


Abstract
Background: Desmoplastic small round cell tumour (DSRCT) is a rare and aggressive cancer that usually develops in the peritoneal cavity of young males. Its prognosis is dismal, with current treatment options including the combination of multi-agent chemotherapy, aggressive surgery, radiation therapy, and autologous stem cell transplantation. Hyperthermic intraperitoneal chemotherapy (HIPEC) may also be an option. Case Report: Herein we report the administration of the marine-derived multi-target antineoplastic agent, trabectedin, in a patient with DSRCT, heavily pre-treated with conventional multi-agent chemotherapy, HIPEC, and surgery. Results: The patient achieved a prolonged partial response and an extended period of stable disease with third-line trabectedin, following disease progression after conventional multi-agent chemotherapy, HIPEC, and surgery. Conclusion: Trabectedin may be a treatment option in multimodal therapy for the management of DSRCT and warrants further research to explore the impact of trabectedin in the treatment of this disease.
Desmoplastic small round cell tumour (DSRCT) is a member of the family of poorly-differentiated round cell tumours including Ewing's sarcoma (EWS), anaplastic synovial sarcoma, neuroblastoma, rhabdomyosarcoma, and neuroectodermal tumors (1-3). It is a very aggressive malignancy that typically affects young males, causing obstructive symptoms from large abdominal or pelvic masses, and involving widespread peritoneal seeding with metastases to the liver, lung, and lymph nodes (1, 4). Being of possible mesothelial origin, DSRCT is characterized by distinctive cytological, histological and immunohistochemical features and the involvement of a recurrent chromosomal abnormality, t(11;22)(p13;q12), in its pathogenesis (1-3). The translocation, involving the Ewing's sarcoma gene (EWS) on chromosome 22 and the Wilms' tumour gene (WT1) on chromosome 11 and resulting in the formation of an aberrant EWS–WT1 fusion gene, is specific to DSRCT and functions as a definitive diagnostic marker. Due to the rarity of the tumour and a diversity of treatment options, there is currently no consensus on optimal management, and the prognosis for patients with DSRCT remains extremely poor. Multimodal treatment approaches commonly consist of multi-agent chemotherapy followed by aggressive debulking surgery aimed at resecting all or most of the tumour; radiation therapy; and high-dose chemotherapy with peripheral blood stem cell transplantation. Various studies have reported cyclophosphamide, ifosfamide, adriamycin, vincristine, etoposide, and topotecan as effective cytotoxic agents (5, 6). Hyperthermic intraperitoneal chemotherapy (HIPEC) may also be considered as part of a multimodality therapy approach. However, approximately 75% of patients with DSRCT will succumb to their disease within three years (4), and survival remains low, even with aggressive multimodality therapy and optimal surgical resection, where an overall survival rate of 55% at three years has been reported (7).
Herein, we report a partial response and an extended period of stable disease following administration of the marine-derived multi-target anti-neoplastic agent, trabectedin, in a patient with DSRCT heavily pre-treated with conventional multiagent chemotherapy, HIPEC, and surgery.
Case Report
On June 2011, a 20-year-old man was admitted to our Institute with a diagnosis of DSRCT, determined elsewhere through a laparoscopic peritoneal biopsy. An abdominal computed tomographic (CT) scan demonstrated a voluminous abdominal mass, 12 cm in maximum diameter, causing compression of the seminal vesicles, bladder, and rectum, with associated ascites and multiple peritoneal nodules. 18F-fluorodeoxyglucose (FDG) positron-emission tomography (PET) showed multiple accumulations of a glucose analogue in the same lesions detected using CT.
A first-line chemotherapy regimen was initiated with the aim of obtaining sufficient tumour shrinkage to allow subsequent surgical debulking. The patient was treated with three cycles of combination chemotherapy with cisplatin (50 mg/m2), epirubicin (75 mg/m2), and vinorelbine (25 mg/m2) administered on day 1 every three weeks, leading to stable disease, which meant that a surgical approach was not possible.
Second-line treatment based on a 14-day continuous infusion of high-dose ifosfamide (1 g/m2) for two cycles was administered, without significant clinical or radiological response. Therefore, the patient underwent debulking surgery with colorectal resection, pelvic peritonectomy, appendectomy, omentectomy, splenectomy, iliac lymphoadenectomy, and resection of peritoneal nodules. Surgery was associated with perfusion of the abdominal cavity with HIPEC. After 40 days, a second surgery involving right hemicolectomy, ileal resection, and diaphragm peritonectomy was undertaken. No radiation treatment was carried-out in light of the peritoneal involvement.
