


Abstract
Background/Aim: Interferon alpha (IFNα) is used sparingly in the management of neuroendocrine tumors (NETs) due to toxicity and perceived limited efficacy. Other medical therapeutic options include somatostatin analogues and molecular-targeted agents, as well as chemotherapy and radionuclide targeted-therapy. The aim of the present study was to perform a retrospective analysis of patients treated with IFNα. Patients and Methods: Patients were identified from the NET database. Radiological, biochemical and symptomatic response were assessed. Progression-free survival (PFS), adverse events and toxicities were recorded. Results: Thirty-five patients were treated with IFNα, with a mean age of 60.1 (range=38-85) years; eight patients (23%) withdrew before 3 months, one (3%) had complete response; there was one partial response; 25 patients (71%) had at least three months of stable disease. The median PFS was 25 months. Conclusion: IFNα demonstrated efficacy and was reasonably tolerated. IFNα may still have a role in small-volume diffuse disease, in syndromic patients where there is resistance to somatostatin analogue, or as a bridge to other therapies.
Neuroendocrine tumors (NETs) are a heterogeneous group of tumors that are derived from the diffuse endocrine system and originate most commonly in the gastrointestinal tract, pancreas, and lung (1, 2). They are relatively rare, with an incidence of approximately five new cases per 100,000 population per year but have a prevalence of 35 in 100,000. They are often slow-growing. The overall 5-year survival for patients with metastatic NETs is 35% (3). With functional tumors, patients present with symptoms associated with hormone hypersecretion. The most common functional syndrome is carcinoid syndrome, which involves a constellation of symptoms, including diarrhea, abdominal pain, flushing, bronchospasm and carcinoid heart disease (4). Most NETs are non-functional, with no syndromic features associated with hormone hyper-secretion (5).
Surgical resection is the only curative treatment, although in over 50% of patients, NETs are metastatic at the time of diagnosis (6). There are many medical therapies for NETs. Somatostatin analogues (SSAs) are the first-line therapy for syndromic patients (2) and more recently they have been demonstrated to have antitumor effects (7, 8). Systemic chemotherapy including platinum regimens are used in first line for poorly differentiated tumours, whereas streptozocin and temozolomide chemotherapy regimens are considered for advanced pancreatic NET. Intestinal NETs, however, are generally poorly-responsive to chemotherapy. Other approaches in the management of NETs include peptide receptor radionuclide therapy (PRRT) with the radiolabelled SSAs 90-yttrium- or 177-lutitium-DOTA octreotide or octreotate. For liver metastases, local ablative and locoregional therapies are used. More recently, molecular- targeted therapies have been developed, including sunitinib, a multi-targeted tyrosine kinase inhibitor (9), and everolimus, an inhibitor of mammalian target of rapamycin (10). In 2011, these were licensed for the management of progressive pancreatic NET (11). Both therapies rarely cause tumor shrinkage, however, disease stabilisation occurs in 60-80% of patients but the burden of toxicities is not insignificant (5).
Interferon-alpha (IFNα) is a cytokine that mediates anti-viral, anti-proliferative and anti-tumour activities. It has been used alone, and combined with chemotherapy and SSAs to treat metastatic NETs since 1982 (2, 12). IFNα is given as a subcutaneous injection, most often at a dose of 3-5 million units (mU) three times a week or alternatively as weekly injections of 75-150 μg long-acting pegylated (PEG)-IFNα (6). Side-effects include initial flu-like symptoms, chronic fatigue, depression, anaemia and neutropenia. In addition, autoimmune responses are manifested in 15-20% of patients, most commonly thyroid dysfunction (2).
With the advent of new therapies and the presumed side-effect profile and toxicities associated with IFNα, it has largely fallen out of favour. There remain some patients that may benefit from IFNα as either an adjunct to treatment, or a bridging therapy while awaiting commencement of another treatment. The purpose of this study was to identify patients that had undergone treatment with IFNα in order to determine the rationale for IFNα use, its side-effects, and the response in terms of symptoms, hormone biochemistry and radiological progression-free survival (PFS).
