


Abstract
Aim: To analyze retrospectively the results of postoperative external beam radiotherapy (EBRT) for resected pancreatic adenocarcinoma. Patients and Methods: The records of 47 patients treated with gross complete resection (R0: 24 patients, R1: 23 patients) and post-operative EBRT were reviewed. The median dose of EBRT was 50 Gy (range, 12-60 Gy), and chemotherapy was used in 37 patients (78.7%). The median follow-up period for all 47 patients was 14.4 months (range, 0.9-67.9 months). Results: At the time of this analysis, 24 patients (51.1%) had disease recurrence. Local failure was observed in 10 patients (21.3%), and the 2-year local control (LC) rate in all patients was 68.7%. Patients treated with EBRT and chemotherapy had a significantly more favorable LC (2-year LC rate: 76.0%) than those treated with EBRT alone (2-year LC rate: 40%, p=0.0472). The median survival time and the 2-year actuarial overall survival (OS) in all 47 patients were 30.0 months and 54.5%, respectively. Patients treated with EBRT and chemotherapy had a significantly more favorable OS (2-year OS rate: 61.6%) than those treated with EBRT alone (2-year OS: 25.0%, p=0.0454). On univariate analysis, chemotherapy use alone had a significant impact on OS, and on multivariate analysis, chemotherapy use also was a significant prognostic factor. There were no late morbidities of NCI-CTC Grade 3 or greater. Conclusion: Post-operative EBRT with chemotherapy yields a favorable LC rate for resected pancreatic adenocarcionoma, and EBRT combined with chemotherapy confers a survival benefit compared to EBRT alone.
Pancreatic cancer is one of the leading causes of cancer death worldwide. The prognosis of patients with this disease remains extremely poor, with a 5-year survival rate after diagnosis of less than 5%. Only a small percentage of patients (10-20%) are candidates for surgical resection (1, 2). However, even if curative resection is performed, 5-year survival rates are approximately only 10-20% (3-5). Such dismal outcomes are caused in large part by high rates of locoregional and distant failure, even in patients with early-stage tumors (5, 6). These patterns of failure suggest that both systemic and local adjuvant therapy may have a positive impact on survival.
Patient and disease characteristics.
To improve the survival after surgical resection for pancreatic cancer, researchers have explored adjuvant radiotherapy and chemotherapy. Although the role of adjuvant chemoradiotherapy for resected pancreatic cancer remains controversial, several reports have indicated the efficacy for combined chemotherapy and radiotherapy (7-10). The Gastrointestinal Tumor Study Group (GITSG) conducted a randomized trial and reported a survival benefit with the addition of chemoradiotherapy to surgical resection (7). Recently, several retrospective reports with a large number of patients have also suggested the efficacy of adjuvant chemoradiotherapy for resected pancreatic cancer on survival compared with postoperative observation alone (11, 12). However, the precise role of adjuvant external beam radiotherapy (EBRT) for patients undergoing resection for pancreatic cancer remains unclear.
Treatment characteristics.
In the current study, we reviewed a retrospective and multi-institutional series of 47 patients with pancreatic adenocarcinoma who underwent gross complete resection followed by EBRT, and evaluated the efficacy and safety of postoperative EBRT alone and with chemotherapy.
Patients and Methods
The Japanese Radiation Oncology Study Group (JROSG) conducted a nationwide questionnaire survey regarding radiotherapy for patients with non-metastatic pancreatic cancer patients treated between 2000 and 2006. The questionnaire included detailed information regarding patient characteristics, treatment characteristics and treatment outcomes. Details of the JROSG survey have been described elsewhere (13-15). In brief, 34 radiation oncology centers in Japan which belong to the JROSG agreed to participated in this survey, and detailed information on 870 patients was acquired. Of these, 51 patients were treated with gross complete resection and postoperative EBRT. The histology of 47 patients was adenocarcinoma, 1 patient had anaplastic carcinoma, and 3 patients had no histological information. These latter 4 patients were excluded from this analysis, and the remaining 47 patients with histologically diagnosed adenocarcinoma were included in the current study.
