


Abstract
Background/Aim: We reported that vitamin D3 increased transforming growth factor (TGF)β2 and decreased prostaglandin (PG)E2 in the breast of normal-risk women, suggesting a protective effect. We determined if the findings held for higher risk women. Patients and Methods: Seventy-eight women received daily for one month/menstrual cycle: placebo, 400 international units (IU) vitamin D3, 2,000 IU vitamin D3 or 2,000 IU vitamin D3/400 mg celecoxib. Nipple aspirate fluid (NAF) and/or serum were analyzed for PGE2, TGFβ1,-2, vitaminD binding protein (DBP) 25(OH)D; and plasma for celecoxib. Results: 25(OH)D increased (p<0.001) in women receiving 2,000 IU vitamin D3. Two thousand IU vitamin D3 lowered NAF PGE2 in normal-risk women (p=0.029), whereas 2,000 IU vitamin D3/celecoxib lowered NAF PGE2 in high-risk women (p=0.063). Serum TGFβ1 was influenced by treatment (p=0.011). NAF TGFβ2 increase correlated with increase in 25(OH)D. DBP serum levels were higher than matched NAF, regardless of race, and did not appreciably change with treatment. Conclusion: Vitamin D3 influenced TGFβ1 and -β2 expression. PGE2 response to vitamin D3 treatment was influenced by a participant's breast cancer risk. The implications of these observations regarding breast cancer risk should be further evaluated.
Dietary vitamin D has been proposed to reduce breast cancer (BCa) risk by controlling cell growth. The odds of developing BCa among women with 25(OH)D levels above 42 ng/ml, requiring a dose of approximately 2,000 IU/day, was 50% less than in women with 25(OH)D levels of 0-11 ng/ml (1). In vitro studies suggest that the active form of vitamin D, 1,25-dihydroxyvitamin D [1,25(OH)2D], decreases cyclooxygenase 2 (COX2) mRNA and protein expression and, thereby, prostaglandin (PG)E2 production, leading to a decrease in cancer cell growth (2).
Preclinical (3) and epidemiological (4) studies suggest that the anti-inflammatory agent celecoxib also reduces BCa risk. Celecoxib inhibits COX2 through direct binding to the molecule, preventing the conversion of arachidonic acid to PGE2 and other PGs (5). 1,25(OH)2D3 is also reported to alter the transforming growth factor (TGF)β pathway, which is important for the prevention and progression of breast carcinogenesis (6).
Breast cells have the enzymatic machinery to convert 25(OH)D3 to 1,25(OH)2D3 (7). Increasing circulating levels of 25(OH)D3 is thought to result in an increased production of 1,25(OH)2D3 locally within breast cells, which, in turn, can affect their proliferation and differentiation (7).
Thus, there is potential for a synergistic effect of improving the vitamin D status with celecoxib in the breast, with the local production of 1,25(OH)2D3 acting to reduce production of COX2, celecoxib to prevent the conversion of arachidonic acid to PGE2 and 1,25(OH)2D3 also increasing the metabolism of the PGE2 produced. We previously reported in a preliminary study that 2,000 IU vitamin D (but not vitamin D plus celecoxib) significantly decreased PGE2 in the breast nipple aspirate fluid (NAF) of normal-risk women (8). To validate our preliminary findings and to determine if they also applied to women at increased breast cancer risk, we now report our findings of a larger cohort of normal-risk women, as well as a cohort of high-risk women who received placebo, 400 IU vitamin D3, 2,000 IU vitamin D3 or 2,000 IU vitamin D3 plus celecoxib. We also evaluated, vitamin D binding protein (DBP) in a subset of women. The major function of DBP is to bind and transport vitamin D and its metabolites (9). Epidemiologic evidence supports a role for DBP in cancer etiology (10). DBP has been demonstrated to be present in different body fluids (serum, urine, breast milk, ascitic fluid, cerebrospinal fluid, saliva and seminal fluid). We aimed to determine if DBP was present in NAF and compare its concentration with matched serum.