Patients and Methods
Patient selection. A retrospective analysis of patients with NETs treated with IFNα was performed. Patients were selected from the Royal Free Hospital Neuroendocrine Tumour Unit database of 1,400 patients (2000-2012) and all patients with metastatic well-differentiated NETs treated with IFNα were included in the study. Patient demographics and tumor histology data were recorded. NETs were histologically-graded according to the 2010 WHO classification of gastroentero-pancreatic NETs as G1, G2 or G3, based on the proliferative rate, which is measured by mitosis per 10 high-power fields, or Ki67-positive tumor cells as percentage of all cells (13).
Assessing response and toxicity. Response to IFNα was measured in three ways: radiologically, biochemically and symptomatically.
Radiological: Radiological response was assessed according to the Response Evaluation Criteria in Solid Tumours (RECIST) guidelines Version 1.1 (14). Baseline computerised tomography imaging was compared with imaging at 3, 6, 12, 18 and 24 months following commencement of therapy, and every 6 months thereafter where therapy continued.
Biochemical: Levels of plasma chromogranin A (CgA, measured at the Hammersmith Gut Hormone Reference Laboratory, London, UK) and 24-hour urine 5-hydroxyindoleacetic acid (5HIAA; measured by the Chemical Pathology Department, Royal Free Hospital, London, UK) were recorded where available, at baseline and at set time points thereafter as per imaging.
Symptomatic: In patients with carcinoid syndrome, symptomatic improvement was recorded in terms of number of episodes of flushing or diarrhoea per day at regular time points.
Toxicities to IFNα were recorded according to the Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0 published by the National Cancer Institute (15).
Statistics. SPSS Version 21 was used to analyze the data. Kaplan–Meier survival plots were used to evaluate PFS. Log-rank tests were used to compare PFS between patient subgroups. Paired-samples t-tests were used to compare levels of CgA and 5HIAA at baseline and set time points. Wilcoxon signed-rank tests were used to evaluate symptomatic response.
Ethics. This study was approved by the Royal Free Hospital Trust Local Ethics Chair of Committee.
Results
Thirty-five patients were identified, 25 males and 10 females (Table I). The primary tumor was of midgut origin (57%) pancreatic (20%), unknown primary (14%), and then one patient each of hindgut, bronchial and thymic origin. Twenty (57%) underwent surgical resection of the primary tumor and four (11%) had liver resection for metastases.
Indications for commencing IFNα are shown in Table II. Ten patients (29%) were prescribed IFNα as a first-line anti-proliferative treatment, typically for low-grade, small-volume disease with a low proliferative index and a negative or low-uptake octreotide scan. Four (11%) were commenced on IFNα together with an SSA. A further 19 (54%) started IFNα due to radiological or symptomatic progression during SSA therapy. Four of these patients had been declined funding for radionuclide targeted-therapy, which was contraindicated in a further two due to bone marrow suppression. One patient had severe chronic obstructive airway disease precluding transarterial embolization and another patient had renal failure precluding chemotherapy. Other decision factors included intolerance to SSAs (one patient) and use of IFNα as a bridging therapy whilst awaiting other therapy options in one patient with progressive disease.
The starting dose of IFNα ranged from 1.5-3.5 mU three times per week, with the majority (86%) being treated with 3 mU three times per week. One patient (3%) was given PEG-IFNα. During therapy, the dose was increased in 11 patients (31%) due to radiological or biochemical progression and reduced in four patients (11%) due to toxicities. During the course of therapy, six patients (17%) commenced an SSA due to biochemical or symptomatic progression and two (6%) underwent transarterial embolization due to disease progression.
