


Abstract
Background/Aim: The usefulness of C-reactive protein-to-albumin ratio (CAR) as a predictive indicator for clinically-relevant postoperative pancreatic fistula (CR-POPF) after pancreaticoduodenectomy (PD) is unclear. We performed a retrospective analysis to identify reliable inflammatory indicators for prediction of CR-POPF after PD. Patients and Methods: We enrolled 160 consecutive patients who underwent PD. Multivariate logistic regression analysis was performed. The areas under curves (AUCs) were compared with the discriminatory ability of inflammatory indicators, namely, C-reactive protein (CRP), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), platelet count multiplied by C-reactive protein (P-CRP), and CAR. Results: The AUC for CAR on POD 3 to predict CR-POPF was 0.782 (p<0.001) and higher than that for CRP (0.773), NLR (0.652), PLR (0.504), and P-CRP (0.703). Multivariate analysis revealed that CAR on POD 3 was an independent predictive indicator of CR-POPF. Conclusion: CAR on POD 3 is a reliable predictor of CR-POPF after PD.
Pancreaticoduodenectomy (PD) is a complex procedure associated with high morbidity and mortality and performed in patients with malignant or benign tumors of the pancreatic head and periampullary region. Despite recent dramatic advances in surgical techniques and developments in perioperative management, reported morbidity and mortality rates after PD are 41.56% and 2.88%, respectively, according to the national clinical database in Japan and other sources, and these rates are unsatisfactory (1-6). Postoperative pancreatic fistula (POPF) is the most frequent and clinically-crucial complication following PD. Clinically-relevant POPF (CR-POPF) sometimes triggers life-threatening complications such as postoperative intra-abdominal hemorrhage, intra-abdominal abscess, sepsis, and death (7-9). Therefore, accurate and rapid prediction of CR-POPF after PD is needed to decrease mortality secondary to serious complications and to optimize individual patient's treatment decisions.
The amylase level in pancreatic drainage fluid is a reliable predictive indicator for CR-POPF after PD (10, 11). However, it is sometimes difficult to predict CR-POPF by the measurement of drainage fluid amylase levels accurately because the concentration of amylase does not always reflect the severity of POPF (12). Systemic inflammatory responses are closely associated with surgical complications in various types of surgery (13-16). C-reactive protein (CRP), an inflammatory marker, is a well-recognized positive acute-phase nonspecific reactant synthesized by the liver that increases rapidly in response to inflammation and infection. CRP has been assessed as a predictive indicator of POPF (17-19). C-reactive protein-to-albumin ratio (CAR) is another inflammatory indicator calculated by dividing serum CRP by albumin levels, and has been correlated with poor prognosis in cancer patients and patients with sepsis (20, 21). Moreover, CAR is a useful biomarker for monitoring activity in systemic inflammatory disease (22); however, the usefulness of CAR as a predictive indicator of CR-POPF after PD remains unclear. Therefore, this study aimed to investigate the predictive significance of CAR for CR-POPF after PD compared with both CRP and other serum-based inflammatory indicators, namely, neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and platelet multiplied by CRP (P-CRP).
Patient clinical characteristics.
Patients and Methods
Patients. In this study, we retrospectively reviewed data from 160 consecutive patients who underwent PD for pancreatic head and periampullary disease at Tottori University Hospital between January 2008 and December 2017.
The study protocol was approved by the institutional review board of Tottori University (No. 17A135), and the requirement for informed consent was waived for this retrospective study.
Surgical procedures. All patients underwent subtotal stomach-preserving PD or pylorus-preserving PD. Reconstruction was performed by modified Child's reconstruction in subtotal stomach-preserving PD or a Traverso reconstruction in pylorus-preserving PD. Pancreases with soft parenchyma were divided using a scalpel or an ultrasonically-activated device, while hard pancreatic parenchyma was divided using an electric scalpel.
