


Abstract
Malakoplakia, a rare granulomatous disease of infectious etiology, is commonly observed in immunocompromised patients. Chronic lymphocytic leukemia (CLL) is characterized by profound immune dysregulation resulting in significant infection-related morbidity and mortality, and several drugs used in CLL treatment have a severe immunosuppressive effect. Ibrutinib, has become a new standard-of-care in patients with CLL, especially for those harboring unfavorable genetic characteristics such as 17 p deletion, with however, unknown long-term immunological consequences. Here we report a case of a patient with CLL with 17 p deletion diagnosed with malakoplakia of the urinary bladder under ibrutinib therapy who developed severe hypogammaglobulinemia during treatment administration. Presumably, ibrutinib might contribute to the development of malakoplakia on the grounds of induced immunosuppression. This case report highlights the need for regular assessment of immunogammaglobulin adequacy during treatment with ibrutinib, considering that it should be given on a permanent basis.
Malakoplakia is a rare granulomatous disease of infectious etiology. The most common site of involvement of malakoplakia is the urinary tract, followed by the gastrointestinal tract. It is characterized by aggregates of histiocytes with abundant eosinophilic cytoplasm known as Hansemann cells, intermingled with lymphocytes, plasma cells and neutrophils. Malakoplakia is believed to result from the inadequate killing of bacteria by macrophages or monocytes with defective phagolysosomal activity. Partially digested bacteria accumulate in monocytes or macrophages and result in the deposition of calcium and iron on residual bacterial glycolipid, consisting the so-called Michaelis–Gutmann body, which is considered pathognomonic for malakoplakia. This specific disorder is commonly observed to occur in immunocompromised patients and it is possible that its rarity is associated with the level of immunosuppression required (1-3). On the other hand, hematological malignancies are frequently associated with serious impairment of the immune system; among these chronic lymphocytic leukemia (CLL) is characterized, in some cases, by profound immune dysregulation and hypogammaglobulinemia, which contributes to the increased rate of infection of patients with CLL (4-6). Moreover, several drugs used in the treatment of CLL have a severe immunosuppressive effect.
Ibrutinib, an orally administered inhibitor of bruton tyrosine kinase (BTK) that antagonizes b-cell receptor (BCR) has become a new standard-of-care in CLL, especially for patients harboring unfavorable genetic characteristics such as 17 p deletion (7, 8). Although the short-term toxicity of ibrutinib is manageable, there is inadequate information regarding the long-term toxicity as the follow-up of patients included in trials is quite short.
Here we report a case of a patient with CLL with 17 p deletion who was diagnosed with malakoplakia of the urinary bladder while she was receiving therapy with ibrutinib, presented with severe hypogammaglobulinaemia and we discuss the possible immunosuppressive effect of this agent.
Case Report
A 69-year-old female was diagnosed with CLL in 2011, clinical stage A according to the Binet staging system. At her presentation, she was clinically fit and there was no palpable lymphadenopathy present. Her blood cell counts showed: white blood cell (WBC): 8.78×109/l, lymphocytes: 5.56×109/l, granulocytes: 2.59×109/l, hemoglobulin (Hb): 13 g/dl, hematocrit (Ht): 39.1%, platelets: 220×109/l. Biochemical examination did not reveal any abnormal findings and serum electrophoresis disclosed that the immunogammaglobulin level was 0.95 g/dl (normal range=0.7-1.6 g/dl). Blood smear examination disclosed a prominent population of small-sized, mature lymphocytes, as well as the presence of nuclear shadows, and blood immunophenotypic analysis was consistent with CLL. Bone marrow examination revealed infiltration by CLL cells at a percentage of 20%.
The patient was placed on a watch-and-wait policy for 2 years. During follow-up, she underwent regularly blood examinations which showed only a slight increase in the absolute lymphocyte count. As far as the immunogammaglobulin levels were concerned, a random assessment in 2012 gave the following values: IgG: 573 mg/dl (normal range=650-1,600 mg/dl), IgM: 112.3 mg/dl (normal range=50.0-300.0 mg/dl), IgA: 100.4 mg/dl (normal range=40.0-350.0 mg/dl).