The duration of IFNα therapy ranged from 19 days to 64 months, with a median of 11 months. At the time of the last recorded follow-up, seven patients (20%) were still being treated with IFNα and 28 (80%) had discontinued therapy. Eight (23%) patients withdrew after less than 3 months of therapy: one due to death, five due to toxicity or poor tolerance, one due to anaemia and one due to progressive disease. Beyond 3 months of therapy, reasons for stopping were as follows: three (9%) due to death; 10 (29%) due to progressive disease (radiological or biochemical); 5 (14%) due to IFNα toxicity; 1 (3%) due to the patient wishing to stop after 29 months of clinical and radiological stability; and 1 (3%) due to 63 months of sustained complete response.
a) Radiological: Radiological response is shown in Figure 1. On an intention-to-treat basis: 1 patient (3%) had complete response; 1 (3%) partial response; 25 (71%) had at least 3 months of stable disease and 20 (57%) at least 6 months of stable disease. Within the first 12 months, 5 patients died (14%) and progressive disease occurred in a further 4 (11%).
At the time of data analysis, 7 patients (20%) had not progressed while on IFNα. Median progression-free survival (PFS) for the whole patient cohort (N=35) was 25 months (95% CI 13.4-36.6). Median PFS was 25 months (N=16, 95% CI 4.5-45.5) for patients on IFNα monotherapy or on a stable dose of SSA at time of the last scan pre-IFNα. PFS was 16 months (N=5, 95% CI=7.4-24.6) for patients starting IFNα and a SSA concomitantly. There was no significant difference between these subgroups (p=0.690, log-rank test). Median PFS was 25 months for midgut NETs (n=9, 95% CI 8.2-41.8) and 26 months for pancreatic NETs (n=5, 95% CI 1.0-60.0) and there was no significant difference between these subgroups (p=0.657, log-rank test) (Figure 2).
Demographic and baseline patients' characteristics.
Indications for interferon-alpha therapy.
b) Biochemical: Thirty patients (86%) had available data for CgA and 13 patients (37%) for 5HIAA. Pre-IFNα, 22 patients (63%) had elevated CgA. At 6 months median CgA increased from 99.4 to 115.0 pmol/l (normal range=0-60pmol/l) but this was not significant (p=0.0574, paired-samples t-test). Nine patients (26%) had elevated 5HIAA pre-IFNα. Median 5HIAA fell from 54 to 29μmol/24h at 6 months (normal range 0-42 umol/24h), although not significant (p=0.508, Paired-samples T-test).
c) Symptomatic: Out of patients on stable-dose SSA or naïve to SSA at baseline, 11 patients (31%) had diarrhea and 13 (37%) had flushing; 9 (26%) had both symptoms. None of these patients were started on a SSA during IFNα therapy. Out of the 11 patients with diarrhea, 3 withdrew within the first 3 months; after 3 months, 5 reported an improvement, 2 worsened and 1 had incomplete data. In the 6 patients with available quantitative data, median daily episodes of diarrhea decreased from 2.75 to 0.5 after 3 months (p=0.102, Wilcoxon signed-rank test). Out of the 13 patients with flushing, 4 withdrew within 3 months; after 3 months, 7 reported an improvement, 1 was unchanged and 1 worsened. In the 7 patients with available quantitative data, median flushes per day fell from 2 to 1 after 3 months (p=0.072, Wilcoxon signed-rank test).
Toxicity: Toxicities were graded according to CTCAE Version 4.0, whereby grade 1 is mild, grade 2 is moderate, grade 3 is severe and grade 4 is life-threatening (see Table III). Forty per cent had grade 1-2 haematological toxicity and 20% grade 3 toxicity (Figure 3). These included anaemia in 51%, leukopenia in 23%, lymphocytopenia in 17%, neutropenia in 11% and thrombocytopenia in 20%. There were no grade 4 toxicities. The only other grade 3 toxicity was depression in 1 patient. Twenty per cent had grade 1-2 depression. Other grade 1-2 toxicities occurring in more than 10% included flu-like symptoms (26%), fatigue (17%), hypothyroidism (11%) and dry skin (14%). Flu-like symptoms tended to occur with initiation of therapy and/or post-injection for a few hours, and were treated with paracetamol. Due to toxicity or poor tolerance, dose was adjusted in 4 patients (11%) and therapy was discontinued in 9 (26%). Out of these 9 patients, 5 were withdrawn within the first 3 months, 1 at 5 months, 1 at 6 months and 1 at 9 months.