Pancreaticojejunostomy (PJ) was performed by a duct to mucosal, end-to-side anastomosis method using eight interrupted 5-0 polydioxanone sutures (PDS-II; Johnson and Johnson Co., Tokyo, Japan) with either an internal or external stent in the main pancreatic duct for drainage of pancreatic juice. In a seromuscular–parenchymal anastomosis, either Kakita's method or the modified Blumgart method was performed using 3-0 or 4-0 nonabsorbable sutures (23, 24). Hepaticojejunostomy was performed 10-15 cm distal to the PJ, followed by antecolic end-to-side gastro- or duodenojejunostomy with a Braun anastomosis. At the end of the operation, closed peritoneal drainage tubes were placed at the upper and lower side of the PJ and behind the hepaticojejunostomy after peritoneal lavage was performed using 8000 ml of normal saline.
Perioperative management. Prophylactic antibiotics were administered for 3 days, including the operation day, in all patients. Proton pump inhibitors were provided to patients throughout the postoperative course. Solid diets were started on postoperative day (POD) 4 regardless of amylase levels in the drainage fluid, if there were no serious postoperative surgical complications.
Amylase levels in the drainage fluid were routinely measured on POD 1 and 3. Similarly, bacterial culture and bacterial smear test of the drainage fluid were performed on POD 1 and 3. We removed peritoneal drainage tubes on POD 3 or 4, when the amylase levels in the drainage fluid were less than three times the upper limit of our institutional normal serum value or less than 1000 IU/l as an absolute value and bacterial smear test of the drainage fluid was confirmed negative on POD 3. We routinely used antibiotics and replaced the drains to prevent drainage failure secondary to occlusion of the drainage tract in patients with the possibility of developing CR-POPF; we removed the drains after complete PF recovery. Nasogastric tubes inserted intraoperatively were removed from all patients on POD 1.
POPF was diagnosed in accordance with the International Study Group Pancreatic Fistula classification (25). In the current study, we regarded grade B or C as CR-POPF and divided the patients into a CR-POPF group and a nonCR-POPF group.
Clinical variables. We retrospectively reviewed the following clinical variables evaluated in this study using patients' electronic medical records: age, sex, body mass index, histological diagnosis, preoperative serum albumin level, preoperative peripheral lymphocyte count, preoperative biliary drainage, texture of the pancreatic parenchyma, diameter of the main pancreatic duct (MPD), operation time, intraoperative blood loss volume, and type of PJ. We also collected data for CRP, NLR, PLR, P-CRP, and CAR on POD 1 and 3 as postoperative inflammatory indicators, from peripheral blood samples.
Patients' postoperative drain amylase concentrations and serum inflammatory parameters.
We calculated CAR by dividing serum CRP level by the peripheral serum albumin level. We calculated NLR and PLR by dividing the peripheral neutrophil count and the peripheral platelet count by the peripheral lymphocyte count, respectively. P-CRP was calculated by multiplying the peripheral platelet count by serum CRP level/104.
Statistical analysis. Continuous variables were expressed as means and deviations. Differences in clinical variables between the two groups were examined by the Chi-square test, Fisher's exact probability test, and the Mann–Whitney U-test. The areas under the curves (AUC) for the amylase level in the drainage fluid, CRP, NLR, PLR, P-CRP, and CAR regarding each measurement's ability to predict CR-POPF were evaluated using receiver operating characteristic (ROC) analysis. The optimal cutoff values for CAR and the amylase level in the drainage fluid were also calculated by ROC analysis. Univariate and multivariate logistic regression analyses were performed to clarify the predictive factors of CR-POPF after PD. Covariates with a p-value <0.1 in the univariate analysis were entered into the multivariate analysis. p<0.05 was considered significant. All statistical analyses were performed using SPSS software (Version 24; SPSS Inc., Chicago, IL, USA).
Results
CR-POPF occurred in 48/160 (30.8%) patients. Patients' characteristics in both the CR-POPF group and nonCR-POPF group are shown in Table I. There were significant differences between the two groups regarding sex, historical diagnosis, texture of the pancreatic parenchyma, and type of PJ. The body mass index of patients in the CR-POPF group was significantly higher compared with patients in the nonCR-POPF group. The diameter of the MPD in patients in the CR-POPF group was significantly shorter than that of patients in the nonCR-POPF group. We observed no significant differences in preoperative serum albumin level and peripheral lymphocyte count, reflecting preoperative nutritional status, between the two groups.
