


Abstract
Background/Aim: RASA1 (p120RasGAP), encodes Ras GTPase-activating protein 1 and, is a potent tumor suppressor gene that is frequently inactivated in several human cancer types. However, its precise role in hepatocellular carcinoma (HCC) has been blurred. Materials and Methods: We hypothesized that RASA1 plays a crucial role in tumor pathogenesis and progression of HCC. RASA1 expression levels were analyzed in 226 cases of HCC by immunohistochemistry. Results: It was found that 38.68% (41/106) of the high-grade HCC samples and 54.17% (65/120) of the low-grade HCC samples expressed RASA1 protein. The difference between RASA1 expression in high-grade and low-grade HCC was statistically significant (p=0.02). Additionally, RASA1 high expression was inversely associated with larger tumor size (p<0.001). Although RASA1 is known as a tumor suppressor, its role in overall survival (OS) in HCC is unclear. Kaplan-Meier survival analysis showed that patients with low level of RASA1 expression correlated with a significantly poorer survival compared to those with high level of RASA1 expression. Conclusion: These data support that RASA1 could serve as an independent prognostic marker for HCC patients.
Liver cancer, including hepatocellular carcinoma (HCC), is the fifth most common cancer worldwide and the second leading cause of cancer-related deaths worldwide (1). Established risk factor for liver cancer include chronic infection with HBV or HCV, heavy alcohol use, and most probably non-alcoholic fatty liver disease (2). HCC will subsequently lead to elevated angiogenesis and metastasis, which may increase the chemotherapy resistance and be responsible for the poor survival of HCC patients (2, 3). Systemic therapies for HCC patients are still facing challenges regarding drug resistance and drug toxicity.
RAS is a small GTP binding protein that may act as molecular switches of signaling transduction modulating many aspects of cell development involving cell growth, differentiation and survival (4). RAS cycles are characterized by two different conformations, an inactive GDP-bound and an active GTP-bound state, which are controlled by RAS guanine nucleotide exchange factors (GEF) and RAS GTPase-activating proteins (GAPs) (5). RAS-GAP mediates inactivation of RAS proteins by promoting the intrinsic GTPase activity of RAS. A study indicated that the RasGAPs are negative regulators of Ras and its function as potential tumor suppressors (6). Thus, inactivation of RasGAPs could decrease the risk for tumor progression (7).
In addition, patients with liver cancer have high incidence of relapse after resection (8). Recently, the hypothesis of cancer-initiating cells indicated that they have a high potential to metastasize and often cause relapse after treatment (9). Previous studies demonstrate that RAS-GAPs are a suppressor in cancer, which modulates cancer stemness and epithelial-mesenchymal transition (EMT) contributing to relapse (10, 11).
RASA1 (Ras GTPase-activating protein 1; also known as p120RasGAP), is the first identified RasGAP protein. Previous studies have indicated that PTP1B dephosphorylates PITX1 to weaken its protein stability and further reduce RASA1 mRNA expression inhibition, suggesting that RASA1 may involved in the suppression of tumor progression (12). RASA1 has been involved in many biological processes including actin filament polymerization, cellular apoptosis, and cell migration (13). Besides, several studies indicated that onco-microRNAs (micorRNA-21 and micorRNA-182) can promote tumor angiogenesis or lymph node metastasis by targeting RASA1 (14, 15). Therefore, RASA1 functions as a tumor suppressor in several types of cancer. However, study of the role for RASA1 in HCC is relatively scarce.
The aim of this study was to analyze whether RASA1 expression is related to clinicalpathological characteristics and prognostic significance in HCC. To examine RASA1 expression in human HCC clinical samples, 226 surgically resected HCC tumors were subject to immunohistochemistry analysis. Then it further investigated whether combination of RASA1 expression and clinicopathological parameters cuuld serve as an independent prognostic factor in HCC. This study presents data that supports that RASA1 is a relevant target for personalized cancer treatment in HCC.