Agents and chemotherapy schedules (n=114).
Patient and disease characteristics in all 47 patients are shown in Table I. The median age of all patients was 65 years (range, 39-83 years) and Eastern Cooperative Oncology Group (ECOG) performance status (PS) ranged from 0 to 2 (median: 1). One-hundred and fifty-two patients (70.0%) had R0 resection and the remaining 65 patients had R1 resection (R0: gross complete resection with negative margins, R1: gross complete resection with positive margins). We used the tumor staging system devised by the Union Internationale Contre le Cancer (16). Of the 47 patients, 33 (70%) had pathological T3-4 disease, and approximately 50% of patients had pathological N1 diseases. The median maximum tumor size was 3.0 cm (range, 0.9-10.0 cm) and the median serum concentration of carbohydrate antigen 19-9 (CA19-9) was 167.9 U/ml (range: 4.9-13,080 U/ml). All patients underwent total or regional pancreatectomy with radical lymph node dissection of the para-aortic area as well as peripancreatic regional nodes. Total pancreatectomy, distal pancreatectomy, pancreaticoduodenectomy and the Appleby procedure was performed for 6, 8, 32 and 1 patients, respectively.
Treatment characteristics in all 47 patients are shown in Table II. The total doses of EBRT (International Commission on Radiation Units and Measurements 50) ranged from 12 to 60 Gy (median: 50 Gy), with a single fraction of 1.8-2 Gy 5 days per week. The treatment field of EBRT consisted of the primary tumor only in 44.7% of patients and the primary tumor plus regional lymph nodes in the remaining 55.3% of patients. Computed tomography (CT)-based treatment planning and conformal radiotherapy were both used in 74.5% (35/47) of patients.
Chemotherapy was administered to 37 patients (78.7%). Agents and chemotherapy schedules are described in Table III. When administering gemicitabine (GEM) before and during radiotherapy, a dose of 1,000 mg/m2 was usually administered weekly for 3 weeks with a 1-week rest, depending on response and toxicity. Some patients received GEM at a dose of 250-350 mg/m2 intravenously weekly during radiotherapy for approximately 6 weeks. GEM maintenance chemotherapy was usually given at 1,000 mg/m2 weekly for 3 weeks with a 1-week rest until disease progression or unacceptable toxicity. 5-Fluorouracil (5-FU) was generally administered via continuous infusion at 200-300 mg/m2/day daily just prior to each irradiation as part of the chemoradiotherapy protocol. After the completion of chemoradiotherapy, patients continued receiving 300-400 mg/m2 5-FU intravenous bolus infusion until CT evaluation revealed tumor progression. S-1 was administered orally twice daily on the day of irradiation during and after radiotherapy. S-1 doses ranged from 60 to 80 mg/m2. Patients treated with cisplatin (CDDP) received approximately 5 mg/m2 during and/or after radiotherapy. Tegafururacil (UFT) was administered at 300 mg/m2 daily during and/or after radiotherapy.
In the current study, there were no definitive treatment policies for pancreatic cancer during the survey period; thus treatment was determined by the respective physicians at each institution. We assigned 47 patients into 2 treatment modality groups by chemotherapy use (yes vs. no) to determine whether the chemotherapy use influenced patient characteristics (Table IV). There were no significant differences in patient characteristics, such as tumor size, CA19-9 level and pathological stages based on classification by chemotherapy use.
The median follow-up of all 47 patients was 14.4 months (range, 0.9-67.9 months). Overall survival (OS), progression-free survival (PFS), metastasis-free rates and local control (LC) rates were calculated actuarially according to the Kaplan-Meier method (17) and were measured starting from the day of initial treatment. Differences between groups were estimated using the Chi-square test, Student's t-test and the log-rank test (18). Multivariate analysis was performed using the Cox regression model (19). A probability level of 0.05 was chosen for statistical significance. Statistical analysis was performed using the SPSS software package (version 11.0, SPSS, Inc, Chicago, IL, USA). Late complications were graded in accordance with the National Cancer Institute-Common Terminology Criteria (NCI-CTC) Version 3.0.