Patients and Methods
Participants. Candidates were enrolled in an institutional review board-approved protocol (ClinicalTrials.gov Identifiers NCT01425476 and NCT01769625). Prior to enrollment and at the end of the study, participants had serum chemistries and a complete blood count drawn to insure normalcy and no change in lab values related to treatment. Participants had to lack a history of active breast cancer. They could not have taken non-steroidal anti-inflammatory medications within two weeks of enrollment, nor while on study (except celecoxib if randomized to receive this). They could not be pregnant or nursing. A urine pregnancy test was obtained within 48 h of enrollment unless the candidate had not had a menstrual cycle in the last 12 months, she was >55-years-old or had undergone hysterectomy. The National Cancer Institute's Breast Cancer Risk Assessment Tool (http://www.cancer.gov/bcrisktool) was used to assess a woman's risk of developing breast cancer during the next five-year period. If the participant's risk was ≥1.67% over the next 5 years, the individual was classified as “high-risk”; otherwise as low-risk. Participants were randomized in a double-blind fashion to one of four treatment groups for one month: placebo, 400 IU or 2,000 IU vitamin D3 (cholecalciferol) daily or 2,000 IU vitamin D3 plus 400 mg celecoxib daily. Vitamin D3 doses were obtained from Tishcon (Westbury, NY, USA); celecoxib was obtained from Pfizer (New York, NY, USA). Due to low enrollment, with potential participants indicating they did not want to enroll if they might receive placebo, the protocol was revised such that additional recruits were randomized to one of three groups that included vitamin D3.
Sample collection. We asked permission to collect two sample types from each participant: blood and NAF. NAF was attempted from at least one breast. Scientists performing the biomarker analyses were blinded as to the participant's treatment assignment. Participants were asked to take their last dose of medication the morning of collection. Blood was collected and serum or plasma separated using standard clinical laboratory techniques. NAF was aspirated by a trained physician or nurse clinician using a modified breast pump (11). All samples were collected within six hours of their last medication dose.
Sample analysis. PGE2: Each NAF and serum specimen and standard was analyzed in duplicate. Because of variability in the concentration of biomolecules, NAF PGE2 biomarker levels were calculated per mg total protein. Total protein in NAF was analyzed using a Pierce BCA Kit (Rockford, IL, USA). PGE2 was measured using the high sensitivity PGE2 immunoassay kit from Oxford Biomedical Research (Oxford, MI, USA) per manufacturer's instructions.
25(OH)D: Serum levels of 25(OH)D2, 25(OH)D3 and total 25(OH)D were determined as previously described (12). Briefly, liquid chromatography-mass spectrometry (LC-MS/MS) was performed to determine the concentration of 25(OH)D2 and 25(OH)D3 to give the total concentration of 25(OH)D using a TSQ Quantum Ultra triple mass-spectrometer (Thermo Finnigan Corp., San Jose, CA, USA).
Celecoxib: High-performance liquid chromatography (HPLC) MS analysis was performed using an Agilent 1100 Series system with an G1969 high resolution time of flight (TOF) MS system with an electrospray (ESI) source (Agilent, Santa Clara, CA, USA). The chromatographic and mass spectral data were acquired using MassHunter software (Agilent). Samples were purified using solid-phase extraction (SPE) with Bond Elute C18 cartridges.
TGFβ1 and -2: The concentrations of TGFβ1 and β2 in NAF and serum samples were measured by immunoassay using a kit from R&D Systems (Minneapolis, MN, USA), following the manufacturer's instructions. The samples were analyzed in duplicate.
Vitamin D binding protein (DBP) expression in NAF and matched serum: DBP expression was measured in NAF and matched serum before and after treatment from six women enrolled on study using a DBP Quantikine ELISA Kit from R&D systems, cat# DVDBP0. The samples were randomly chosen. NAF protein was diluted in 180 μl of re-suspension solution; 100 μl of this solution was used to measure DBP in duplicate.