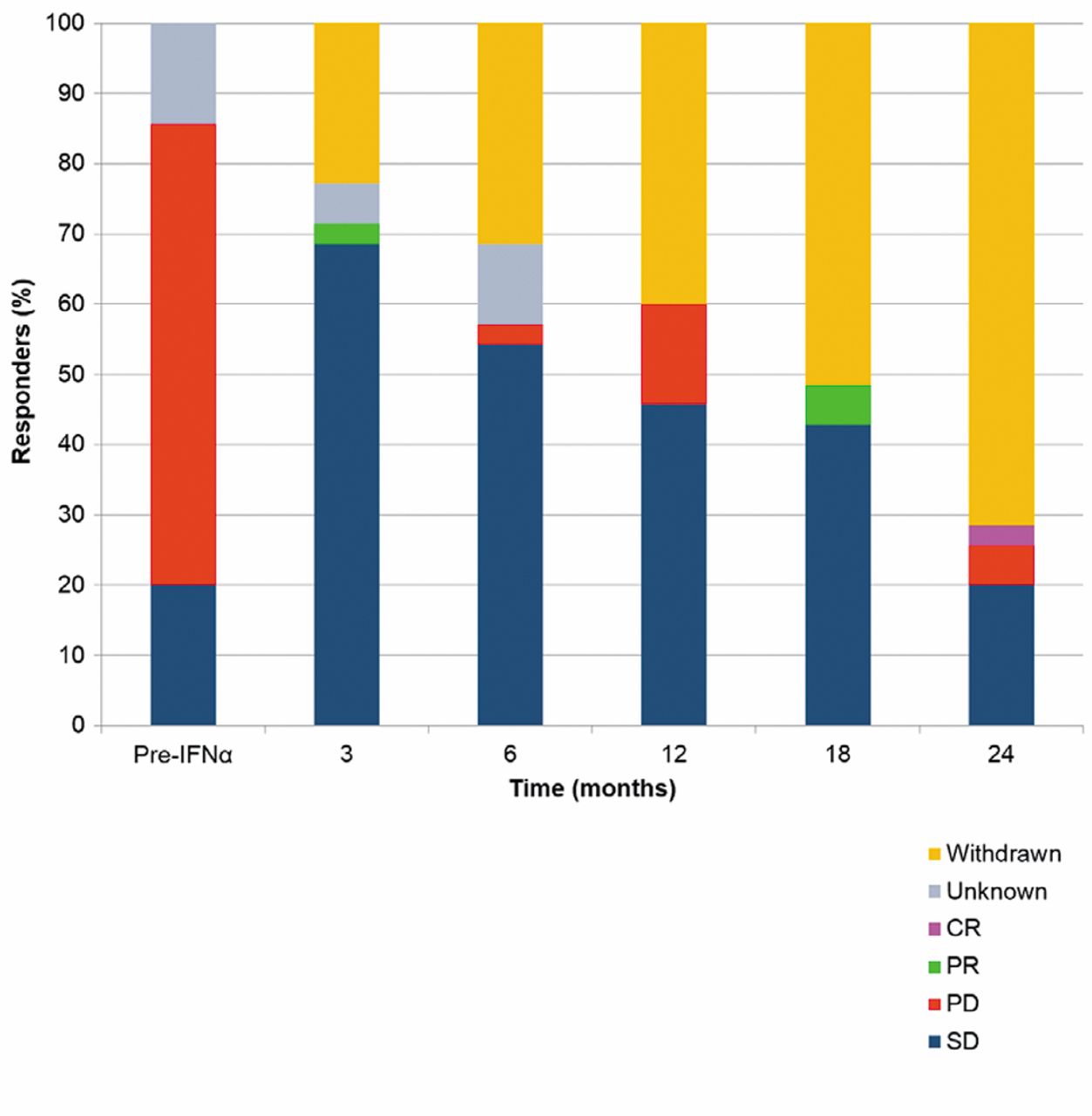
Radiological response to interferon-alpha (IFNα) at each time point. Overall, 71% of patients had at least 3 months of stable disease (SD) or partial response (PR). CR: Complete response; PD: progressive disease.
