


Abstract
Aim: To evaluate the efficacy of methotrexate, epirubicin and cisplatin (MEC) or gemcitabine and cisplatin (GC) as adjuvant chemotherapy in advanced upper tract urothelium carcinoma (UTUC). Patients and Methods: From 2002 January to 2008 December, a total of 70 patients with advanced UTUC received radical nephroureterctomy at our Institute with MEC and GC as adjuvant chemotherapy. Disease-free survival (DFS), cancer-specific survival (CSS) and overall survival (OS) among the two groups were evaluated. Results: The MEC (n=30) and GC group (n=40) were compared and showed no significant differences in DFS (p=0.859), CSS (p=0.722) and OS (p=0.691). Positive lymph nodes, preoperative creatinine >1.5, old age, a high ECOG state and low BMI are all the independent risk factors of poor prognosis in advanced UTUC. Conclusion: In patients with UTUC, MEC has a non-inferior efficacy to GC in consideration of cancer recurrence, cancer-specific survival and overall survival.
The worldwide incidence rate of urothelial carcinoma is 8.9 per 100,000 person-years for men and 2.2 per 100,000 person-years for women (1). Bladder tumors have been estimated at about 90-95% (urothelial carcinomas) and is the most common malignancy in the urinary tract (2). Upper tract urothelial carcinomas (UTUC) are relatively rare and account for only 5-10% of UCs, but are common in Taiwan (3). Its behavior appears multi-focal and in 17% of cases, concurrent bladder cancer is present (4). Furthermore, an estimated 22-47% of patients with UTUC may suffer from bladder recurrence (5) and 2-6% of patients suffer from contralateral recurrence (6).
A radical nephroureterectomy and bladder cuff excision is standard treatment for UTUC, while offering the benefits of preventing tumor spreading and an entire urinary tract resection (7). However, after definite and en bloc surgical removal of the kidney, it still appears to be a poor prognosis for advanced disease, with a <50% 5-year cancer-specific survival rate in pT2/pT3 tumors and <10% in pT4 patients (8, 9).
For adjuvant chemotherapy, current practice is mainly focused on evidence related to muscle-invasive bladder cancer. Despite the similar morphology between upper and lower tract bladder tumors (10), the phenotype and genotype still showed differences between the two groups (11). Cisplatin-based chemotherapy used in bladder cancer may not always be suitable for patients with UTUC due to potential nephrotoxicity. Current analysis also suggests that data generated from bladder urothelial carcinoma cannot always be extrapolated to patients with UTUC (12, 13).
To avoid poor prognosis in advanced urothelial carcinoma, systemic chemotherapy has been established and M-VAC therapy (methotrexate, vinblastine, doxorubicin and cisplatin), was proposed by the Memorial Sloan Kettering Cancer Center in 1985, which has been widely accepted as a first line regimen of chemotherapy (14). However, cardiotoxicity from doxorubicin is still a risk, and may be in doubt when using this therapeutic protocol. Additionally, significant adverse drug reactions, including bone marrow suppression and stomatitis has been observed, and despite a high response rate is, the survival rate seems still poor (15). Regimens with MEC (methotrexate, epirubicin and cisplatin) have been introduced since 1996 in urothelial carcinoma in the bladder, with wide acceptance in Asian patient groups (16) and have been established as efficacy as M-VAC (17). Thereafter, regimens with MEC have been used in our clinical institute.
Gemcitabine plus cisplatin (GC) has also been used and provides similar survival rate benefits to M-VAC, with a better safety profile and tolerability, whether for adjuvant therapy or neoadjuvant therapy (18). With fewer instances of neutropenic fever, mucositis, body weight loss and fatigue, it offered better compliance and acceptance in patients receiving GC than M-VAC did (19).
In our clinical Institute, each of the two regimens, MEC and GC, have been widely used in patients with advanced urothelial carcinoma in the upper and lower urinary tracts after radical surgery, as adjuvant chemotherapy. To our knowledge, there is no direct comparison of these two regimens available for advanced UTUCs. Thus, we try to identify patients with advanced UTUCs, after a definite radical nephroureterectomy and bladder cuff excision could benefit from these two regimens.