Statistical analysis. Clinical information collected from each participant included breast cancer risk, family history of breast cancer, history of breast biopsy, age, body mass index (BMI) and the number of pregnancies. Risk was calculated using the Gail Model, with women having a 1.67% risk of developing breast cancer in the next five years considered high-risk, otherwise they were considered low- (normal) risk. The original pool of cases numbered 84. Four cases were excluded due to missing risk information, another two due to erroneous information. Our analysis started with n=78 and was done on SPSS v. 20 (https://www-01.ibm.com/software/analytics/spss/products/statistics/). Other exclusions took place due to biomarker information: either a pre- or post-measure was missing or the measures were extreme as defined by SPSS. Outliers were considered extreme if they were two standard deviations from the mean or greater. The change in biomarkers after treatment was calculated for each variable by subtracting the initial values from the final. All biomarker differences were natural log-transformed prior to analysis. Comparisons of changes with treatment, as well as risk for each biomarker, were conducted using two-way analysis of variance (ANOVA). Alpha was set at p<0.05.
Results
Participants. Thirty-two percent of the women were clinically obese (BMI >30). Mean age at enrollment was 47.7 years; most were parous. Mean age of menses was 13.1 and mean age of first pregnancy was 24.8. Table I summarizes the demographic composition of the women in our data set. There were no significant differences between the treatment groups for any of the variables.
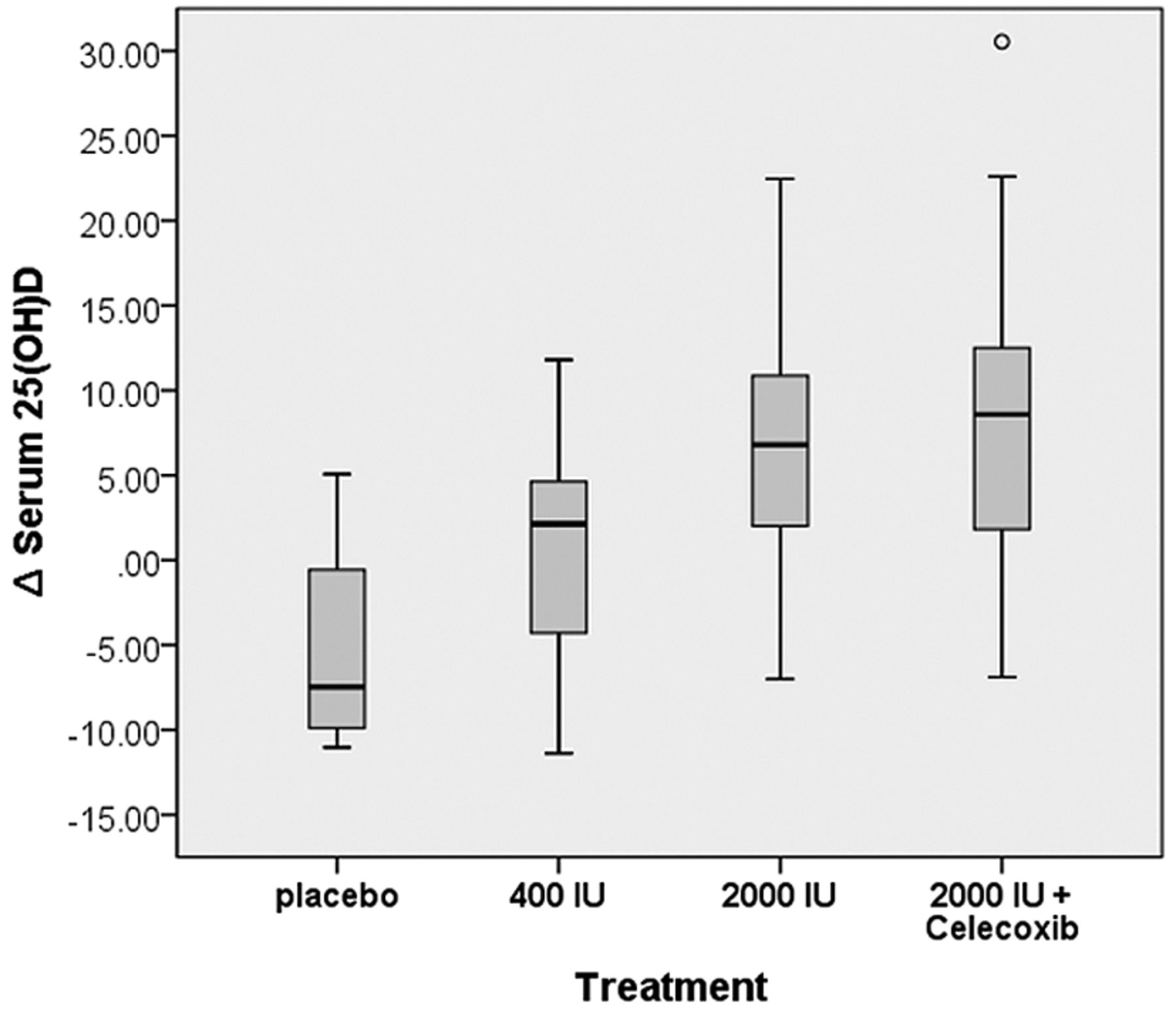
25(OH)D and celecoxib levels increase after treatment. One hundred forty-eight serum samples from 74 participants (half before and half after study completion) were analyzed for 25(OH)D2, 25(OH)D3 and total 25(OH)D. 25(OH)D3 represented more than 95% of the total 25(OH)D for all participants both before and after treatment. There was not a significant difference in 25(OH)D2, 25(OH)D3 or total 25(OH)D