Discussion
Although at least 66% of patients had progressive disease at baseline, IFNα demonstrated efficacy with inducing or maintaining stable disease in 71% of patients for at least 3 months, with partial or complete response achieved in 6%. Overall median PFS was 25 months. Principally, median PFS was also 25 months for the subgroup of patients with new single-agent IFNα or on a stable dose of SSA prior to therapy. The biochemical and symptomatic responses were not statistically significant in the present study. This study was limited by the small number of patients, its retrospective nature and the heterogeneity of tumour type.
The main rationale for use of IFNα in our cohort of patients was as a second-line therapy following development of resistance to SSA in the form of radiological and/or symptomatic progression. In cases of low grade, small volume disease and a negative or low uptake in octreotide scan, patients were given IFNα as a first-line antiproliferative agent, as this was believed to be more appropriate than SSA. In some cases IFNα was chosen due to comorbidities which contraindicated other therapies such as radionuclide targeted-therapy. Other reasons included SSA intolerance and use of IFNα as a bridging therapy.

Kaplan–Meier plot of progression-free survival (PFS) for patients on interferon-alpha (IFNα) monotherapy or with a stable dose of somatostatin analogue prior to IFNα therapy, for all tumor types (N=16), and midgut (N=9) and pancreatic (N=5) tumours. The survival of patients in the midgut and pancreatic subgroups were not significantly different (p=0.657, log-rank test).
The results of the present study are comparable with historic phase II studies on the treatment of NETs with IFNα monotherapy. Ten studies on IFNα and 1 on IFNγ carried-out between 1987 and 2004 included a total of 274 patients (12-111). Overall, stable disease was induced in 69.4% and partial or complete response in 10.6% (12, 16-25). Notwithstanding the lack of a significant biochemical response in our study, a study by Oberg et al. including 111 patients with carcinoid tumors demonstrated a significant reduction in CgA and 5HIAA in 42% of patients and symptomatic remission in 68% (12). To date, there have been three prospective randomised trials comparing SSA monotherapy with SSAs-plus-IFNα. All three trials were underpowered, with no significant benefit. First, a trial by Kolby et al. (2003) included 68 patients and showed increased 5-year overall survival with octreotide-plus-IFNα, compared to octreotide-alone (57% vs. 37%), but this was not significant (p=0.13) (26). Secondly, a trial by Arnold et al. (2005) in 105 patients with ganstroentero-pancreatic (GEP) NETs demonstrated a median time-to-treatment failure of 32 months for the octreotide group and 54 months for octreotide-plus-IFNα, but again this was not found to be significant (p=0.59) (27). Finally, a trial by Faiss et al. (2003) in 80 patients with GEP-NETs demonstrated no significant difference in PFS between 25 patients receiving lanreotide, 27 receiving IFNα and 28 patients receiving both treatments (p=0.312) (28). This is consistent with our study, in which IFNα combined with a SSA did not significantly improve PFS compared to IFNα monotherapy. Nevertheless, the trial by Faiss et al. demonstrated better symptom control with combination therapy, although toxicities were more common. Within the first 12 months, progressive disease occurred in 56% of patients on IFNα and 50% on combination therapy, in comparison with 23% in our study (28).

Toxicities to interferon-alpha graded according to the Common Terminology Criteria for Adverse Events Version 4.0. Grade 1: Mild; grade 2: moderate; grade 3: severe; grade 4: life-threatening. There were no grade 4 toxicities.