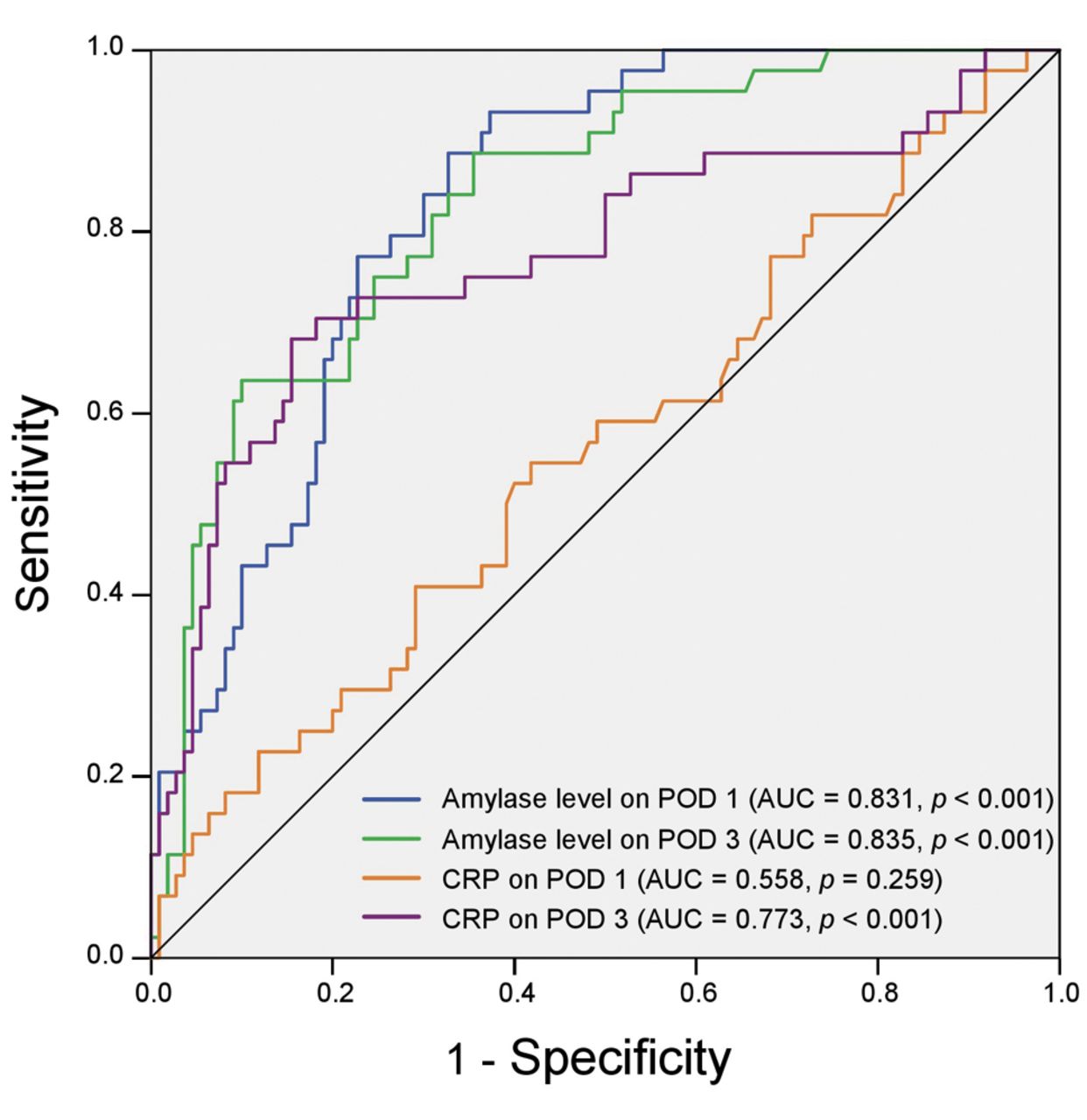
Table II summarizes the postoperative findings of the drain amylase concentrations and serum inflammatory parameters in the patients in the current study. Amylase levels in the drainage fluid on both POD 1 and 3, and CRP, NLR, P-CRP, and CAR on POD 3 in patients in the CR-POPF group were significantly higher than those in patients in the nonCR-POPF group. ROC analysis regarding the prediction of CR-POPF revealed that the AUCs for serum CRP level and amylase level in the drainage fluid on POD 3 were 0.773 (p<0.001) and 0.835 (p<0.001), respectively. In contrast, AUCs for values on POD 1 were 0.558 (p=0.259) and 0.831 (p<0.001), respectively, which were lower than those on POD 3 (Figure 1).