levels between the groups at baseline. There was a significant difference (p<0.001) in the change in serum 25(OH)D3 and total 25(OH)D based on treatment, with both groups receiving 2,000 IU vitamin D3 increasing with treatment, whereas values for those receiving placebo declined slightly and those who received 400 IU vitamin D3 remained relatively stable (Table II, Figure 1).
Demographics1.
Biomarker expression before and after treatment1.
Celecoxib was only detected in the plasma of participants randomized to the 2,000 IU vitamin D3 plus celecoxib arm and only after treatment. As expected, levels of the agent significantly increased in this group after treatment (p<0.001).
Change in PGE2 after treatment depends on a woman's breast cancer risk. Considering the entire cohort, there was not a significant difference in the effect of different treatments on NAF PGE2 (Table II), although levels trended lower after treatment with 2,000 IU vitamin D, but increased in the other groups. Serum levels of PGE2 did not significantly change based on treatment. Two thousand IU vitamin D3 lowered NAF PGE2 in normal (low-) risk women (mean Δ -0.168 ng/mg), but not in high-risk women (mean Δ +0.024 ng/mg). This difference in response was significant (p=0.029). Two thousand IU vitamin D3 + celecoxib lowered NAF PGE2 in high-risk women (mean Δ -0.117 ng/mg) but not in normal-risk women (mean Δ +0.124 ng/mg) (Figure 2A). This difference in response was marginally significant (p=0.063) (Figure 2B).
TGFβ1 and -2. TGFβ1 levels in serum but not NAF were influenced by treatment (p=0.001, Table II). TGFβ1 levels in serum remained similar before and after treatment in the placebo and 2,000 IU vitamin D3 groups and decreased after treatment in the 400 IU vitamin D3 group and in the group that received 2,000 IU vitamin D3 + celecoxib. The change in TGFβ2 in the breast was positively correlated with change in the level of vitamin D in the circulation for all 3 treatment groups receiving vitamin D, but not placebo (Figure 3A). This correlation was observed for both normal- (low-risk) and high-risk women (Figure 3B).