Results
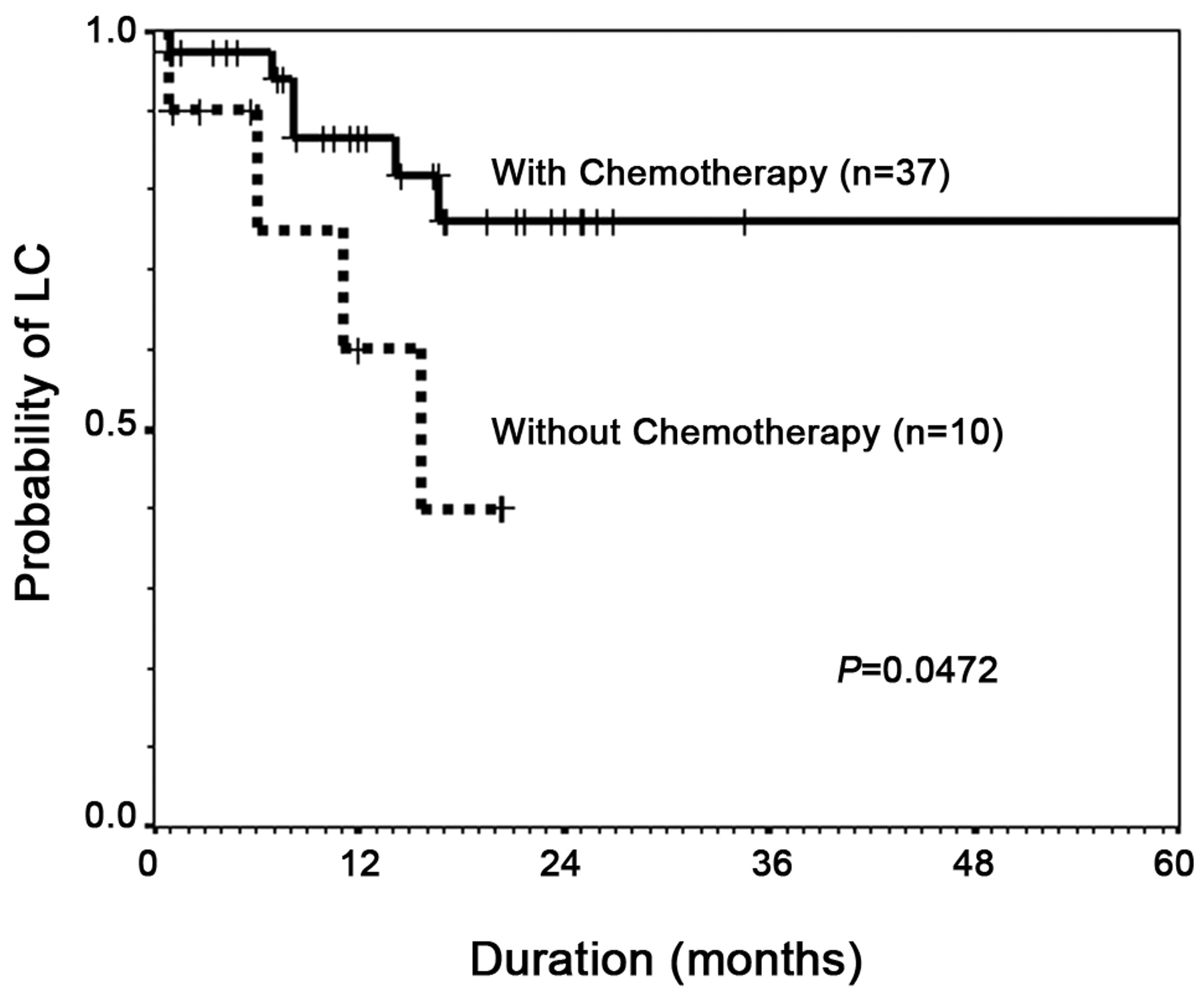
At the time of this analysis, 24 patients (51.1%) had disease recurrences (local only in 5 patients, regional lymph nodes only in 1 patient, liver only in 4 patients, peritoneum only in 4 patients, lung only in 4 patients, and multiple sites in 6 patients). For 6 patients with multiple recurrences, 5 patients had a simultaneous local recurrence. Therefore, local recurrence occurred in a total of 10 patients (21.3%). The 2-year actuarial LC rate in all 47 patients was 68.7% (Figure 1). Patients who received chemotherapy had a statistically significantly higher LC rate than those who received EBRT alone (p=0.0472), and the 2-year actuarial LC rates in patients with chemotherapy use and those without chemotherapy use were 76.0% and 40.0%, respectively (Table V, Figure 2). On the other hand, other factors, such as CA19-9 level, pathological T stage, pathological N stage, degree of resection and total radiation dose, did not influence LC (Table V).
