


Abstract
Background/Aim: For patients undergoing cancer surgery, the risk for cancer progression is enhanced during the perioperative period. To what extent the type of anesthetic can affect the metastatic process and finally the outcome of patients with cancer is under debate. For this reason, the aim of this study was to investigate the effects of the volatile anesthetics sevoflurane and desflurane on colon cancer cells in vitro. Materials and Methods: SW480 colon carcinoma cells were exposed for 3 or 6 h to sevoflurane (1 or 2.5 vol%) or desflurane (6 or 12 vol%). Cell cycle distribution was analyzed by flow cytometry after a 24-72 h recovery and apoptosis was detected by annexin V staining after a 0-48 h recovery. Viability was tested by measuring ATP content after 0 and 24 h recovery. Results: Treatment with sevoflurane or desflurane caused no or only slight changes in cell-cycle distribution and apoptosis rate. Desflurane at 12vol% significantly reduced cell viability by 17±25% and 11±22% after 3 and 6 h incubation and 24 h recovery, respectively, while 2.5 vol% sevoflurane slightly increased viability. Conclusion: At clinically relevant concentrations, sevoflurane and desflurane had only slight effects on SW480 colon cancer cells in vitro.
For patients undergoing cancer surgery, the risk for cancer dissemination and metastasis is supposed to be enhanced during the perioperative period (1, 2). Cancer cells are released into the circulation due to traumatization of tumor vessels and surgical manipulation of the tumor tissue (3). Increased levels of growth factors and an imbalance between pro- and anti-angiogenic factors can be detected during the wound-healing process (4). At the same time, impairment of the immune response occurs for several days after cancer surgery (1).
Anesthesia as well as surgical trauma activates the neuroendocrine stress response by stimulating the hypothalamic–pituitary–adrenal axis and the sympathetic nervous system, leading to increased levels of immunosuppressive factors such as catecholamines, glucocorticoids and prostaglandins (5). With reduced numbers of natural killer cells, cytotoxic T-cells and T-helper cells, cell-mediated immunity is attenuated (6). For this reason, the growth of disseminated cancer cells and micrometastases can be fostered during the perioperative period.
Usually anesthesia is induced by the administration of intravenous anesthetics and maintained either by volatile anesthetics or as total intravenous anesthesia. Balanced anesthesia that combines several agents to achieve unconsciousness, amnesia, analgesia and muscle relaxation, and minimization of adverse effects by reducing the dosage of the single agents is a well-established anesthesia regime (7). In terms of a multimodal pain therapy management, opioid analgesics are often combined with other agents such as ketamine and non-opioide-analgesics (8). If applicable, regional anesthetic techniques such as epidural anesthesia, paravertebral blockade or blockade of peripheral nerves are applied to improve intra- and postoperative pain management (8).
It remains unknown whether the application of a special anesthesia regime or agents can affect cancer recurrence and oncological outcome. A large number of preclinical and clinical studies are currently addressing this issue. The aim of this study was to investigate the effects of the volatile anesthetics sevoflurane and desflurane on viability, apoptosis and cell-cycle distribution of SW480 colon cancer cells in vitro.
Materials and Methods
Reagents. Commercially available sevoflurane (Sevorane®; Abbvie, Ludwigshafen, Germany) and desflurane (Suprane®; Baxter, Unterschleißheim, Germany) were used for this study.
Cell line. SW480 colon carcinoma cell line was purchased from the German Collection of Microorganism and Cell Culture (DSMZ, Braunschweig, Germany). RPMI 1640 medium (Pan Biotech, Aidenbach, Germany) contained 10% fetal calf serum (Sigma–Aldrich, Steinheim, Germany), 2 mM sodium pyruvate (Appli Chem, Darmstadt, Germany) and 2 mM L-glutamine (Sigma–Aldrich) and was supplemented with 5% penicillin plus streptomycin (Sigma–Aldrich). Cells were maintained in monolayer culture and were cultured in a humidified CO2 atmosphere (5%) at 37°C. Experiments were performed when cells reached ~80% confluence.
Exposure to volatile anesthetics. SW480 (2.5-3×105) cells were seeded in 25-cm2 cell culture flasks (BD Falcon, Heidelberg, Germany) and allowed to attach for 2-3 days.