DBP. Of the six women in whose matched NAF and serum samples DBP was measured, four were Caucasian and two African American (AA). Three women received 400 IU vitamin D3 and three received 2,000 IU vitamin D3 plus celecoxib. DBP was detectable in all samples. Expression was higher in serum than in NAF before and after treatment for each participant studied. Mean pretreatment DBP for the Caucasian women was 117.3 μg/ml (NAF) and 295 μg/ml (serum); and for the AA women 13.8 μg/ml (NAF) and 61.1 μg/ml (serum). Two AA women and one Caucasian woman received 400 IU vitamin D3; all three women receiving 2,000 IU vitamin D3 + celecoxib were Caucasian. NAF DBP increased after treatment with 400 IU vitamin D3 by 22% for the Caucasian woman and by a mean of 3.6% for the AA women. Serum DBP declined by 4.5% for the Caucasian woman and increased a mean of 0.6% for the AA women. The mean increase in NAF DBP after treatment with 2,000 IU vitamin D3 + celecoxib was 6.7%; in serum it was 23.5%. Three Caucasian women were at increased breast cancer risk (5-year Gail risk of developing breast cancer >1.67%). Mean baseline levels of NAF/serum DBP trended higher (147.5/355.1 μg/ml) for the three high-risk women vs. the three women at low- (normal) risk (18.1/78.7 μg/ml) each of whom had NAF DBP levels below 30 μg/ml and serum DBP levels below 120 μg/ml.
Discussion
BCa is the most common type of cancer and the most common cause of cancer-related death worldwide (13) with an increasing incidence (14). Only two medications (tamoxifen and raloxifene) are approved by the FDA to decrease the risk of developing breast cancer and this approval is limited to high-risk women. Both drugs have side-effects that limit their use. Vitamin D is available over the counter. Celecoxib is used by thousands of women for arthritis relief. We were somewhat surprised to observe (8) that the combination of 2,000 IU of vitamin D3 plus celecoxib was not more effective than 2,000 IU of vitamin D3 alone in decreasing PG expression in normal-risk women. Since the time of that publication, two in vitro studies were published, one in breast cancer (15) and the second in ovarian cancer cells (16) suggesting that 1,25(OH)2D3 and celecoxib demonstrate at least additive effects. To better evaluate the clinical effects of one or both agents, we recruited additional normal-risk women, as well as women at increased breast cancer risk, to validate and extend our findings in our preliminary report.
Vitamin D levels increase after treatment with 2,000 IU vitamin D3 but not with lower doses. 25(OH)D levels increased in women receiving 2,000 IU vitamin D3 with or without celecoxib, but not in women receiving either placebo or 400 IU vitamin D3.
Similar to our earlier study (8), in this larger cohort we observed that 2,000 IU vitamin D3 with or without celecoxib was more effective than either placebo or 400 IU vitamin D in raising circulating levels of the 25(OH)D levels. We also observed a significant increase in plasma celecoxib in those assigned to the 2,000 IU vitamin D3 plus celecoxib group, demonstrating that the participants took their assigned medication. We did not observe in this larger cohort that 2,000 IU vitamin D3 was more effective than other treatments in lowering the cancer promoting prostaglandin PGE2 in the breast, although mean PGE2 in the breast trended down (after treatment) for women treated with 2,000 IU vitamin D3 with or without celecoxib, whereas PGE2 increased in the breast, on average, after treatment in the other groups. There was a significant difference in how high- vs. low-risk patients responded to treatment with 2,000 IU vitamin D3 and a marginally significant difference in how high- vs. low-risk patients responded to treatment with 2,000 IU vitamin D3 + celecoxib. With 2,000 IU vitamin D3 alone, the effect was greater in the low-risk group, with 2,000 IU vitamin D3 + celecoxib, the effect was greater in the high-risk group. Why this was observed is not certain. It is known that the mechanism by which vitamin D and celecoxib influence PGE2 production is different, the former limiting the production of COX2 (2) and the latter directly inhibiting COX2 (5). If validated, our findings suggest that the preferred treatment to decrease breast cancer risk depends on risk status.

Effect of treatment on PGE2 levels in the breast. (A) 2,000 IU vitamin D lowered NAF PGE2 in normal-risk but not in high-risk women (p=0.029). (B) 2,000 IU vitamin D + celecoxib lowered NAF PGE2 in high-risk but not in normal-risk women (p=0.063).