Materials and Methods
Patients. Primary tumor tissues were obtained from 226 HCC patients receiving surgery in Changhua Christian Hospital from July 2011 to November 2013. The patients' relevant clinical data, including demographic information, pathologic diagnosis, laboratory finding and follow up information, were obtained from medical records. All samples and the respective protected health information were acquired in accordance with the protocols approved by the Changhua Christian Hospital Institutional Review Board. The age of all patients was between 29 and 81 years. Clinical patterns and overall survival data were analyzed by chart review. The clinical characteristics of these 226 specimens are shown in Table I. The follow-up period from surgery until death or the endpoint of this study was 884 days and the median overall survival of all patients was 935 days. All samples and the respective protected health information were acquired in accordance with the protocols approved by the Changhua Christian Hospital Institutional Review Board. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Immunohistochemistry (IHC). Immunohistochemistry (IHC) was performed in order to detect RASA1 expression from paraffin-embedded liver cancer specimens. The RASA1 antibody (Ab40677) was purchased from Abcam (Cambridge, USA). The slides were stained with primary antibody using EnVision Detection Systems Peroxidase/DAB, Rabbit/Mouse kit (Dako, Glostrup, Denmark). The slides were photographed with the microscope (BX50, OLYMPUS, Japan, Tokyo). In liver cancer specimens, the detailed scores for IHC were defined as described previously (16, 17), and the IHC score of RASA1 for each specimen were defined as the cell staining intensity (0=nil; 1=weak; 2=moderate; and 3=strong) multiplied by the percentage of labeled cells (0-100%), leading to scores from 0 to 300. A score higher than the mean was defined as ‘high’ expression, while a score equal to or lower than the mean was categorized as ‘low’ expression in tumor.
Relationship of clinical parameters with RASA1 expression in hepatocellular carcinoma patients.