Cells were exposed to sevoflurane (1 or 2.5 vol%) or desflurane (6 or 12 vol%) for a period of 3 or 6 h. A modified anesthesia unit (Trajan 808; Draeger, Lübeck, Germany) was used as described previously (9). Anesthesia gas vaporizers were installed for the evaporation of sevoflurane (Vapor Sevorane®; ABBOTT Draeger, Lübeck, Germany) or desflurane (Vapor Devapor; Draeger). The gas mixture (95% air and 5% CO2 plus 1 or 2.5 vol% sevoflurane or 6 or 12 vol% desflurane) was continuously monitored using a Capnomak Ultima monitor (Datex Engstrom, Fairfield, CT, USA). In addition, sevoflurane and desflurane concentration dissolved in culture medium was detected by gas chromatography. Cells were maintained at 37°C by placing the cell-culture flasks on feedback-regulated heated gel pads. To prevent protein binding of volatile anesthetics, standard growth medium was replaced by serum-free medium in all groups (including controls) during anesthetic exposure. After exposure, cells were washed once and incubated with standard growth medium and cells were returned into the incubator for recovery.
Cell-cycle analysis. Cell-cycle profiles were analyzed by flow cytometry after treatment with sevoflurane (1 or 2.5 vol%) or desflurane (6 or 12 vol%) and a 24- to 72-h recovery. Standard culture medium was used for negative control and 5 mM acetylsalicylic acid (ASS) (Sigma–Aldrich) was used for positive control. Cells were harvested by standard trypsinization and washed twice with cold phosphate-buffered saline (PBS)/1% fetal calf serum. Cells (2.5×105) were fixed with 70% methanol at room temperature and stored at 4°C. For measuring, the cells were washed twice with PBS and treated with 1 mg/ml RNase A. After a 20-min incubation at room temperature in the dark, cells were stained with 100 μg/ml propidium iodide (PI) (Sigma–Aldrich). For each sample, 104 cells were measured by flow cytometry using FACS Calibur (BD Bioscience, Franklin Lakes, NJ, USA) driven by the CellQuest Software (BD Bioscience). The cell-cycle distribution was assessed using ModFit LT 3.2 software (Verity Software House, Topsham, ME, USA). All tests were performed as at least three independent experiments.
Apoptosis analysis. Apoptosis rate was measured after treatment with sevoflurane (1 or 2.5 vol%) or desflurane (6 or 12 vol%) and 0-48 h recovery. Staurosporine (1 μM; Sigma Aldrich) was used as a positive control. Floating cells were preserved by decanting supernatant. Adherent cells were rinsed with PBS (37°C) (Sigma–Aldrich) and detached by standard trypsinization. Fluorescein isothiocyanate Annexin V Apoptosis detection Kit (BD, Heidelberg, Germany) was used according to the manufacturer's protocol as described previously, PI staining was used for the exclusion of necrotic cells (10). All tests were performed in duplicates as at least three independent experiments. For data analysis, Flowjo v10.0.7 (BD, Ashland, OR, USA) was used.
Cell viability. Cell viability was measured by the Glo Lumninescent assay (Cell Titer Glo Luminescence) (Promega, Madison, WI, USA) according the manufacturer's protocol. SW480 colon cancer cells (4×104) were seeded in six 24-well plates and allowed to attach for 2-3 days. Standard growth medium was replaced by serum-free medium and plates were incubated for 0, 3 or 6 h with 2.5 vol% sevoflurane or 12 vol% desflurane. Three wells were used for each control, 3 h and 6 h incubation time and 0 and 24 h recovery time (separate plates). Cell viability was analyzed directly after incubation and after 24 h recovery time. Cell Titer Glo reagent (285 μl) was added to each experimental well of the 24-well plate containing 285 μL culture medium and contents were mixed for 2 min to induce cell lysis. The content was transferred to 5 wells of a 96-well plate with 100 μl per well and allowed to incubate at room temperature for 15 min. Luminescence signal was detected by a Varioskan Flash (Thermo Fisher Scientific, Waltham, MA, USA) multiplate reader using Skanit 2.4.5 software (Thermo Fisher Scientific). For data analysis, an ATP (Sigma) standard curve was generated. All experiments were performed in triplicates as three independent experiments.