Patients and Methods
From January 2002 to December 2007, we retrospectively evaluated 279 patients with UTUC to receive radical nephroureterectomy and bladder cuff excision with lymph node dissection (open or laparoscopic method) at Taichung Veterans General Hospital. Patients with incomplete data, localized disease (≤pT2N0M0), metastasis disease at diagnosis, non-urothelial carcinoma and any who had received neoadjuvant therapy were excluded. Preoperative contrast-enhanced computed tomography was routinely performed and discussion with radiologist specific in the urinary tract. Pathological specimens were evaluated by a pathologist with expertise in the urinary tract in our institute, and the staging was recorded base on TNM classification.
Follow-up protocol included contrast compute tomography, urine cytology, a cystourethroscope and chest plain film. Patients were evaluated every 3 months for the first two years, every 6 months for the next two years and annually after. Inadequate evaluation and follow up of less than two years was excluded based on this protocol.
A total 70 patients were recorded. Adjuvant chemotherapy had been started within 3 months after definite radical surgery. The standard MEC consisted of methotrexate (30 mg/m2), epirubicin (30 mg/m2) and cisplatin (70 mg/m2) administered every 3 weeks, for 4-6 courses in a cycle. Methotrexate was administered on day 1, while epirubicin and cisplatin were administered on day 2. If after 24 h the CCR (Creatinine Clearance Rate) was <60 cc/min, cisplatin would be divided into two 35 mg/m2 courses on day 2 and day 3. The protocol of GC consists of being administered every 3 weeks, in a 4-6 courses cycle, using a combination of gemcitabine and cisplatin with gemcitabine 1,200 mg/m2 on days 1 and 8, plus cisplatin 70 mg/m2 intravenously on day 9. If after 24 h CCR was <60 cc/min, cisplatin would be divided into two 35 mg/m2 courses on day 9 and 10. If it was needed, the next course would be delayed until after recovery of the absolute neutrophil count ≤500/mm3 and the platelet count ≤100,000/mm3 when G-CSF would be administered for neutropenia. This study has the institute with human ethical issue and the institute review board number was CE13240A-3.
Clinical characteristics were compared using both the Student's t-test and Pearson's Chi-square risk analysis. The definition of recurrence includes bladder recurrence, local recurrence or recurrence at the contralateral kidney, while disease-free survival (DFS) was also recorded. Cancer- specific survival (CSS) was defined as disease specific death, and overall Survival (OS) was defined as all cause death. Kaplan-Meier survival curve estimates and log-rank tests were used to determine the association of DFS, CSS and OS between these two groups of regimens and significance would be accepted at p<0.05.
Univariate and multivariate analysis using the Cox proportional hazards model were used to predict the DFS, CSS and OS. The variables with p-values <0.2 in the univariate analysis were checked into the multivariate model where statistical significance would be accepted at p<0.05 in the multivariate model. All statistical tests were carried out using IBM SPSS version 22.
Results
Table I summarizes the characteristics in a total of 70 patients among the two patient groups, MEC group (n=30) and GC group (n=40). The mean age and BMI (Body Mass Index) appear to possess no statistical differences among the two groups. Risk factors such as smoking, history of uremia, having received a transplant, pre-operative creatinine and pre-operative creatinine >1.5 also showed no significant differences between the two groups. In consideration of the pathology stage, there were 0/8/17/5 patients of pT1/T2/T3/T4 in the MEC group, and 3/5/25/7 patients of pT1/T2/T3/T4 respectively in the GC group (p=0.240). Additionally, there were 24/3/3/0 patients of pN0/N1/N2/N3 in the MEC group, and 29/4/6/1 patients of pN0/N1/N2/N3 respectively in the GC group (p=0.750). In consideration of tumor grading, there were 7/23 patients of Grade 2/3 in the MEC group, and 5/35 patients of Grade 2/3 respectively in the GC group (p=0.234). There was also no significance in multiple lesions, angiolymphatic invasion, surgical margin, positive lymph node and total lymph node number among the two groups. The only significant difference between the two groups may be found in the follow up time, which was relatively longer in the MEC group (45.91±29.61 months vs. 29.35±13.41 months, p=0.003).
