway and in cellular adherens junctions along with E-cadherin. The destruction of adherens junctions affects tumor invasion or epithelial-mesenchymal transition (EMT), which is associated with metastasis (12). Many authors reported that Wnt/β-catenin signaling plays an important role in the initiation and progression of CRC; however, because of the complexity of the Wnt signaling pathway, it is unclear which Wnt ligand sub-types affect the progression of CRC (13, 14). The aim of the study was to investigate the correlation between Wnt proteins and β-catenin expression levels and CRC prognosis using tissue microarray sample immunohistochemistry.
Patients and Methods
Patients. This study included 201 patients with Stage II or III CRC based on the Japanese Classification of Colorectal Carcinoma (second English edition) who underwent curative resection for the first time at the Kurume University Hospital between April 2007 and December 2009 (15). None of the patients had distant organ metastasis. Clinical records and pathological reports were reviewed retrospectively. All the samples were obtained after the patients signed the informed consent form. This study was approved by the Institutional Review Board of Kurume University (No. 203). The clinicopathological findings were diagnosed based on the Japanese Classification of Colorectal Cancer.
Tissue microarray. Paraffin blocks containing formalin-fixed primary tumors were obtained from all patients. In each case, a core biopsy 3.0 mm in diameter was taken from the center of the tumor in the paraffin blocks using a tissue microarray instrument. Tissue cores from each specimen were assembled on recipient paraffin blocks and embedded.
Immunohistochemistry of the tissue microarray. We performed immunohistochemical staining on 4-μm-thick sections of the tissue microarray blocks. Paraffin sections were de-paraffinized in xylene and rehydrated in graded ethanol. Microwave-induced antigen retrieval was performed in 0.01 M citrate buffer, pH 6.0. Endogenous peroxidase activity was blocked using 0.3% hydrogen peroxide in methanol for 15 min. Sections were incubated at room temperature with the following primary antibodies at the specified dilutions: anti-Wnt1 (dilution 1:800, ab91191; Abcam, Cambridge, UK), anti-Wnt3 (dilution 1:400, LS-C175701; LSBio, Seattle, WA, USA), anti-Wnt5a (dilution 1:1000, ab86720; Abcam), anti-Wnt8a (dilution 1:100, ab67350; Abcam) and anti-β-catenin (dilution 1:100, #8480; Cell Signaling Technology, Danvers, MA, USA). Immunohistochemical staining was performed using the DAKO ChemMate™ EnVision™ Kit system (DAKO, Glostrup, Denmark) and a Peroxidase/DAB Kit (DAKO). Sections were counterstained with haematoxylin, dehydrated and mounted.
Statistical analysis. The chi-squared test was used to evaluate the significant correlation between the expressions of the studied proteins. Survival curves were computed using the Kaplan-Meier method and statistical significance was assessed with a log-rank test. Overall survival (OS) and disease-free survival (DFS) were defined as the time period extending from the operation to the date of death or recurrence. Univariate and multivariate analyses were performed using the Cox proportional-hazard model. All statistical analyses were performed using JMP, version 11.0, and a p-value under 0.05 was considered statistically significant.
Results
Patients' characteristics and protein expression levels. The patients' clinicopathological characteristics are summarized in Table I. Furthermore, 97 patients (48.3%) were categorized as having Stage II disease and 104 patients (51.7%) were categorized as having Stage III disease. The majority of patients had T4 tumors with lymphatic and venous invasion. Moreover, 79 patients (39.3%) had received adjuvant chemotherapy after curative surgery. The Japanese Society for Cancer of the Colon and Rectum guidelines (2014) for the treatment of colorectal cancer recommend postoperative adjuvant chemotherapy for patients with Stage III disease and those at high-risk (with clinical characteristics, such as T4 tumors, perforation, poorly differentiated or signet ring tumor types and vascular or lymphatic invasion), as well as for patients with Stage II disease who have sufficient physical strength to receive chemotherapy (16).