The discrimination ability of CAR to predict CP-POPF, estimated by AUC, was 0.782 (p<0.001), which was the highest value among all inflammatory indicators on POD 3 (CRP: 0.773, p<0.001; NLR: 0.652, p=0.003; PLR: 0.504, p=0.943; and P-CRP: 0.703, p<0.001) (Figures 1 and 2). In the ROC analysis, the highest Youden indices (sensitivity + specificity - 1) showed the optimal cutoff value of CAR on POD 3 to be 7.4. Based on this result, we grouped patients as CARHigh (CAR ≥7.4; n=43) or CARLow (CAR <7.4; n=113). Table III shows the relationship between CAR and the clinical characteristics of patients who underwent PD. Significant differences were observed between CAR and sex (p=0.026), pancreatic parenchymal texture (p<0.001), MPD diameter (p<0.001), amylase level in the drainage fluid on POD 3 (p<0.001), and CR-POPF (p<0.001).

Receiver operating characteristic curves for serum CRP levels and amylase levels in drainage fluid on POD 1 and 3 to predict clinically-relevant postoperative pancreatic fistula in patients who underwent pancreaticoduodenectomy. CRP: C-reactive protein; AUC: area under the curve; POD: postoperative day.
Multivariate logical regression analyses revealed that CAR on POD 3 was an independent predictive factor of CR-POPF after PD, along with amylase level in the drainage fluid on POD 3 (Table IV).
Discussion
Our results showed that CAR was the most reliable indicator for predicting CR-POPF following PD among the inflammatory indicators evaluated. CR-POPF is a serious complication and causes potentially life-threatening complications that can lead to sepsis secondary to intra-abdominal abscess, or postpancreatectomy hemorrhage (26, 27). CR-POPF leads to prolonged hospital stay and increased medical costs. Furthermore, CR-POPF causes a poor prognosis in patients with malignant disease secondary to depleted systemic immune function or delayed administration of adjuvant therapy (28, 29). Because no definitive methods exist to completely prevent CR-POPF, despite several studies, accurate and reliable prediction of CR-POPF in the early postoperative period after PD is needed to prevent these complications.

Receiver operating characteristic curves for CAR, P-CRP, NLR, and PLR on POD 3 to predict clinically postoperative pancreatic fistula in patients who underwent pancreaticoduodenectomy. CAR: C-reactive protein-to-albumin ratio; P-CRP: platelet multiplied by CRP; NLR: neutrophil-to-lymphocyte ratio; PLR: platelet-to-lymphocyte ratio; POD: postoperative day; AUC: area under the curve.
Drain amylase concentration is the most well-known predictive indicator for CR-POPF (11). Several reports have indicated that high amylase levels in the drainage fluid, perioperatively, are an independent predictive risk factor for CR-POPF (10, 30). Our results confirmed that the amylase level in the drainage fluid was an independent predictive indicator for CR-POPF after PD. However, in contrast, one study reported that the amylase level in the drainage fluid does not always reflect the clinical severity of POPF (12). This may be because amylase consists of glycolytic enzymes and does not damage tissues directly as with pancreatic peptidases; one study reported a nonparallel correlation in secretion between amylase and pancreatic peptidases (31). As another reason, measuring the amylase level has the shortcoming of being susceptible to the location or condition of the inserted peritoneal drainage tube, and evaluating CR-POPF might not be performed correctly due to drain migration and obstruction. Therefore, it is desirable to predict CR-POPF using objective surrogate markers unaffected by the surgical procedure.