The Kaplan-Meier survival curve was used in the evaluation of DFS, CSS and OS among the two groups, which showed no statistical significance among the MEC group and GC group. Figure 1a shows that there is no significance among the two groups in DFS, where the median time in MEC vs. GC was 16.09±8.252 (95%CI=0.000-32.272) and 20.66±7.39 (95%CI=6.187-35.144). Figure 1b and c shows that there was no significant difference in CSS and OS among the two regimens, and both did not reach the medial survival time. The 2-year DFS, CSS and OS rate among MEC vs. GC were 63.3% vs. 64.7%, 81.6% vs. 87.3% and 75.5% vs. 85.0%, respectively. Additionally, the 5-year DFS, CSS and OS rate among MEC vs. GC were 39.4% vs. 44.4%, 81.6% vs. 74.7% and 70.8% vs. 52.1%, respectively. The efficacy of MEC and GC in two independent risk factors, lymph node positive and creatinine, was discussed separately.
Clinical and pathology characteristics of cohorts (N=70).
The patients with positive lymph nodes appeared to have poor prognosis, while the 2-year and 5-year CSS among our population was 55.6% vs. 93.7% and 47.6% vs. 87.5% (p=0.000). The efficacy among this subgroup was examined and Figure 2a, b and c reveals that there is no significant difference in DFS, CSS and OS rates among MEC and GC in patients with positive lymph nodes (n=16, 6 in MEC group and 10 in GC group). The median time of DFS in MEC and GC in lymph node positive patients was 5.13±2.23 (95%CI=0.748-9.502) and 10.09±3.97 (95%CI=2.297-17.875). Both CSS and OS rates among the two regimens in this subgroup did not reach the median survival time.
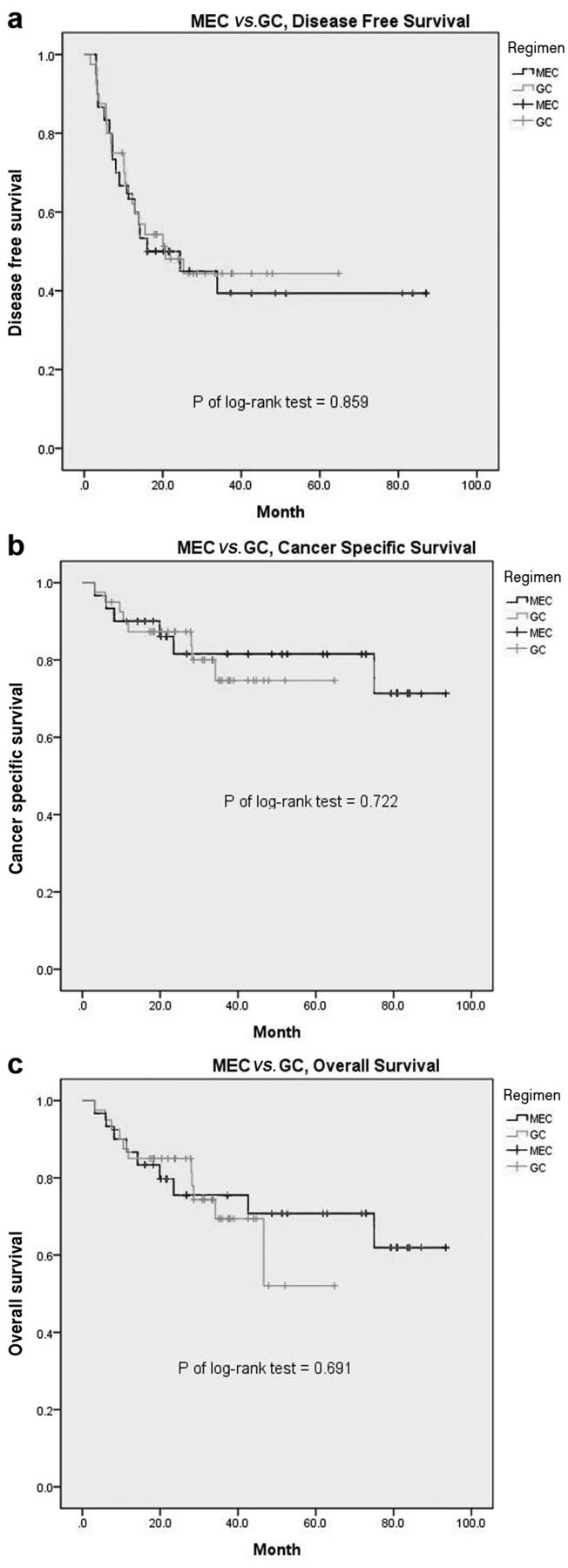
Kaplan-Meier survival curve evaluation of DFS (a), CSS (b) and OS (c) in patients with UTUC who received MEC (n=30) and GC (n=40).