In February 2013, our patient presented with enlarged cervical, axillary and inguinal lymph nodes. Computed tomographic evaluation also disclosed enlarged abdominal lymph nodes, as well as the presence of slight splenomegaly. Examination of the peripheral blood revealed that the white blood cell count was 59×109/l, with 86% of lymphocytes, Hb: 11.8 g/dl, Ht: 39.1%, platelets: 97×109/l, IgG: 612 mg/dl, IgM: 101 mg/dl, and IgA: 61 mg/dl; bone marrow biopsy revealed an infiltration of 70% by CLL cells. Furthermore, a biopsy of a cervical lymph node was performed which disclosed an infiltration by small-sized lymphocytes with immunohistochemical features consistent with CLL, mixed with an increased number of paraimmunoblasts.
Before treatment initiation, fluorescence in situ hybridization analysis for 17 p del was performed, which disclosed that the patient harbored deletion of 17 p. In conclusion, the patient was classified in the high-risk CLL group and was in need of first-line treatment. Thus, the patient was administered the ofatumumab regimen, receiving the initial standard weekly protocol and subsequently the first monthly infusion, however, without any significant response. Thereafter, she was placed on second-line therapy with combination of rituximab and bendamustine, but experienced stable disease after four cycles of the aforementioned regimen. At that time period, it was feasible to have access to the new BCR inhibitor, ibrutinib, and thus, she received this agent in November 2014 at the standard dose (420 mg/daily). Gradually, the enlarged lymph nodes disappeared and after a transient increase of peripheral lymphocytes, eventually there was a restoration of normal blood cell counts. Twelve months after ibrutinib initiation, our patient presented to our Department with hematuria, while her disease was still in remission. Computerized tomography of the abdomen and the pelvis revealed the presence of a mass of 5×3×2 cm covering the anterior side wall of the urinary bladder, while there were no enlarged abdominal lymph nodes (Figure 1). Urinary analysis showed hematuria and the urinary culture was positive for Escherichia coli. At that time point, estimation of serum immunogammaglobulin levels was as follows: IgG: 75 mg/dl, IgM: 49.1 mg/dl, and IgA: 30.9 mg/dl.
Transurethal biopsy of the bladder was performed and revealed sheets of histiocytes with fine eosinophilic cytoplasmic granules and basophilic inclusions positively stained with von Kossa stain (Michaelis–Gutmann bodies), while there was no infiltration by malignant cells (Figure 2). The above findings were consistent with the diagnosis of malakoplakia of the urinary bladder. After this diagnosis, the patient was placed on antibiotics while she received intravenous immunoglobulin replacement. She is currently under therapy without hematuria and is about to undergo re-evaluation of the urinary bladder mass.
Discussion
The established treatment algorithms for CLL are currently challenged by the advent of novel drugs whose mechanisms of action are different from those of conventional cytotoxic agents and antibodies (9). One of the most promising new agents is ibrutinib, which is an orally administered inhibitor of BTK that antagonizes BCR, which is critical in normal B-lymphopoiesis (7-8). It has been reported that germline inactivating mutations in BTK lead into an immunodeficiency syndrome first described by Bruton in boys suffering from recurrent bacterial infections. These boys proved to have a severe defect in B-cell maturation, resulting in the virtual absence of immunoglobulin (10-12). On the other hand, it is well known that CLL is characterized by profound immune dysregulation. Hypogammaglobulinemia is present in a varying percentage of patients with B-CLL at the time of diagnosis, depending on the defined lower normal limit, and it is correlated with Binet stage (4).
Patients with heavy bone marrow infiltration or absolute lymphocyte counts exceeding 40×109/l tend to be hypogammaglobulinemic at diagnosis (4). In relation to immunoglobulin subclasses, it has been noted that low levels of IgA, IgM and IgG occur in 30%, 30% and 10%, respectively, of patients with B-CLL at the time of diagnosis (4). Despite its low frequency at the time of diagnosis, the appearance of hypogammaglobulinemia seems to be a continuous phenomenon during the clinical course of untreated B-CLL, affecting up to 75% of patients. IgA and IgM levels are more frequently reduced than IgG, while chemotherapy usually does not improve hypogammaglo-bulinemia, even in patients who enter complete clinical remission (4).