CRP is a positive acute-phase reactant synthesized by the liver and a hallmark of systemic inflammation that is widely used as a blood marker in medical treatment (17). Serum CRP levels generally increase acutely in response to inflammation and infection and peak at approximately 48-72 h (32). Several reports have shown that serum CRP level on POD 3 is a useful indicator for predicting CR-POPF after PD (18, 33). Our results confirmed that serum CRP levels on POD 3 in patients with CR-POPF were significantly higher than levels in patients with nonCR-POPF, which supports the close relationship between CRP on POD 3 and CR-POPF. However, individual differences in the distributions of serum CRP levels have been noted, related to genetic or environmental factors (34). Moreover, there is a significant association between regulation of serum CRP levels and polymorphisms in the promoter of interleukin-6 (34). Because of these individual differences, CRP alone might not accurately predict CR-POPF.
Comparison of the clinical variables in the CARHigh group and CARLow group in patients who underwent PD.
Univariate and multivariate analyses of predictive indicators for CR-POPF in patients undergoing PD.
CAR, calculated by dividing the serum CRP level by the serum albumin level, is a new inflammatory indicator that is widely used as a prognostic indictor in various cancers as well as in inflammatory disease (35, 36). Albumin is a negative acute-phase reactant, and its level in the blood decreases in response to the degree of inflammation during catabolism, and hypoalbuminemia is associated with inflammation severity, disease prognosis, and mortality (37, 38). Therefore, CAR reflects acute inflammatory intensity, incorporating individual differences, by dividing CRP by albumin. In fact, CAR was reportedly superior to CRP level in predicting mortality in patients with septic shock (21). In the current study, we demonstrated that the AUC of CAR on POD 3 was the best predictor of CR-POPF among the inflammatory indicators, including CRP on POD 3, and that CAR was an independent predictive indicator of CR-POPF.
Platelets are implicated in many pathophysiological processes including inflammation and immunity (39). However, different from acute inflammatory reactants such as CRP or albumin, platelet numbers begin to increase after peak inflammation (40). Platelets are consumed during hemostasis secondary to intraoperative bleeding or platelet aggregation in the acute inflammatory phase in highly-invasive surgeries such as PD. Therefore, inflammatory indicators based on the platelet count, such as PLR and P-CRP, are unsuitable to predict CR-POPF following PD early postoperatively, before peak inflammation.
The present study has limitations, including that this was a retrospective analysis with a limited number of enrolled patients, which generated bias. Additionally, although we measured CAR on POD 1 and 3, only, the optimal time to measure CAR remained unclear. Other inflammatory indicators, such as the albumin-to-fibrinogen ratio, red cell distribution width and, the mean platelet volume, in addition to the five inflammatory indicators verified in this study, should be estimated to identify the true reliable predictive indicators for CR-POPF after PD.
In conclusion, based on our result, CAR on POD 3 was a reliable predictive indicator of CR-POPF after PD. Furthermore, accurately and quickly predicting CR-POPF after PD using CAR may prevent life-threatening complications and provide optimal individual patient treatment.
Acknowledgements
The Authors would like to thank Jane Charbonneau, DVM, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
Footnotes
Authors' Contributions
Study concepts: Teruhisa Sakamoto; Study design: Teruhisa Sakamoto; Data acquisition: Takuki Yagyu, Ei Uchinaka, Masaki Morimoto, and Takehiko Hanaki; Quality control of data and algorithms: Joji Watanabe; Data analysis and interpretation; Teruhisa Sakamoto and Naruo Tokuyasu; Statistical analysis: Teruhisa Sakamoto; Manuscript preparation: Teruhisa Sakamoto; Manuscript editing: Soichiro Honjo; Manuscript review: Yoshiyuki Fujiwara; Final approval of the article, all Authors.
Conflicts of Interest
The Authors have no conflicts of interests to declare regarding this study.
- Received October 13, 2019.
- Revision received October 23, 2019.
- Accepted October 24, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}