Comparisons of patient characteristics according to chemotherapy use.
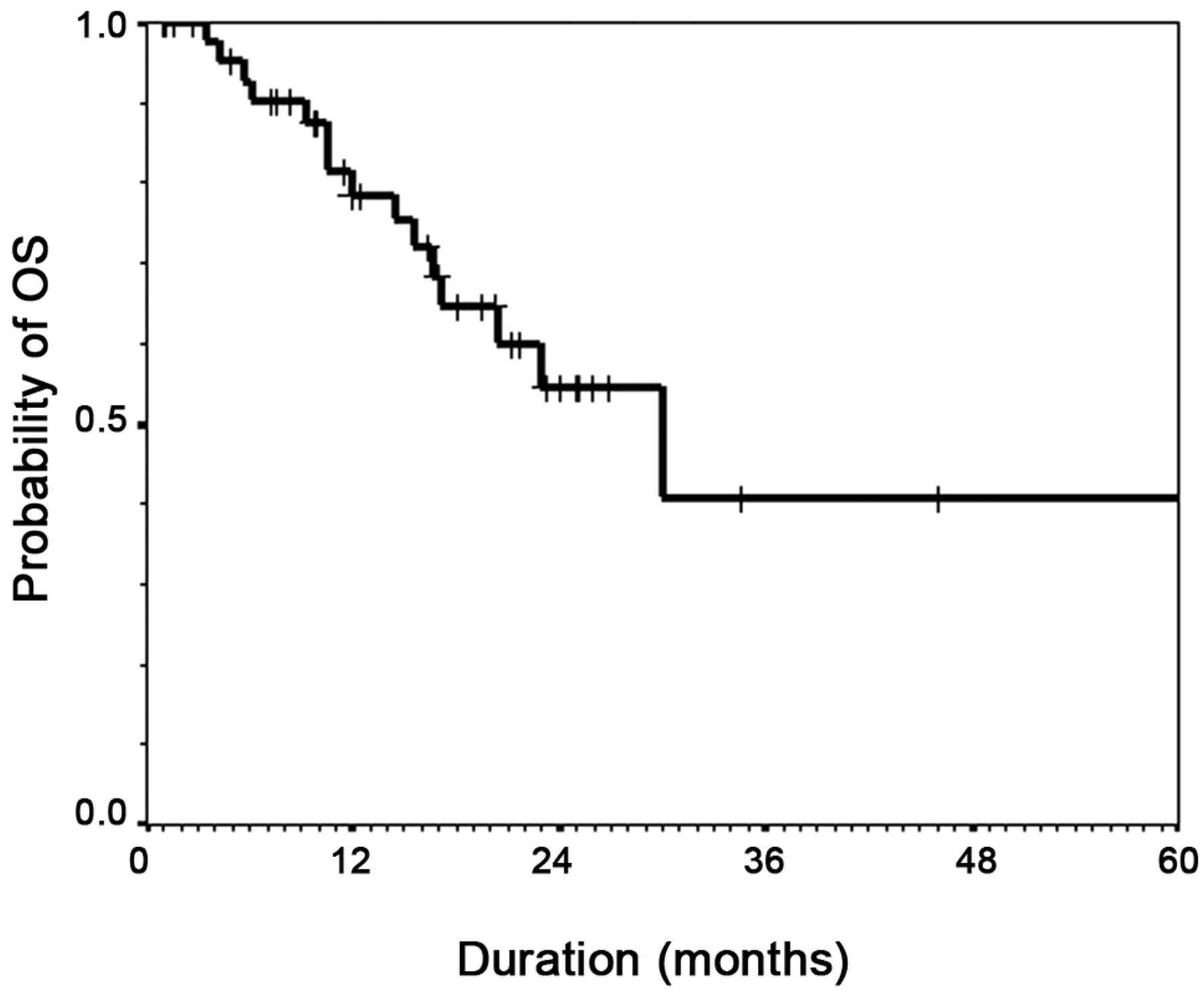
Eighteen out of 47 patients (38.3%) died during the period of this analysis. Of these 18 patients, 16 died of pancreatic cancer and the remaining 2 died without any sign of clinical recurrence (1 died of concurrent disease, 1 died of unknown cause). The 2-year actuarial PFS rate and the median time to progression for all 17 patients were 33.5% and 12.2 months, respectively (Figure 1). Table V indicates the metastasis-free rates according to various potential factors. Chemotherapy use significantly influenced the metastasis-free rates, while CA19-9, pathological T stage, pathological N stage, degree of resection and total radiation dose did not influence the metastasis-free rate. Figure 3 indicates the OS curves for all 47 patients. The median survival time and the 2-year actuarial OS rate in all 47 patients were 30.0 months and 54.5%, respectively. Concerning the use of chemotherapy, patients treated with chemotherapy had significantly