Kaplan-Meier survival curve evaluation for DFS (a), CSS (b) and OS (c) in patients with lymph node positive UTUC (N=16) who received MEC (n=6) and GC (n=10).
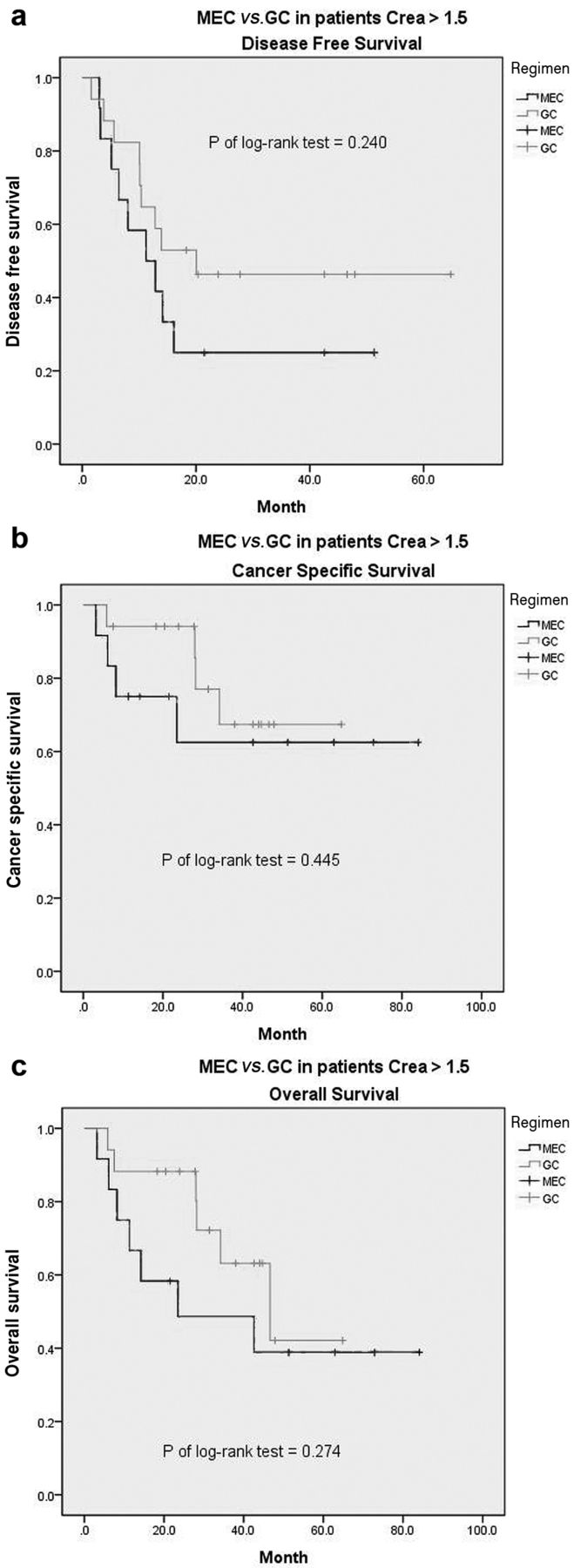
Patients with preoperative creatinine >1.5 also appeared to have a poor prognosis, and the 2-year and 5-year OS among our population was 71.9% vs. 87.4% and 45.2% vs. 83.9% (p=0.013). The efficacy among this subgroup was also examined. Figure 3a, b and c reveals that there is no significant difference in DFS, CSS and OS rates among MEC and GC in patients with creatinine >1.5 (n=29, 12 in MEC group and 17 in GC group). All DFS, CSS and OS in patients who received MEC and GC in this subgroup did not reach the median survival time. Univariate and multivariate analysis with the Cox proportional hazards model were used to predict the risk factors in DFS, CSS and OS.