Statistical analysis. Scoring of immunoreactivity was compared with clinical data to assess correlation with clinical outcome. Chi-square analysis and paired-samples t-test were conducted using SPSS software (Version 13.0 SPSS Inc, Chicago, IL, USA). Differences between experimental groups were calculated with the log-rank test. Survival data was analyzed using the Kaplan-Meier method and variables related to survival were analyzed using SPSS software. Differences with p-values of <0.05 are considered to be statistically significant.

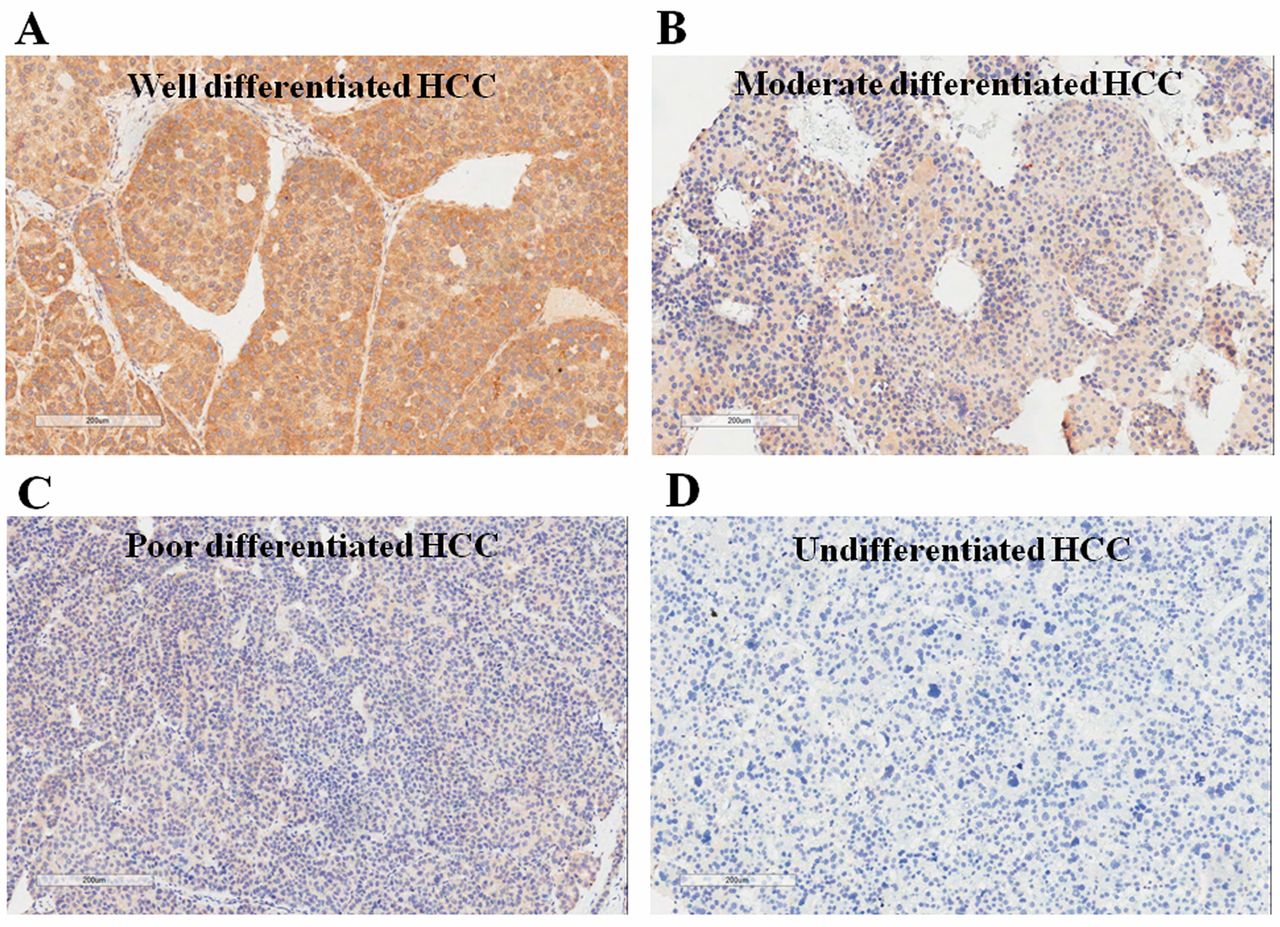
RASA1 protein expression in degree of differentiation in HCC. Positive RASA1 protein expression was predominantly observed in (A) well-differentiated and (B) moderate HCC, but rarely observed in (C) poorly differentiated and (D) undifferentiated HCC.
Results
RASA1 expression is significantly correlated with differentiation and tumor size. A total of 226 HCC specimens were analyzed in the study. The clinicopathological characteristics of these patients are listed in Table I. Age, gender, stage, Hepatitis B surface antigen (HBV), Hepatitis C virus (HCV) and the tumor number were not significantly different between patients with low versus high expression level of RASA1. We observed that 38.68% (41/106) of the high-grade (poorly differentiated/undifferentiated) HCC and 54.17% (65/120) of the low-grade (well/moderate differentiated) HCC expressed high levels of RASA1 protein. The difference between incidence of high RASA1 expression in high- and low-grade HCC was statistically significant (p=0.02). Thus, our data showed that RASA1 protein level was relatively weak in undifferentiated and poorly differentiated tumor samples (Figure 1). Besides, patients with a high level of RASA1 expression had smaller tumor size (43.59±36.21 mm versus 55.25±41.77 mm) than patients with low level of RASA1 expression. Previous studies have demonstrated that differentiation and tumor size are important predictors of survival that it's potential due to the higher RASA1 expression in the well-differentiated HCC (Figure 1). Therefore, our data suggest that RASA1 expression had a correlation with tumor differentiation and tumor growth and could serve as a prognostic marker for HCC.