higher OS rate than those treated without chemotherapy (p=0.0454) and the 2-year OS rates in patients treated with chemotherapy and those treated without chemotherapy were 61.6% and 25.0%, respectively (Figure 4). On univariate analysis, chemotherapy use alone had a significant impact on OS and on multivariate analysis, chemotherapy use also was a significant prognostic factor (Tables VI and VII). Other factors such as tumor size, PS and total radiation dose did not influence OS.

Local control (LC) and progression-free survival (PFS) curves for 47 patients with pancreatic cancer who were treated with gross complete resection and postoperative external beam radiotherapy (EBRT).
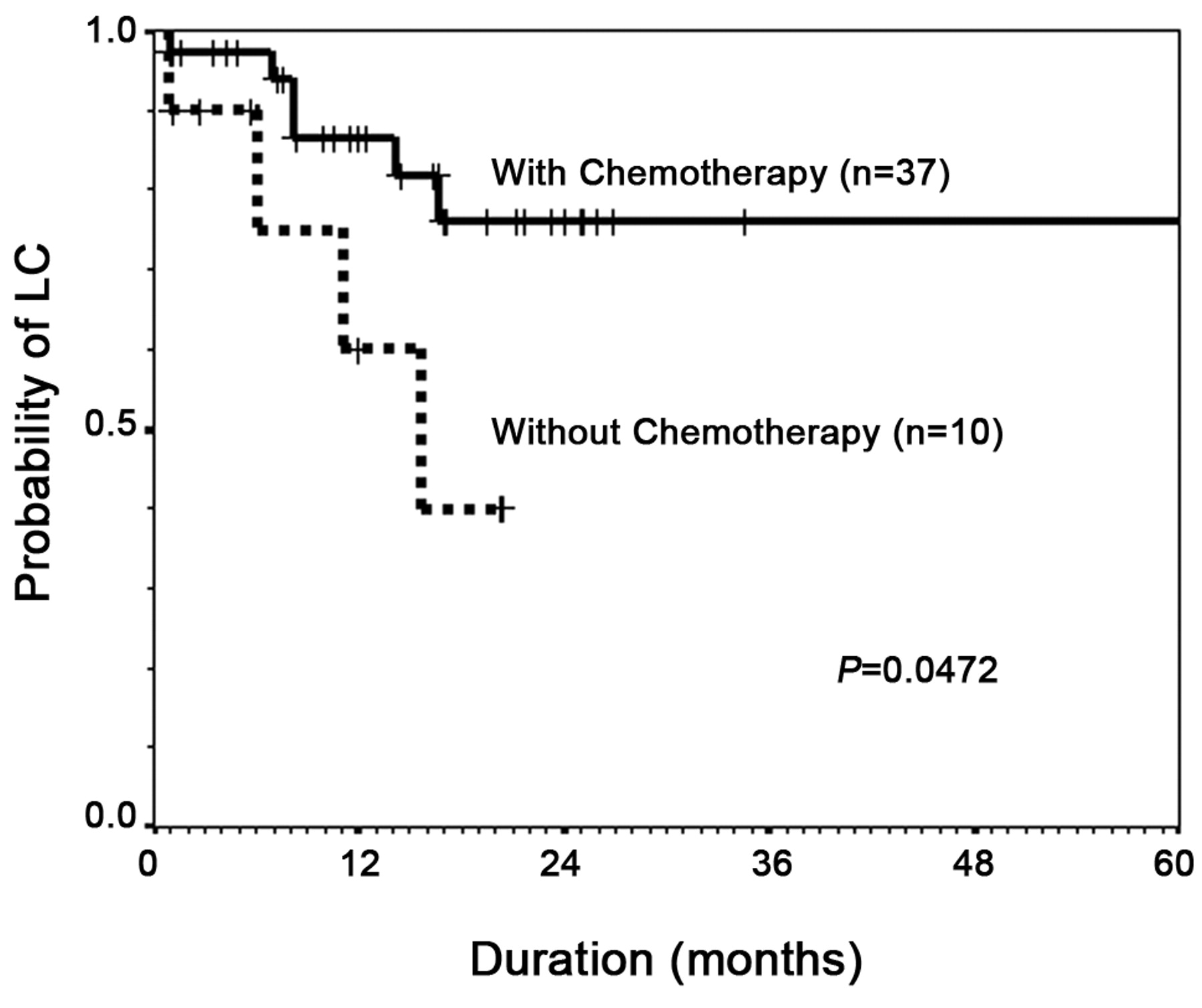
Local control (LC) curves according to chemotherapy use in patients with pancreatic cancer who were treated with gross complete resection and postoperative external beam radiotherapy (EBRT). A significant difference in LC was observed between chemotherapy use and no chemotherapy use (p=0.0472).
Local control rates (LCR) and metastasis-free rates (MFR) according to the CAA19-9 level, pathological T stage, pathological N stage, degree of resection, total radiation dose and chemotherapy use.

Actuarial overall survival (OS) curves for 47 patients with pancreatic cancer who were treated with gross complete resection and postoperative external beam radiotherapy (EBRT).

Actuarial overall survival (OS) curves according to chemotherapy use in patients with pancreatic cancer who were treated with gross complete resection and postoperative external beam radiotherapy (EBRT). A significant difference in OS was observed between chemotherapy use and no chemotherapy use (p=0.0454).
Univariate analysis of various potential prognostic factors for overall survival in patients with resected pancreatic cancer treated with postoperative EBRT.
At the time of this analysis, 1 out of 47 patients (2.1%) had survived for more than 5 years and LC had been maintained. Concerning the adverse effects, there were no late morbidities of NCI-CTC grade 3 or greater in any of the 47 patients.