Statistical analysis. Results are expressed as the mean±standard deviation (SD). For comparison between mean values, the non-parametric Mann–Whitney U-test was used. Differences were considered statistically significant at p<0.05. IBM SPSS Statistics V 21 (IBM, New York, NY, USA) and Excel 2010 (Microsoft, Redmond, Washington, USA) packages were employed for statistical analysis.
Results
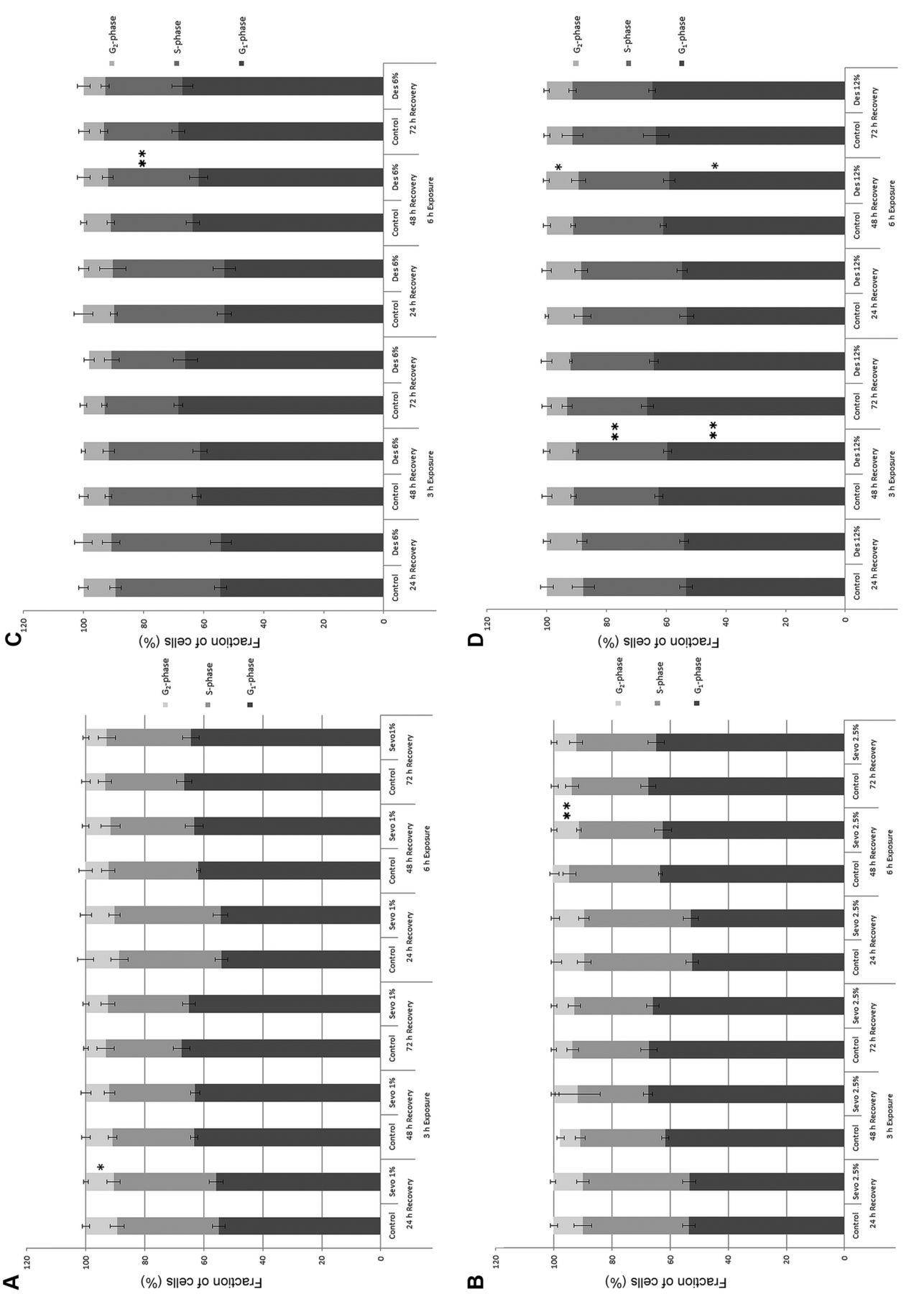
Cell-cycle analysis. After exposure to sevoflurane or desflurane, only slight changes in the cell-cycle distribution were detected. In SW480 cells exposed to 1 vol% sevoflurane for 3-h and 24-h recovery, the fraction of cells in G2 phase significantly decreased from 10.6±1.3% to 9.4±0.8% compared to the untreated control (p<0.05) (Figure 1A). After 6 h of exposure to 2.5 vol% sevoflurane, a significant increase in G2 phase cells was detected compared to the untreated control from 5.8±0.5% to 8.6±1.7% after 48 h and from 6.1±0.8% to 7.6±0.6% after 72 h recovery (p<0.01) (Figure 1B). In cells treated with 6 vol% desflurane for 6 h or 12 vol% for 3 h, an increase in S-phase cells from 27.4±1.3% to 30.2±1.8% and 28.5±0.9% to 30.7±0.9% respectively, compared to the corresponding control cells, was detected after a 48-h recovery (p<0.01) (Figure 1 C and D). A significant decrease in G1-phase cells occurred in cells exposed to 12% desflurane for 3 or 6 h followed by a 48-h recovery time from 62.5±1.3% to 59.6±1.4% and 61.1±1.0% to 59.0±to 1.9% respectively (p<0.05) (Figure 1D).