In Table II, the model of DFS shows that performance state (HR=2.506, 95%CI=1.034-6.071) and lymph node positive (HR=2.520, 95%CI=1.108-5.734) were two independent risk factors for disease recurrence. BMI, uremia, multiple lesions, angiolymphatic invasion, renal calyx tumor, renal pelvis tumor and bladder tumor at diagnosis showed no statistical significance in a multivariate analysis of the DFS model.
In Table III, the model for CSS is discussed. Age (HR=1.097, 95%CI=1.025-1.175), gender (female vs. male, HR=0.012, 95%CI=0.000-0.966) and positive lymph node (HR=40.628, 95%CI=6.283-262.719) were the three independent risk factors for cancer-specific mortality. BMI, performance state, multiple lesions, CIS, Creatinine >1.5 and renal calyx tumor showed no statistical significance in a multivariate analysis of the CSS model.
Table IV reveals univariate analysis and multivariate analysis in the OS model. When compared to CSS, age (HR=1.074, 95%CI=1.023-1.128) was the same significant risk factor. There are three major differences between the OS and CSS models: gender was not related to any risk for all causes of death in this group, but BMI (HR=0.793, 95% CI=0.658-0.957) and creatinine >1.5 (HR=10.214, 95%CI=3.237-32.228), which were not a statistical significance in the CSS model, displayed a significance in the OS model. Among the three univariate and multivariate models, a regimen of adjuvant chemotherapy, MEC or GC, was not a risk factor towards DFS, CSS and OS.
In summary, there is no significant difference in MEC and GC in all UTUC patients, UTUC patients who were lymph node positive or UTUC patients with creatinine >1.5. Performance state and positive lymph nodes were independent risk factors for cancer recurrence (including bladder recurrence). Age, gender and positive lymph node were independent risk factors for cancer specific mortality. Age, BMI, positive lymph node and creatinine >1.5 were independent risk factors for all causes of mortality.
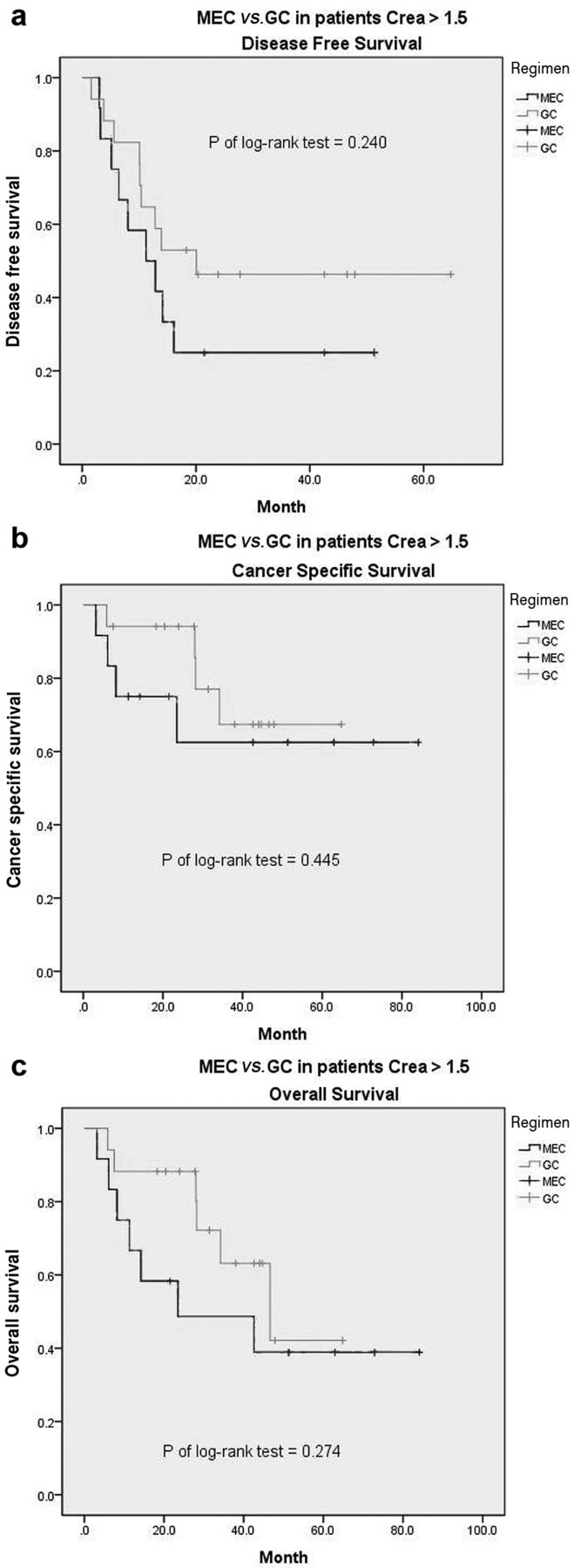
Kaplan-Meier survival curve evaluation for DFS (a), CSS (b) and OS (c) in patients with UTUC and preoperative creatinine >1.5 (N=29) who received MEC (n=12) and GC (n=17).
Univariate and multivariate Cox proportional hazard regression analysis for prediction of disease-free survival.
Discussion