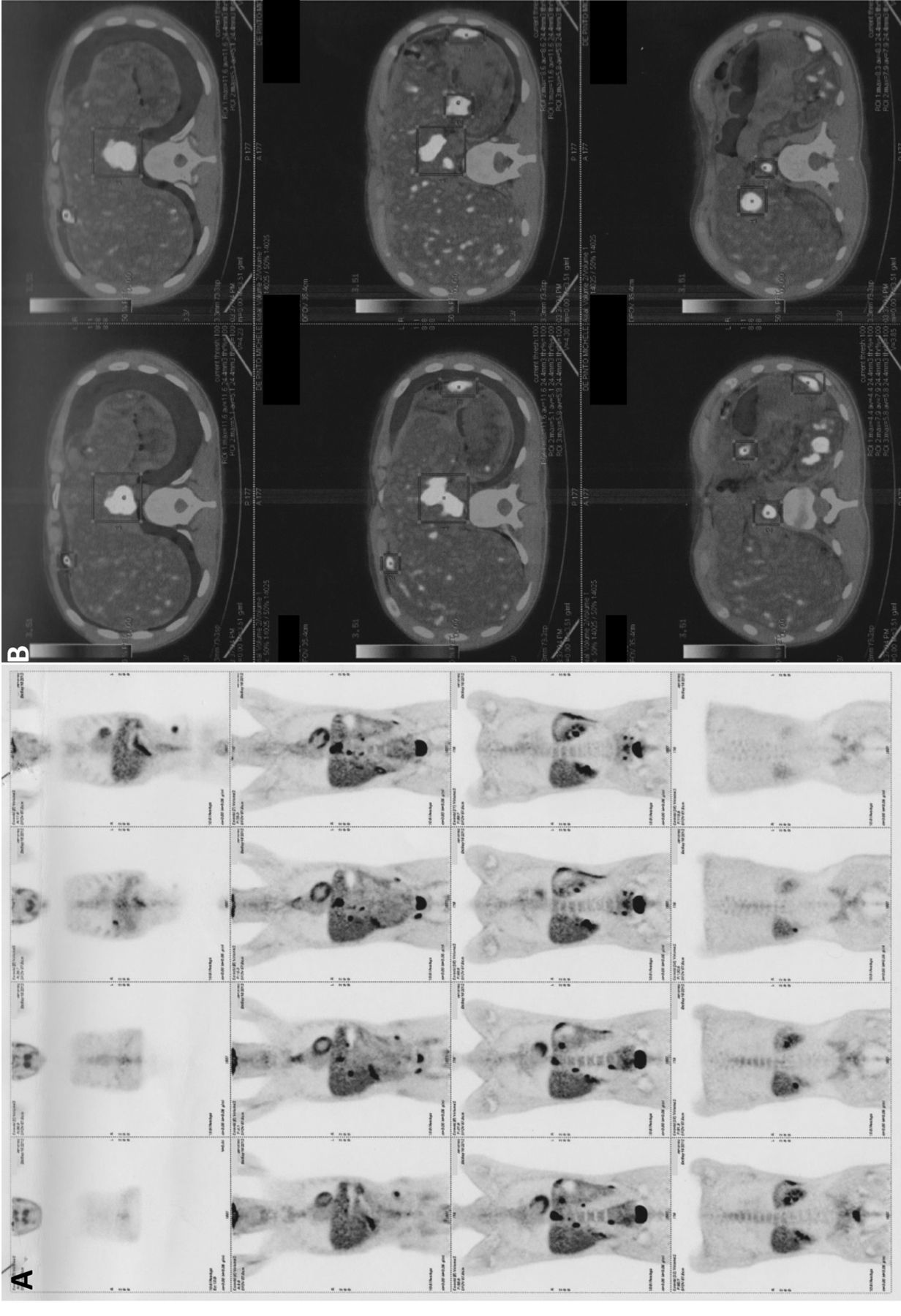
Two months later, a CT scan and FDG-PET showed recurrence in the lombo-aortic, inguinal lymph nodes, and liver peritoneum. The patient was started on third-line treatment with trabectedin (1.5 mg/m2 q3w), with dexamethasone premedication (8 mg intravenous 1 h before infusion). Objective response was evaluated using FDG-PET and CT, and assessed using Response Evaluation Criteria in Solid Tumors (RECIST) (8). There was a partial response after four cycles, and stable disease at the end of eight cycles. Figure 1 shows FDG-PET/CT images taken at the initiation of trabectedin treatment in September 2012, in November 2012, and in February 2013. The images highlight a gradual reduction in FDG uptake at the liver hilar lymphadenopathy, and at lymph nodes along the lesser curvature of the stomach, inter-aortocaval, lumbar, iliac and right inguinal areas. In addition, a corresponding reduction in FDG uptake can also be appreciated in multiple peritoneal nodes, especially along the liver margins. In fact, the maximum standardized uptake values for all lesions were reduced from a range of 9.1-11.6 to a range of 6.6-7.9 from September 2012 to February 2013.