Effect of volatile anesthetics on cell-cycle distribution. SW480 cells were exposed for 3 or 6 h to sevoflurane (Sevo) at 1 vol% (A) or 2.5 vol% (B), or desflurane (Des) at 6 vol% (C) or 12 vol% (D). Cell-cycle profiles were determined by flow cytometry after 24-72 h recovery. Significantly different at *p<0.05 and **p<0.01 compared to the untreated control. Data are given as the mean±SD percentage of cells.
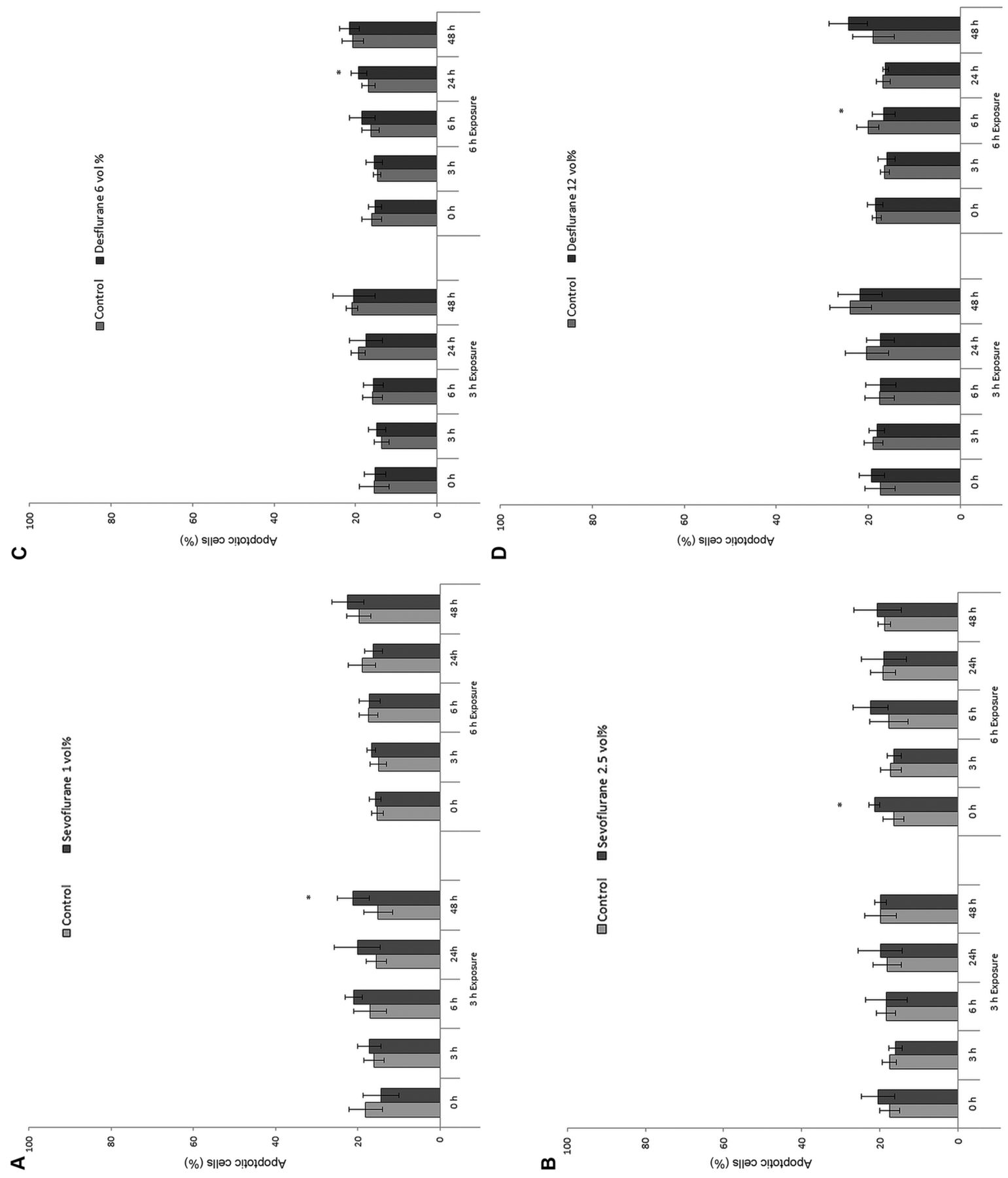
Effect of volatile anesthetics on apoptosis rate. SW480 cells were exposed for 3 or 6 h to sevoflurane at 1 vol% (A) or 2.5 vol% (B), or desflurane (Des) at 6 vol% (C) or 12 vol% (D). Apoptosis was detected by annexin V staining after 0-48 h recovery. *Significantly different at p<0.05 compared to the untreated control. Data are given as the mean±SD percentage of cells.
Apoptosis analysis. Compared to the untreated control, a statistically significant increase in apoptosis (15.0±3.6% to 21.1±3.9%, p<0.05) was detected after a 3-h exposure to sevoflurane (1 vol%) and a 48 h recovery (Figure 2A), as well as immediately after incubation with 2.5 vol% sevoflurane for 6 h (16.5±2.7% to 21.4±1.3%) (Figure 2B).
For cells incubated with desflurane 6 vol% for 6 h, the apoptosis rate increased significantly from 14.1±1.4% to 16.4±1.9% after 24 h recovery (Figure 2C). However, a significant reduction of apoptotic cells was detected after 6 h of exposure to 12 vol% desflurane and a 6-h recovery, from 20.1±2.5% to 16.6±2.5% (p<0.05) (Figure 2D). No significant changes in apoptosis rate were detected after exposure to sevoflurane or desflurane at any other timepoints.