Discussion
The current study indicates that postoperative EBRT with chemotherapy yields a favorable LC rate for resected pancreatic adenocarcinoma, with a 2-year LC rate of 76.0%. Several reports have also demonstrated the efficacy of postoperative EBRT with chemotherapy on LC (20, 21). Whittington et al. treated 20 patients with resected pancreatic adcenocarcinoma by adjuvant radiotherapy and 5-FU chemotherapy, and local recurrence occurred in only 25% of the patients (20). On the other hand, in the current study, the LC in patients treated with EBRT alone was significantly lower (2-year LC rate: 40%) compared to LC in patients treated with EBRT and chemotherapy. Therefore, our results strongly suggest that EBRT does not appear to be effective in preventing local recurrence. Concerning EBRT alone, approximately 40-50% of patients treated with adjuvant EBRT have been reported to develop local recurrence even after complete resection (4, 6, 22). Considering the lower LC rate in patients treated with EBRT alone, postoperative EBRT in addition to chemotherapy appears to be a reasonable treatment option to achieve LC in patients with resected pancreatic adenocarcinoma.
Although the efficacy of postoperative EBRT with chemotherapy for LC is apparent, the optimal use of EBRT, such as appropriate radiation dose and field, remains unclarified. The NCCN guidelines have recommended that postoperative radiotherapy should be administered at a dose of 45-54 Gy (1.8-2.0 Gy/day) (23). However, the standard dose (45-54 Gy) of postoperative radiotherapy alone did not seem to be effective in preventing local recurrence in the current study. Bosset et al. treated 14 patients with 54 Gy postoperative radiotherapy alone, but found a 50% incidence of local recurrence (22). If microscopic residual disease exists after gross total resection, the EBRT dose necessary to accomplish local control appears to be 60 Gy or more in 1.8-2 Gy fractions (24). However, radiation doses of 60 Gy or more may have higher risks of late complications. Therefore, additional therapies, such as adjuvant chemotherapy, are required to improve LC in patients with resected pancreatic cancer when treated with 45-54 Gy EBRT.
Concerning the extent of the radiation field, our results indicated that for approximately 45% of patients, the primary tumor bed only was treated with EBRT. Although the optimal radiation field for pancreatic cancer remains to be defined, the NCCN practice guidelines have recommended that when 5-FU-based chemoradiotherapy is used, the treatment volumes should include the primary tumor location and the regional lymph nodes (23). However, in the current study, most patients were treated with GEM, and several reports have indicated that the rate of severe toxicity is greater in patients treated with GEM-based chemoradiotherapy than in those treated with 5-FU-based chemoradiotherapy (25). Additional studies investigating the optimal radiation field when using chemotherapy drugs, such as GEM, should be conducted.
Despite the relatively favorable LC rates in patients treated with EBRT and chemotherapy, the role of EBRT and chemotherapy on survival for these patients remains controversial (7-10, 20-25). The Gastrointestinal Tumor Study Group (GITSG) conducted a randomized trial, and the median survival for the chemoradiotherapy group (20 months) was significantly longer than that for the observation group (11 months) (7). In contrast, recent randomized trials conducted by the European Organization for Research and Treatment of Cancer (EORTC) and the European Study Group for Pancreatic Cancer (ESPAC-1) have shed doubt on the benefit of adjuvant chemoradiotherapy (8, 9). In addition, the Pancreatic Cancer Meta-analysis Group reviewed the patient data from several randomized trials, and their results did not identify a survival advantage or disadvantage for adjuvant chemoradiotherapy, but they did report an improvement in survival with adjuvant chemotherapy (10). Therefore, it is important to evaluate possible factors affecting the prognosis of patients who receive EBRT and chemotherapy.
Multivariate analysis of potential prognostic factors for overall survival in patients with resected pancreatic cancer treated with postoperative radiotherapy.