Our patient remained asymptomatic with an improved quality of life throughout this time, and treatment tolerability was good, with the only adverse event consisting of two episodes of grade 1 neutropenia. No dose reductions because of toxicity were required.
Finally, after six months, FDG-PET imaging showed progression of his disease. The patient is currently alive.
Discussion
DSRCT is a rare aggressive tumour with a poor prognosis and few long-term survivors. Treatment strategies for DSRCT include intensive multi-agent chemotherapy, aggressive surgical debulking, adjuvant whole-abdominal radiation, HIPEC, and myeloablative chemotherapy with autologous stem cell rescue. However, the rarity of this neoplasm has prevented the development of a standard therapy, particularly for inoperable and metastatic DSRCT cases, and therapeutic management remains challenging and the prognosis poor.
Trabectedin (Ecteinascidin-743; ET-743; Yondelis®, Pharma Mar S.A., Madrid, Spain) is novel tetrahydroisoquinoline alkaloid originally extracted from the Caribbean sea squirt Ecteinascidia turbinata, and now produced synthetically (9). It is approved in Europe for the treatment of adult patients with advanced soft tissue sarcoma after failure or unsuitability of anthracyclines or ifosfamide. Administered via a central venous catheter using a Baxter LV10 elastomeric pump by continuous infusion over 24 h every 21 days at a dose of 1.5 mg/m2, trabectedin has shown antineoplastic activity in translocation-related tumors such as Ewing's sarcoma, liposarcoma, leiomyosarcoma, myxoid-round cell liposarcoma, rhabdomyosarcoma, and synovial sarcoma (2, 10-12). Activity has also been shown in another case of DSRCT where, at last reporting, the patient was alive without progression eight months after third-line therapy with trabectedin and four years after the initial diagnosis (13).
Trabectedin appears to act by binding to the DNA minor groove, interfering with the binding of a number of transcription factors and DNA repair proteins to DNA (11, 14). Several researchers have suggested that the sensitivity of specific translocation-related sarcomas to trabectedin could be related to a direct inhibitory effect on the Fused in Sarcoma (FUS)–CHOP fusion protein, produced by the t(12;16)(q13;p11) translocation (10, 15, 16). As DSRCT similarly involves a translocation leading to the generation of a chimeric fusion protein, in this case EWS–WT1, a similar mechanism of action may explain the effect of trabectedin seen in our patient with DSRCT. Trabectedin at therapeutic concentrations acts on the tumor microenvironment and directly inhibits tumor cell proliferation. In particular, the in vitro production of two pro-inflammatory mediators, interleukin-6 and the cytokine chemokine C-C ligand 2 (CCL2), was markedly down-regulated by trabectedin in monocytes, macrophages, tumour-associated macrophages and freshly-isolated ovarian tumour cells (17-20).
The response to trabectedin in our patient is notable. Following disease progression despite two lines of intensive chemotherapy, HIPEC, and three rounds of aggressive surgery, he achieved a partial response after 12 weeks of trabectedin at 1.5 mg/m2 every three weeks. Trabectedin was well-tolerated, with mild neutropenia being the only adverse event recorded. At the end of 24 weeks of treatment with trabectedin, his disease remained stable, before disease progression was finally noted nine months later. Our patient is still alive, 29 months after his initial diagnosis.