Cell viability. Incubation with 2.5vol% sevoflurane for 3 h increased cell viability by 8±17% and 4±13% respectively (Figure 3A). However, after 6-h incubation, no significant changes in ATP content were detected. Incubation with 12% desflurane for 3 and 6 h significantly reduced viability after a 24-h recovery by 17±25% and 11±22%, respectively (Figure 3B).
Discussion
Sevoflurane and desflurane are volatile anesthetics usually used for balanced anesthesia (7). A common tool to describe the anesthetic potency of volatile anesthetics is the minimal alveolar concentration (MAC) which is required to avoid movement to a surgical stimulation in 50% of patients, referred to as MAC 50% (11). For desflurane, MAC 50% is 6 vol% and for sevoflurane 2.05 vol% in oxygen (12). MAC decreases with increasing age and in combination with other depressive agents such as opioids and benzodiazepines (11).
The mechanism of action of volatile anesthetics has not been fully elucidated. For a long time, interaction with the lipid of the cell membrane was purported to be the mechanism of action (12). Later, the involvement of proteins was discussed and, in recent years, binding sites for anesthetics have been detected in different ion channels such as nicotinic acetylcholine, glycine, N-methyl-D-aspartate (NMDA), α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) and serotonin receptors (12).
In this study, we only detected no or slight effects on cell proliferation and viability of SW480 cells upon incubation with sevoflurane and desflurane for 3 or 6 h. These changes were quite small sporadic differences between the groups which did not follow any pattern. For this reason, we do not judge these changes to be a specific effect of sevoflurane or desflurane.