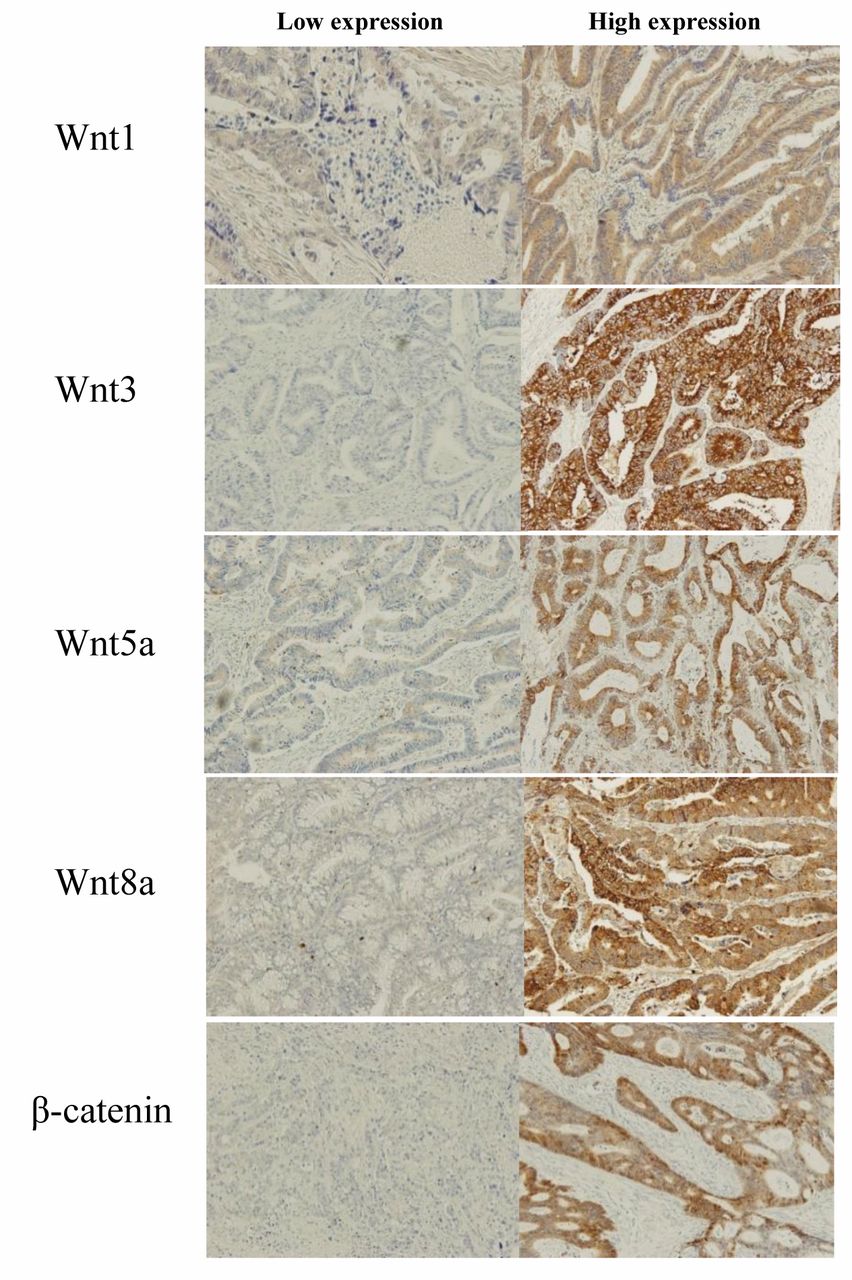
Immunohistochemical marker staining. Representative immunohistochemical marker stainings are shown in Figure 1. Wnt proteins were mainly localized to the cytoplasm and low expression levels of the proteins were also detected in the nucleus and membrane of normal and tumor cells. On the other hand, β-catenin was detected in the membrane, nucleus and cytoplasm of tumor cells, although it was detected mainly in the membrane of normal cells. Therefore, we evaluated expression levels of Wnt proteins in the cytoplasm only and those of β-catenin in the nucleus, cytoplasm and membrane, respectively. Wnt proteins and β-catenin were expressed in more than 50% of the investigated cases. The staining intensity was categorized into high- or low-expression groups (Figure 2). In each case, the staining grade was scored as an average throughout the spot.
Incidence of Wnt and β-catenin. In order to investigate which subtype of Wnt proteins affect Wnt/β-catenin signal pathway, the correlation between expression of each Wnt protein and nuclear β-catenin expression was analyzed using a Chi-squared test. The high expression of Wnt1 protein was strongly correlated with the high expression of nuclear (p=0.0004) and cytoplasmic (p=0.02) β-catenin. The high expression of Wnt5a protein was correlated with high expression levels of membrane β-catenin (p=0.03). The expression of Wnt3 and Wnt8a proteins did not correlate with the expression of β-catenin (Table II).
Clinicopathological characteristics of patients (n=201).