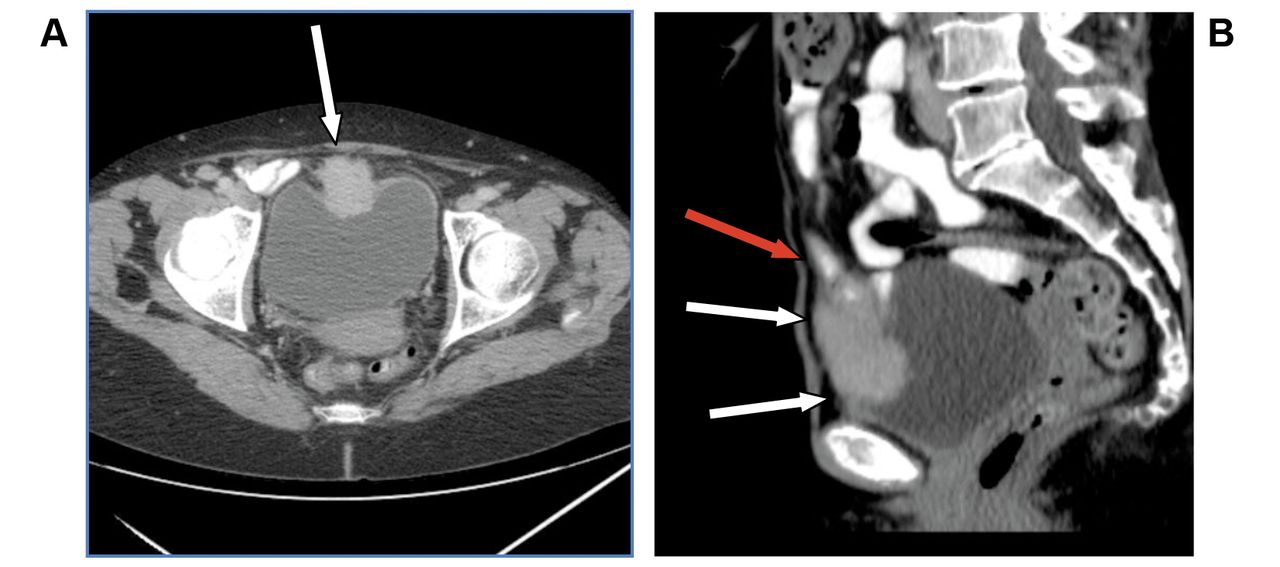
Computerized tomography of the urinary bladder tumor. A: Transverse section: Presence of a mass located at the anterior wall of urinary bladder which is infiltrated (white arrows). B: Sagittal view of the tumor (white arrows). Apart from the urinary bladder, the ileum is also infiltrated (red arrow).

Histology of the urinary bladder tumor. A: Hematoxylin and eosin stain reveals the presence of abundant histiocytes. Original magnification, ×40. B: Michaelis–Gutmann bodies (white arrows) are present (von Kossa stain). Original magnification, ×60.
To what extend ibrutinib-induced BTK inhibition affects normal B-cell function and immunoglobulin levels is not yet fully known. There are some clinical studies in which the immunoglobulin levels were monitored during treatment, showing a gradual improvement of IgA level but also a decline in IgG level. The latter change was apparent after a prolonged period (8, 13-14).
In our case, the patient presented with almost normal IgG levels while IgA and IgM levels were within normal limits before the initiation of ibrutinib treatment. In fact, sequential assessment of immunoglobulin levels was not performed during ibrutinib treatment in order to monitor the possible changes concerning the quantity of each immunoglobulin separately. However, the estimation of immunoglobulin levels performed at the time of the detection of the bladder mass revealed severe hypogammaglobulinemia and, impressively, an extreme decline of IgG level to 75 mg/dl. Of importance was the fact that at the time of the diagnosis of malakoplakia, CLL was in remission with normalization of blood cell counts and no enlarged abdominal lymph nodes, as documented.
Although hypogammaglobulinemia is a common finding during the course of disease, the decrease of immunoglobulin levels, focusing mainly on the depth of decline of IgG level observed after ibrutinib administration, raises the question of the possible involvement of ibrutinib treatment, bearing in mind that the long-term immunological consequences of pharmacological BTK inhibition are unknown.
To our knowledge, this is a first case of malakoplakia of the urinary tract in a patient with CLL under therapy with novel agents such as ibrutinib and this highlights the need for regular assessment of immunogammaglobulin adequacy during treatment with these agents, considering that they should be given on a permanent basis.
Footnotes
Conflicts of Interest
None.
- Received June 23, 2016.
- Revision received July 10, 2016.
- Accepted July 11, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.