Effect of volatile anesthetics on cell viability. SW480 cells were exposed for 3 or 6 h to 2.5 vol% sevoflurane (A), 12 vol% desflurane (B). Cell viability was detected by ATP assay a 0 or 24 h recovery time. Significantly different at *p<0.05 and **p<0.01 compared to the untreated control. Data are given as the mean±SD percentage of cells.
In SW620 and HCT116 colon carcinoma cells, incubation with 1-4% sevoflurane for 6 h caused little change in cell viability measured by MTT test. However, inhibition of cell invasion and migration was detected (13).
Results from several studies show inconsistent effects of volatile anesthetics on cell proliferation, apoptosis and metastatic potential. In A549 lung cancer cells, incubation with sevoflurane enhanced apoptosis, increased apoptotic bodies, impaired DNA integrity (14) and caused changes in apoptosis-related miRNAs (15). Liang and colleagues showed apoptosis induction and inhibition of cell proliferation, as well as anti-invasive and anti-migratory effects by sevoflurane via down-regulation of expression of matrix metalloproteinase (MMP)-2 and -9 (16). Furthermore, co-treatment with sevoflurane and the chemotherapeutic agent cisplatin caused synergistic growth inhibitory and anti-invasive effects (17). However, in another study, the incubation of A549 cells with 3.6vol% sevoflurane for 2 h reduced cell proliferation and increased chemosensitivity but did not affect migration (18). Interestingly, in the same study, the viability and metastatic potential, as well as the chemoresistance, of renal cell carcinoma cells was enhanced (18). Kvolik et al. showed increased apoptosis induced by sevoflurane in Caco 2 colon cancer cells but only moderate effects in laryngeal cancer cells (19). Moreover in head and neck squamous cell carcinoma, sevoflurane inhibited cell invasion and induced apoptosis (20). In contrast, isoflurane was shown to increase proliferation, reduce apoptosis and promote invasion in two head and neck squamous cell carcinoma cell lines (21). In addition, exposure to isoflurane, desflurane or sevoflurane for 2 h significantly increased the metastatic potency of SKOV-3 ovarian cancer cells by increasing levels of vascular endothelial growth factor A, MMP11 and transforming growth factor beta (22). Isoflurane furthermore caused cell-cycle progression and increased cell growth in ovarian (23) and prostate cancer (24) cells, and attenuated dynorphin-induced cytotoxicity in neuroblastoma cells (25).
In preclinical studies, incubation time ranged from 30 min (15) to 48 h (26); in many studies incubation times from 2 to 6 h were used (14, 20, 23, 24, 27). Concentrations used ranged from 1.7 vol% (16) to 6 vol% for sevoflurane (26) and from 6.6 vol% (28) to 12 vol% for desflurane (26). In this study, SW480 cells were exposed to sevoflurane or desflurane for 3 or 6 h. These incubation times are in accordance with clinical exposure to volatile anesthetics for cancer surgery.
Conclusion
Sevoflurane and desflurane are common inhalative anesthetics used for the maintenance of anesthesia during many surgical procedures, including cancer surgery. In this study, sevoflurane and desflurane revealed no or only slight effects on cell-cycle distribution and apoptosis of SW480 colon cancer cells. Due to the contradicting results of preclinical studies investigating the effect of volatile anesthetics on cancer cells, a recommendation for clinical praxis cannot yet be given.
Acknowledgements
The Authors thank Sigrid Bamberger, Regina Lindner, Marion Schindler, Ruth Spaeth and Gerhard Piendl for excellent technical support.
Footnotes
↵* These Authors equally contributed to this study.
Authors' Contributions
AB, MM, MG and BS designed the study. BS and BG supervised the study. AB, VU, MM and MG performed the assays. AB, VU and GB analyzed the experimental data. AB and VU wrote the article. All Authors revised the article.
This article is freely accessible online.
Presented at: DAC (German Congress of Anesthesiology) 2017, Nürnberg.
This study is part of the thesis of Viktoria Ullrich.
Conflicts of Interest
The Authors declare they have no conflicts of interest in regard to this study.
- Received September 2, 2019.
- Revision received September 21, 2019.
- Accepted September 25, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.