The expression of nuclear β-catenin was significantly correlated with poor prognosis. Analysis for DFS showed that tumor location (p=0.03), tumor depth (p=0.0003), tumor differentiation (p=0.002), adjuvant chemotherapy (p=0.0007), high expression of Wnt1 (p=0.047), low expression of Wnt5a (p=0.04) and high expression of nuclear β-catenin (p=0.008) were all prognostic factors for shortened DFS. In multivariate analysis, tumor depth (95% confidence interval (CI)=1.8-8.6; p=0.0003), tumor differentiation (95% CI=1.0–3.6; p=0.046), adjuvant chemotherapy (95% CI=1.4-4.8; p=0.001), low Wnt5a expression (95% CI=0.3-1.0; p=0.02) and high nuclear β-catenin expression levels (95% CI=1.1-3.9; p=0.02) were all found to be independent predictors for DFS (Table III). In the univariate analysis of OS, tumor depth (p=0.03), lymph node metastasis (p=0.004), lymphatic invasion (p=0.03), venous invasion (p=0.03), high Wnt1 protein expression levels (p=0.045) and high nuclear β-catenin expression levels (p=0.01) were all predictive factors for OS. In multivariate analysis, lymph node metastases (95% CI=1.0-3.8; p=0.0046) and high expression of nuclear β-catenin (95% CI=1.0–3.4; p=0.04) were independent prognostic factors for shortened survival (Table IV). Tumor depth (p=0.11), lymphatic invasion (p=0.61), venous invasion (p=0.68) and high Wnt1 protein expression (p=0.17) were excluded as confounders in multivariate analysis. The high expression of nuclear β-catenin was the only predictive factor for both OS and DFS (Figure 3). However, the expression levels of nuclear β-catenin were not correlated with any clinicopathological factors, such as age, tumor location and tumor differentiation.
Correlation between Wnt protein expression and β-catenin expression in colorectal cancer.
Discussion
This study investigated the expression of several Wnt proteins and the correlation between Wnt proteins and nuclear β-catenin in CRC. We confirmed that high expression levels of nuclear β-catenin were associated with poor prognosis. We also found that Wnt1 protein might play an important role in the progression of the CRC by activating the β-catenin signaling pathway and that Wnt5a might play a role in the stabilization of adherens junctions to suppress EMT.
Based on previous reports, we hypothesized that high expression levels of the Wnt1, 3 and 8a proteins, which are considered to be activators of the β-catenin pathway, are related to poor prognosis (17). In contrast, we hypothesized that increased expression of Wnt5a, which is known to inhibit the β-catenin pathway and to activate non-canonical pathways, is related to good prognosis (17, 18). Understanding which Wnt proteins are most effective in regulating β-catenin signaling pathways could help predict the prognosis of patients with CRC, establish postoperative adjuvant chemotherapy strategies and develop new molecular treatments targeting Wnt proteins.

Immunohistochemical staining for Wnt1, 3, 5a, 8a and β-catenin proteins. Wnt proteins were mainly localized to the cytoplasm with low expression levels in the nucleus and membrane of normal and tumor cells. β-catenin was detected in the membrane, nucleus and cytoplasm of tumor cells. Original magnification ×400.
β-catenin is a multi-functional protein that plays key roles in the Wnt/β-catenin signaling pathway and in cellular adherens junctions. Elevated expression of nuclear β-catenin is considered a sign of aberrant β-catenin signaling pathway activation and is thought to promote tumor progression. Recently, Myung et al. reported that increased levels of nuclear β-catenin were correlated with poor prognosis in CRC (3). The destruction of cell adherens junctions is considered to affect tumor invasion or EMT, which is related to metastasis. Stanczak et al. reported that the destruction of adherens junctions have an impact on the invasiveness of CRC (1). From all proteins investigated in this study, nuclear β-catenin aberrant expression was the only independent prognostic factor for both shortened survival and recurrence. However, the mechanisms by which the β-catenin signaling pathway promotes carcinogenesis and the progression of CRC are still not clearly elucidated.
The present study shows that Wnt1 protein expression is strongly correlated with high expression of nuclear β-catenin. This suggests that Wnt1 protein is a key ligand that activates the β-catenin signaling pathway during the progression of CRC. Wnt1 protein was correlated with an unfavourable phenotype and a poorer prognosis in various types of human cancers, such as those of the lung, oesophagus and stomach (19). Indeed, Xu et al. reported a significant correlation between the expression levels of Wnt1 and β-catenin proteins in lung cancer (20). In addition, Huang et al. reported that elevated expression of Wnt1 protein was a significant factor in the poor prognosis of non-small cell lung cancer. Mizushima et al. showed that Wnt1 could stimulate the β-catenin pathway in oesophageal squamous cell carcinoma (21). Furthermore, Lv et al. reported that Wnt1 played an important role in progression of oesophageal squamous cell carcinoma (22, 23). Mao et al. demonstrated that Wnt1 accelerated the proliferation of gastric cancer stem cells (24). The expression of Wnt5a was correlated with an increased DFS in our univariate analysis. Wnt5a is known to inhibit the β-catenin signaling pathway and to activate non-canonical pathways. Moreover, Wnt5a is thought to stabilize adherens junctions with β-catenin and E-cadherin components and to inhibit tumor invasion or metastasis (18, 25). We hypothesized that Wnt5a may work to prevent EMT. In contrast to our original hypothesis, the other Wnt proteins investigated in this study, Wnt3 and Wnt8a, were not correlated with nuclear β-catenin expression or CRC prognosis. Lee et al. also reported that β-catenin is expressed independently of Wnt3a levels and that Wnt3a expression levels were not correlated with CRC prognosis (3).