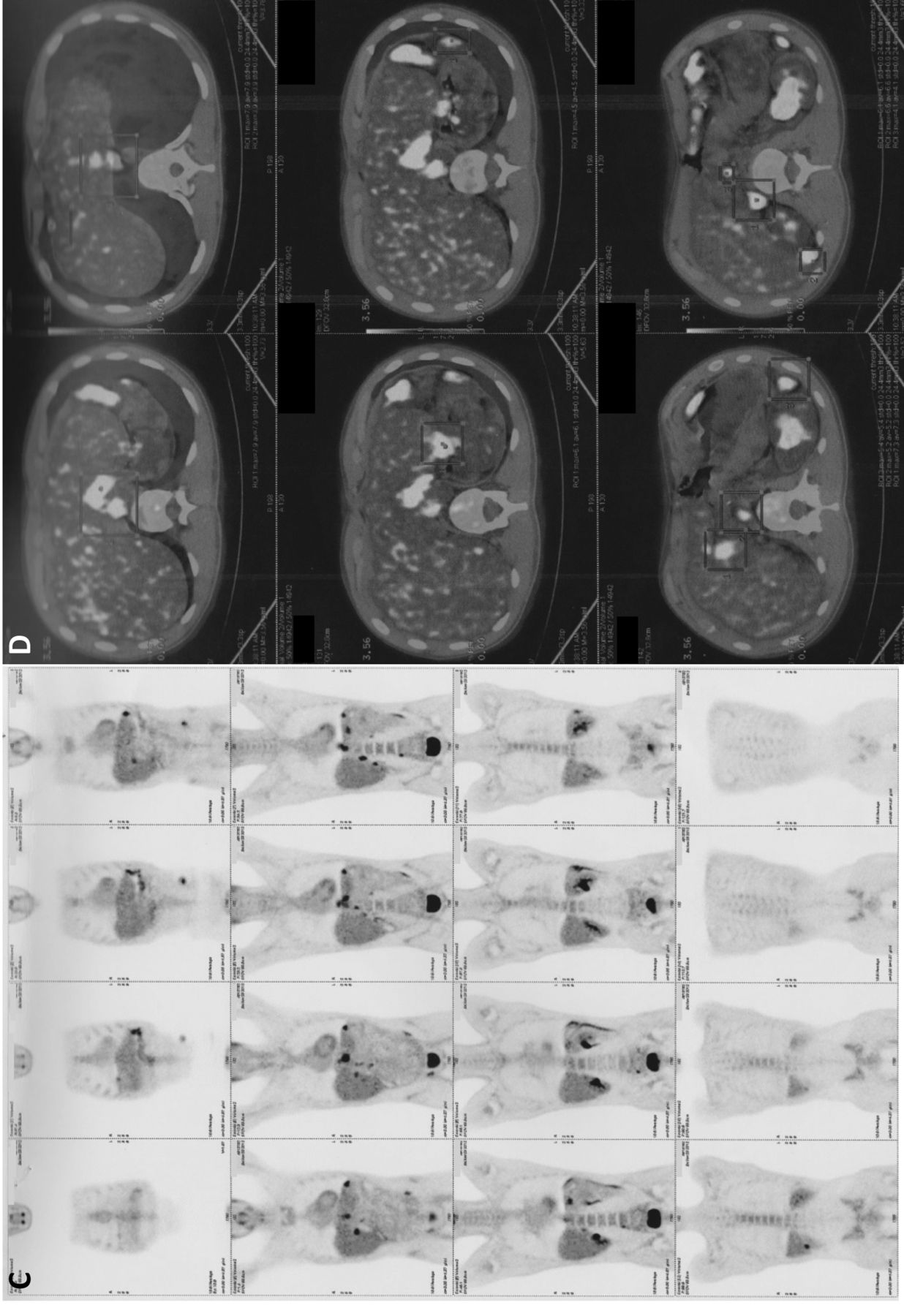

18F-fluorodeoxyglucose positron-emission tomography/computed tomographic scans at the initiation of trabectedin treatment in September 2012 (A and B), in November 2012 (C and D), and in February 2013 (E and F). The maximum standardized uptake values for all lesions were reduced from a range of 9.1-11.6 to a range of 6.6-7.9.
Conclusion
Our case report suggests that trabectedin may be considered as a treatment option in multimodality therapy for the management of DSRCT. Further research is warranted to explore the impact of trabectedin on the treatment of this disease.
Acknowledgements
The Authors thank Ray Hill, an independent medical writer, who provided medical writing support on behalf of Health Publishing & Services (HPS) Srl, Milan, Italy. This assistance was funded by PharmaMar, Spain.
Footnotes
-
Conflicts of Interest
The Authors declare that they have no conflicts of interest.
- Received March 15, 2014.
- Revision received May 23, 2014.
- Accepted May 26, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}