Although UTUC is morphologically similar to bladder cancer, there are occasional phenotypic and genotypic (genetic and epigenetic) differences between UTUC and bladder cancer (11). Thus, despite having the same origin as urothelial carcinoma, further discussion regarding UTUCs is still needed. Adjuvant chemotherapy with a cisplatin base regimen was first introduced in 1985 and revealed a 21% partial remission rate in urothelial carcinoma patients (14) and had been widely accepted until now. Many of publications have reported on the benefits of adjuvant chemotherapy in urothelial carcinoma of the bladder, where one meta-analysis declared a 25% relative reduction in the risk of death for chemotherapy (20). Although there is still controversy, many of the studies have established that there are survival benefits with adjuvant chemotherapy in UTUCs (21, 22).
Kwak et al. directly compared 32 patients with UTUCs who were receiving adjuvant chemotherapy (M-VAC and GC), with 11 patients receiving only a surgical resection, revealing the benefits in DFS (include bladder recurrence) and OS (21). Suzuki et al. further reported DFS and OS in advanced UTUCs, and even further in patients with lymph node involvement (22).
In our Institute, the regimens mentioned above (MEC and GC) have been widely used up until now for advanced lower urinary tract and upper urinary tract urothelial carcinoma with tolerable side effects. Despite M-VAC having been widely used around the world, the side effects of cardiotoxicity and other symptoms make it an undesirable option. MEC has been reported to have a similar efficacy as M-VAC, but with a less toxic effect (17, 23), a factor which was more accepted in our institute. Moreover, the efficacy of GC has been proved in urothelial cancer (19). To our knowledge, there has been no direct comparison of these two regimens, MEC and GC. Which regimen may prove to be superior may be what we need to consider as we discuss more on this topic in the future.
During our investigation, the efficacy of both MEC and GC was comparable when considering DFS, and because bladder recurrence was included, this may reflect the efficacy of systemic chemotherapy. Additionally, there is no difference in CSS and OS, which further suggests that MEC is an effective protocol for UTUCs.