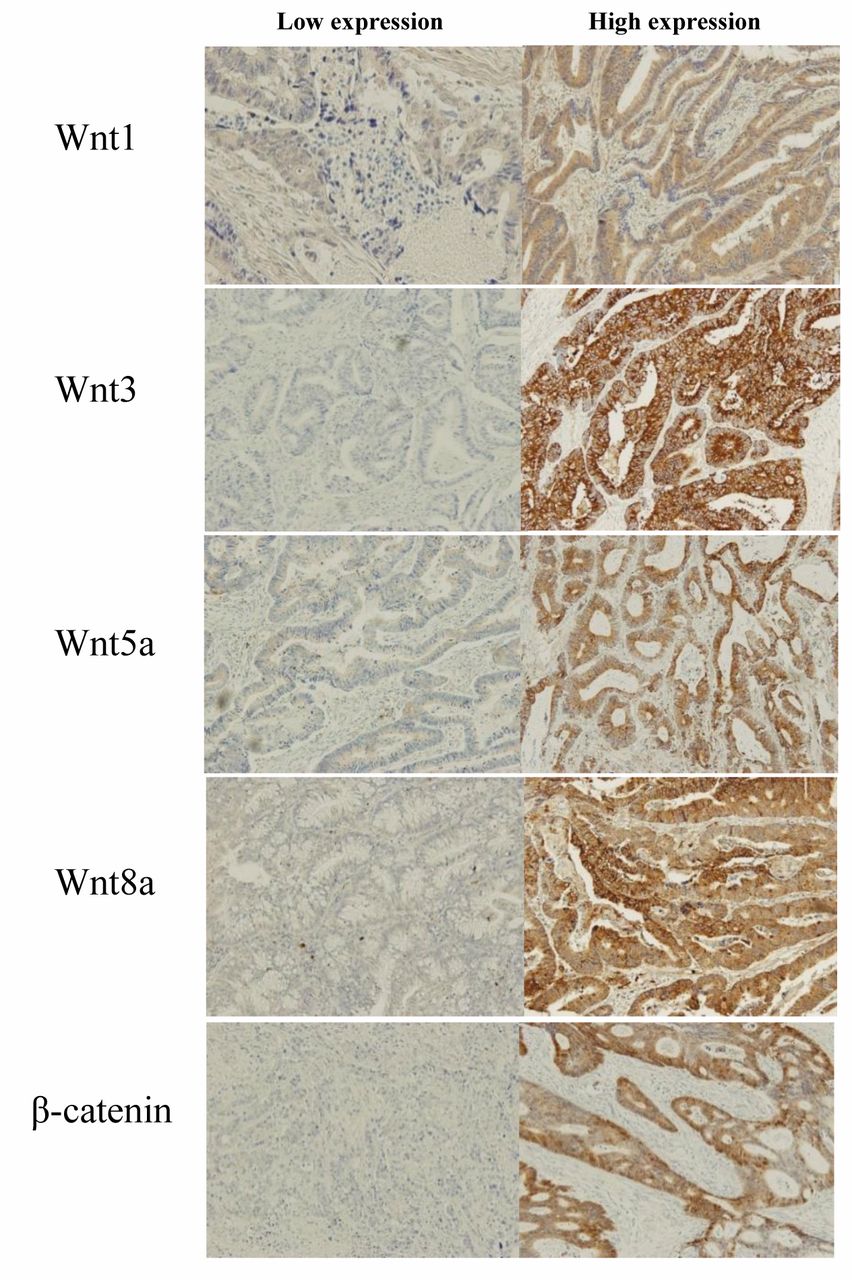
Immunohistochemical staining showing high or low expression levels of each protein. High or low expression levels of each protein as shown by immunohistochemistry. Original magnification ×100.
The Wnt proteins and β-catenin have been studied in various cancers. According to some studies, different sub-types of the Wnt proteins and Fz receptors may activate Wnt signaling pathways depending on cancer type (5). Further studies are required to elucidate the role of the Wnt/β-catenin signaling pathway in each cancer type. If the role of each Wnt protein in cancer is clearly and thoroughly understood, Wnt proteins may become valuable prognostic markers and targets for specialized molecular cancer therapy (11).

Kaplan-Meier curves for disease-free survival (a) and overall survival (b) based on nuclear β-catenin expression. The continuous line indicates nuclear β-catenin positivity and the dotted line indicates nuclear β-catenin negativity (Kaplan-Meier method, log-rank test).
Univariate and multivariate analysis of disease-free survival using the Cox proportional hazard regression model.
Univariate and multivariate analysis of overall survival by Cox proportional hazard model.
- Received April 3, 2015.
- Revision received May 8, 2015.
- Accepted May 11, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}