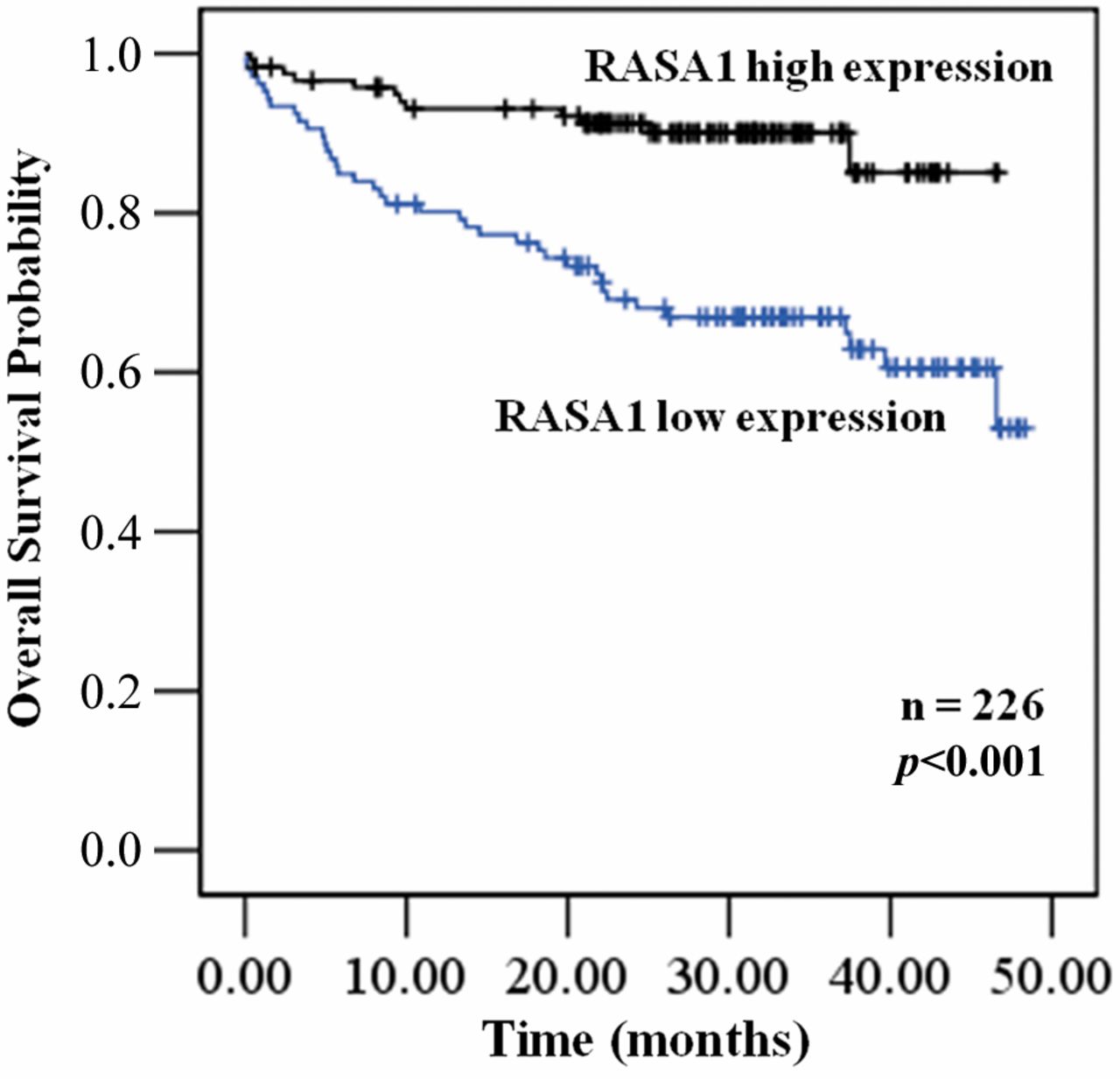
Kaplan Meier plots of the overall survival (OS) rates of HCC patients with high RASA1 expression versus those with low RASA1 expression.