Grading of toxicities in the Common Terminology Criteria for Adverse Events Version 4.0 (15)
The somatostatin analogues are the first line therapy for symptom control of functional NETs, e.g. carcinoid syndrome, and our data for IFNα is inferior to published data for SSAs with regards to diarrhea and flushing. Notably, however, 17% of patients in our study were given IFNα due to symptomatic progression while on SSA; the syndromic control in patients resistant to SSAs is often difficult even with addition of IFNα. Khan et al. demonstrated a 94% symptomatic response to prolonged release Lanreotide (Somatuline Autogel) in a retrospective study of 69 patients with malignant carcinoid syndrome (29). SSAs also have significantly less toxicity. With regards to anti-tumor action, the PROMID study was a randomised controlled trial (RCT) comparing octreotide LAR with placebo in 85 patients with midgut NETs. Median PFS was 14.3 months for octreotide compared to 6.0 months in placebo (7). The CLARINET study was a large-scale, multi-national, double-blind RCT investigating the antiproliferative effect of the SSA lanreotide autogel in 204 patients with non-functioning gastro-enteropancreatic NETs. After 2 years of treatment, median PFS for lanreotide was not reached, compared with 18 months with placebo, and 65% of patients in the lanreotide group had not progressed at 2 years, compared with 33% in the placebo group (8). The anti-tumor effect of IFNα is comparable with a median PFS of 25 months in our study.
In the present study PFS on IFNα was comparable to that for molecular-targeted therapies. In the treatment of advanced pancreatic NETs, a RCT using the tyrosine kinase inhibitor sunitinib versus placebo in 171 patients had a median PFS of 11.4 months compared to 5.5 months in the placebo group. Also in pancreatic NETs, a RCT with the mammalian target of rapamycin inhibitor everolimus versus placebo in 410 patients had a median PFS of 11.0 months compared to 4.6 months with placebo (9, 10). These phase III studies led to the approval of both drugs for progressive pancreatic NETs (11). The evidence to date for everolimus in non-pancreatic NETs is less clear. The RADIANT-2 study was an RCT using everolimus-plus-octreotide LAR compared to placebo-plus-octreotide LAR. Four hundred and twenty nine patients with carcinoid tumors were included (52% midgut primary). Median PFS was 16.4 months (95% CI 13.7-21.2) versus 11.3 months (8.4-14.6) in placebo, with 95% confidence intervals overlapping (30). In contrast, our study did not demonstrate a significant difference between pancreatic and midgut NETs, although this is most likely due to the small numbers.
Many clinicians prefer not to use IFNα due to the side-effects (31). Although toxicity caused withdrawal from IFNα therapy in almost one third of patients, this occurred most frequently within the first 3 months. Thus, this study suggests that earlier identification of patients that may not tolerate treatment would be beneficial.
In this study, 20% of patients had grade 3 toxicities, most frequently lymphocytopenia. There were no grade 4 toxicities. In the sunitinib trial, the sum of percentage of patients with each grade 3 or 4 toxicity was 63%, compared to 36% in placebo. For everolimus, these statistics were 44% versus 8%.
In conclusion, despite the limitations of the present study, especially related to the number of patients and retrospective data, there is evidence of efficacy and reasonable tolerability. IFNα may still have a valuable role in the management of metastatic NETs. Perhaps the most useful roles for IFNα include: control of carcinoid syndrome in somatostatin receptor-negative patients or patients who have developed resistance to or have become intolerant to SSA; as an addition to SSA in order to control symptoms; as an anti-proliferative therapy in small volume diffuse disease in G1 and G2 tumours; anti-proliferative therapy as a bridge to other therapies e.g. PRRT when there can be delays in logistics of PRRT therapy. Further prospective studies are required to compare IFNα with newer molecular-targeted therapies and determine whether there is merit in their combination with newer agents.
- Received July 3, 2014.
- Revision received August 4, 2014.
- Accepted August 6, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.