Lymph node-positive patients were discussed separately because their condition has been reported in many publications as an independent risk factor in UTUCs. Kwak et al. state that positive lymph nodes possess a significant risk of recurrence and for all causes of death (21). Kazutoshi et al. further discuss the effect of adjuvant chemotherapy in patients with lymph node positive UTUCs as having a 48% reduction in the risk of recurrence, and a 64% reduction in the risk of cancer specific mortality (24). In our investigation, lymph node positive appears to be a poor prognosis, while having a higher risk of recurrence (HR 2.520, 95%CI=1.108-5.5734), cancer specific mortality (HR 40.628, 95%CI=6.283-262.719) and for all causes of death (HR 10.214, 95%CI=3.237-32.228). MEC and GC appear to display a comparable efficacy with regards to DFS, CSS and OS in this subgroup of patients.
Univariate and multivariate Cox proportional hazard regression analysis for prediction of cancer-specific survival.
Univariate and multivariate Cox proportional hazard regression analysis for prediction of overall survival.
A level of creatinine >1.5 prior to surgery reflects relatively poor renal function and in our experience, may be an additional risk of uremia for patients who are a candidate for a radical nephrectomy. This condition would also indicate whether or not patients could tolerate a complete course of chemotherapy. This is a major difference from urothelial carcinoma in the upper tract and urinary bladder, which could preserve the bilateral kidney with relatively better renal function. Shuichi et al. declare preoperative creatinine as an independent risk factor in regards to CSS in patients with UTUCs (25). Our results show that despite there being no significance in CSS (p=0.126), the prognosis is significantly poorer in OS (5-year survival 45.2%, p=0.013). This may explain the deterioration of renal function after a radical nephrectomy and how cisplatin based chemotherapy would be a risk that can't be ignored and may introduce to all cause death. Respectively, MEC and GC were examined in this subgroup and displayed no differences for all causes of death, which may indicate the comparable efficacy and toxicity.
As outlined in most publications, age and performance state with ECOG may reflect the patient's disabilities and the disease severity. Colin et al. further describe that age, ECOG status and a surgical delay of more than 3 months would cause a risk in prognosis (26). When compared to our result, the higher ECOG score also indicates a higher risk of recurrence (HR=2.506, 95% CI=1.034-6.071, p=0.042) and for all causes of death (HR=4.684, 95% CI=1.207-18.180, p=0.026). It appears likely that age seems to be an independent risk for cancer specific death (HR=1.097, 95%CI=1.025-1.175, p=0.008) and for all causes of death (HR=1.074, 95%CI=1.023-1.128, p=0.004).
BMI is thought to be another risk factor for poor prognosis, which may reflect the cachexia condition of the patient. Liu et al. state that being preoperatively underweight is an independent predictor of unfavorable recurrence-free survival, along with cancer-specific survival in Chinese patients with UTUC who were treated with a radical nephroureterectomy (27). That outcome was the same in comparison with our result, with regards to OS (HR 0.793, 95% CI 0.658-0.957, p=0.016).
Although uremia is an established risk factor for urothelial carcinoma, there was no significance in our cohort. This may due to cisplatin based regimens which should be used in concern of toxicity and side effects in this group of patients and this may lead to a selection bias. Uremic patients with UTUCs under hemodialysis would be excluded in and all of the uremia patients in our population in this cohort had received a renal transplant prior, which may be the reason for the deviation.
In view of its retrospective nature, this study may be limited by its small sample size and short follow up time. By using a larger sample, future prospective studies may give us better answers towards the efficacy of these two regimens in UTUCs. However, due to the current lack of study focus on MEC and GC in UTUCs, there may still be some value in our study.
Conclusion
In patients with upper tract urothelial carcinoma, MEC has a non-inferior efficacy to GC when considering cancer recurrence, cancer specific survival and overall survival. Positive lymph nodes, preoperative creatinine >1.5, old age, a high ECOG state and low BMI are the independent risk factors for a poor prognosis in advanced upper tract urothelial carcinoma. Further multi-institutional, prospective studies are required to confirm these findings.
Footnotes
This article is freely accessible online.
Conflicts of Interest
None of the contributing Authors have any conflict of interest, including specific financial interests or relationships and affiliations relevant to the subject matter or materials discussed in the manuscript.
Ethical Approval
This study has the institute with human ethical issue and the institute review board number was CE13240A-3.
- Received February 7, 2017.
- Revision received February 28, 2017.
- Accepted March 1, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}