Overall survival (OS) according to differentiation, tumor-Node-Metastasis (TNM) stage, tumor size and RASA1 expression level. The correlation of RASA1 and clinicopathological characteristics with patients' survival was statistically examined by univariate analysis and shown in Table II. Results indicated the significance survival function in several characteristics including age, gender, differentiaiton, TNM stage, hepatitis b surface antigen (HBV), hepatitis c virus (HCV), tumor number, tumor size and RASA1 expression (OS: p=0.465 for age, p=0.478 for gender, p=0.038 for differentiaition, p<0.001 for TNM stage, p=0.903 for HBV, p=0.29 for HCV, p=0.951 for tumor number, p<0.001 for tumor size and p<0.001 for RASA1 expression). First, our analysis of clinical samples revealed that 120 patients with low-grade (well- and moderate-differentiation) had longer survival time than 106 patients with high-grade (poor- and un-differentiation). The OS of HCC patients with low-grade and high-grade was 30.69±9.88 and 26.53±12.66 months, respectively (p<0.038). Next, our data also showed that the OS of HCC patients with tumor size <5 cm and ≥5 cm was 31.6±8.96 and 23.81±14.06 months, respectively (p<0.001) and HCC patients with stage III/IV had a worse prognosis than those with stage I/II specimens (p<0.001). Futhermore, we examined whether RASA1 expression is associated with clinical outcomes in HCC patients. Kaplan-Meier survival analysis showed that patients with low level of RASA1 expression correlated with a significantly poorer survival than those with high level of RASA1 expression (Figure 2). These results suggest that RASA1 expression is lower in the high-grade than the low-grade and may be correlated with tumor growth and consequently result in poor outcomes in HCC patients.
Discussion
RASA1 is ubiquitously expressed across different tissue types. Although previous studies revealed that RASA1 may play tumor suppressive roles in many cancer types (12, 14, 15), the correlation between the role of RASA1 expression, tumor differentiation and overall survival in HCC have not been previously addressed in detail. This study shows that RASA1 protein is rarely expressed in HCC, especially in poor differentiated and undifferentiated tumors or large-sized tumors. Previous studies have demonstrated that differentiation and tumor size are important predictors of survival (18-20) that it's potential due to the higher RASA1 expression in the well-differentiated HCC (Figure 1). RASA1 protein expression was inversely associated with liver cancer aggressiveness (Figure 1). Additionally, RASA1 levels decreased significantly in the nodules of tumor size ≥5 cm compared to their corresponding smaller nodules (Table I). As tumor size increased, survival progressively worsened. Despite accumulating evidence pointing to the regulatory role of RASA1 in cancer progression and proliferation, its regulatory role in outcomes of HCC is still poorly understood. Therefore, our results showed that reduced RASA1 expression is significantly correlated with poor outcome in HCC (Figure 2).
Univariate analysis of influence of clinical characteristics on overall survival in hepatocellular patients.
A previous study indicated that miR-182 could be induced in HCC cells under hypoxia and promote angiogenesis by targeting RASA1 (15). In another study, it was shown that onco-miRNA, miR-21, may promotes malignant behaviors of cancer cells through regulation of RASA1 expression (14). Moreover, a recent study reported that PTP1B de-phosphorylates PITX1 and weakens its protein stability and the transcriptional activity for RASA1 expression, resulting in enhanced tumor suppression in human liver cancer cells (12). Taken together, these data may suggest RASA1 not only regulates cell apoptosis, cell proliferation and tumor growth, but also stimulates cell invasion and cancer metastasis. Our finding in this study is in agreement with studies in several other of cancer, suggesting that RASA1 may act tumor suppressor.
In conclusion, our findings reveal that RASA1 expression level could confer poor outcome and potentially serve as one of prognosis biomarkers and targets for intervention of tumorigenesis in HCC.
Acknowledgements
This study was funded by grants 102-2321-B-750-001- and 103-2314-B-442-002-MY3 from the Ministry of Science and Technology, Taiwan, and RB15001 and RB16001 from Show Chwan Memorial Hospital, Taiwan.
Footnotes
↵* These Authors contributed equally to this study.
Conflicts of Interest
The Authors declare that they have no conflict of interest.
- Received December 1, 2016.
- Revision received December 23, 2016.
- Accepted December 29, 2016.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Triple-negative Breast Cancer: Identification of circRNAs With Efficacy in Preclinical In Vivo Models
- Hepatocellular Carcinoma-associated microRNAs Induced by Hepatoma-derived Growth Factor Stimulation
- Use of signals of positive and negative selection to distinguish cancer genes and passenger genes
- Comparative Genomics Reveals Shared Mutational Landscape in Canine Hemangiosarcoma and Human Angiosarcoma