TGFβ2 levels in the breast correlate with changes in vitamin D in the circulation. (A) There was a positive correlation for change in NAF TGFβ2 with change in serum vitamin D for all treatment groups except placebo: 400 IU vitamin D3 (r=0.29), 2,000 IU vitamin D3 (r=0.26), 2,000 IU vitamin D3 + celecoxib (r=0.53). (B) There was a positive correlation for change in NAF TGFβ2 with change in serum vitamin D for both low-risk (r=0.39) and high-risk (r=0.30) groups.
By having both high- and normal-risk cohorts, we were able to determine the effect of both treatment and risk on biomarker response to treatment. We observed that vitamin D treatment was more effective than placebo in lowering TGFβ1 in serum, but not in the breast. This effect was true for both normal and high-risk women. We also observed that change in TGFβ2 in the breast directly correlated with change in vitamin D levels in the circulation, for both normal- and high-risk groups. TGFβ isoforms influence breast cancer risk in multiple ways and the effect(s) depend on the context. TGFβs mediate pro-apoptotic effects during involution (17). Transgenic mice that overexpress TGFβ show increased apoptosis in the mammary epithelium throughout mammary development (18). On the other hand, TGFβs promote cancer progression (19). The effect of vitamin D to increase TGFβ2 levels in the breast are most consistent with a tumor suppressive effect, given the predominant role of TGFβs as an inhibitor of breast cancer development. The effect of vitamin D on TGFβ1 in serum is less clear, since TGFβ1 was not changed in the breast and serum levels reflect the contributions of all organs in the body.
DBP levels in the circulation are marginally associated with cancer risk (10). Analysis of matched NAF samples from women with cancer in one breast but not the other identified DBP as increased in the breasts with cancer (20). It has been reported that mean DBP serum levels are lower in African Americans than Caucasians using a monoclonal (but not a polyclonal) assay (21). We used a DBP monoclonal assay to confirm these findings in serum and assess if similar differences are also present in NAF. Mean pre-treatment NAF DBP for the Caucasian women was 8.5-fold that of AA (117.3 vs. 13.8 μg/ml); serum levels in Caucasians were 4.8-fold that of AA (295.0 vs. 61.1 μg/ml). Changes in DBP levels with treatment were modest in both AA and Caucasian women. Three Caucasian women were at increased breast cancer risk (5-year Gail risk >1.67%). Their mean baseline NAF/serum DBP levels trended higher (147.5/355.1 μg/ml) vs. the three women at low- (normal-) risk (18.1/78.7 μg/ml), each of whom had NAF levels below 30 and serum DBP levels below 120 μg/ml. We acknowledge that the DBP sample size is limited and, therefore, the findings are preliminary.
Vitamin D has been reported to enhance the secretion of TGFβ2 (22). Consistent with that observation, we observed a direct correlation between change in circulating 25(OH)D3 and TGFβ2 levels in the breast. TGFβ2 is thought to have a breast cancer preventive function in healthy organisms. Transgenic mice that overexpress TGFβ exhibit increased apoptosis in the mammary epithelium throughout mammary development (23) as TGFβ mediates proapoptotic effects during involution (24). We previously observed that TGFβ2 significantly increased in breast milk during weaning, as the breast initiated involution back to the pre-pregnant state (25).
In conclusion, 25(OH)D3 and total 25(OH)D levels rose in the circulation in women receiving 2,000 IU vitamin D3 daily (with and without celecoxib) but not with a lesser dose. The effect of 2,000 IU vitamin D3 (with and without celecoxib), but not with the lower dose, was influenced by breast cancer risk. DBP trended higher in women at increased breast cancer risk. TGFβ1 levels in the serum were significantly influenced by vitamin D treatment. TGFβ2 levels in the breast increased in relation to increases in serum levels of vitamin D. The action of vitamin D on TGFβ2 is consistent with a chemopreventive effect.
Acknowledgements
This study was supported, in part, by Department of Defense grant BC073283.
Footnotes
This article is freely accessible online.
- Received August 1, 2016.
- Revision received August 24, 2016.
- Accepted August 26, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.