Several previous studies have suggested potential prognostic factors associated with OS, such as tumor size, negative lymph nodes, negative CA19-9 and degree of resection in patients treated with macroscopically gross resection (20, 24, 26, 27). In the current study, chemotherapy use alone was an independent prognostic factor for OS. Moreover, chemotherapy use significantly affected the metastasis-free rate. Therefore, our results indicate that distant metastasis remains as the major problem negatively affecting survival in these patients. Several other reports have indicated that the local and distant recurrence rates vary from 12%-50% and 42%-94%, respectively, for patients with resected tumors treated with gross complete resection and radiotherapy (28-31). Therefore, in addition to achieving local control, preventing distant metastasis is necessary for improving the prognosis of patients with resectable pancreatic cancer.
Our results indicated that EBRT combined with chemotherapy confers a survival benefit on pancreatic cancer patients compared to EBRT alone. The use of chemotherapy also reduced the metastasis-free rate, suggesting that chemotherapy may prevent distant metastasis of these tumors. Therefore, adjuvant EBRT alone was insufficient for resected pancreatic cancer. Recent reports have indicated that adjuvant radiotherapy and chemotherapy improves survival after surgery when compared with patients with observation alone (11, 12). Herman et al. analyzed 908 patients who were treated with pancreaticoduodenectomy and found that adjuvant concurrent 5-FU-based chemotherapy and radiotherapy significantly improves OS when compared with patients not receiving chemotherapy and radiotherapy (11). Corsini et al. evaluated the results of 472 patients treated with R0 resection, and OS was better in patients who received adjuvant chemotherapy and radiotherapy than those not receiving chemotherapy and radiotherapy (12).
Regarding drugs for pancreatic cancer, 5-FU, with or without mitomycin-C, has been frequently used for therapy of pancreatic cancer (32, 33). Recently, single-agent GEM was found to be marginally superior in clinical benefit and survival compared to 5-FU, and a single-agent GEM has become the standard first-line agent for the treatment of pancreatic cancer (34). More recent reports have indicated that S-1 and UFT are promising agents for pancreatic cancer (35, 36). Timing of chemotherapy has also become a major concern for these patients. Although adjuvant chemoradiotherapy is often tried, an alternative approach to delivering adjuvant chemoradiotherapy, which should be evaluated further, is as preoperative treatment. Recent reports have indicated the favorable results using neoadjuvant chemotherapy with median survivals of 18-22 months for patients with resectable tumors (37, 38). Further evaluations of optimal timing of radiotherapy and chemotherapy should be performed to optimize treatment outcomes for patients with resected pancreatic cancer.
Concerning the long-term survival, one patient (2.1%) in our series survived for more than 5 years and LC was achieved for this patient. Recent reports have also indicated that achieving LC is associated with improved survival for patients with resected tumors (39, 40). Valentini et al. indicated that patients with achieving LC had significantly favorable OS (3-year OS: 28.4%) than patients without achieving local control (3-year OS: 11.9%) for patients with resected tumors (39). These results suggested that while metastasis still remains a primary treatment challenge for treatment of pancreatic cancer, improvement of LC with EBRT may improve survival of patients with less disseminated diseases.
In the current study, the frequency of severe late toxicity was 0%, highlighting the safety of combined EBRT and chemotherapy. Several reports have also described the feasibility of radiotherapy for long-term survivors of pancreatic cancer (11, 12). Further studies are required to determine the optimal timing and dose of EBRT in this setting.
In conclusion, our results indicated that postoperative EBRT with chemotherapy yields a favorable LC rate for patients with resected pancreatic cancer without causing severe late toxicity. Our results also suggest that EBRT combined with chemotherapy confers a survival benefit compared to EBRT alone. Therefore, we conclude that EBRT alone is insufficient, and EBRT combined with chemo-therapy appears to be theadjuvant treatment of choice after gross complete resection. However, this study was a retrospective one with various treatment modalities, and further prospective studies are required to confirm our results.
Footnotes
-
Conflict of Interest
There is no conflict of interest regarding the study.
- Received February 22, 2010.
- Revision received May 21, 2010.
- Accepted May 27, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.