


Abstract
Background: There exist limited therapeutic opportunities for the treatment of endometrial cancer (EC). Itraconazole, a common anti-fungal agent and a potent inhibitor of the Hedgehog pathway, has been shown to be clinically effective for various types of cancers, but its clinical efficacy for EC is unknown. Herein, we evaluated the efficacy of itraconazole in treating EC. Materials and Methods: We performed immunohistochemistry on EC tumour samples including serous endometrial intraepithelial carcinoma (SEIC). We further evaluated the in vitro efficacy of itraconazole for inhibiting proliferation and migration of EC cell lines. Results: Sonic Hedgehog and glioma-associated oncogene homolog 1 (GLI1) were expressed in SEIC and endometrioid adenocarcinoma. We found that itraconazole significantly inhibited tumour cell growth in both dose-dependent and time-dependent manners and inhibited migration of HEC-1A cells. Conclusion: Hedgehog signaling plays a role in carcinogenesis and malignant progression in EC. Itraconazole at a physiological dose may suppress progression of EC.
The Hedgehog (Hh) signaling pathway has been associated with oncogenesis in breast, colon, lung, and pancreatic cancer (1-3), and its involvement in endometrial carcinoma (EC) has also been suggested (4, 5). Itraconazole, a commonly used oral anti-fungal agent, has been reported to have anticancer effects by inhibiting Hh signaling and angiogenesis, and by reversing resistance to taxanes through inhibition of P-glycoprotein (6-9). Treatment with itraconazole alone has demonstrated clinical benefits in prostate cancer and basal cell carcinoma (10, 11), and Rudin et al. reported a survival benefit of itraconazole in combination with chemotherapy for lung cancer (12). We reported in retrospective studies that combination chemotherapy with itraconazole prolonged survival of patients with refractory ovarian cancer, triple-negative breast cancer, pancreatic cancer, and biliary tract cancer (13-17).
Previous studies reported and association between Hh signaling and endometrial carcinogenesis (4, 5). However, no association was demonstrated with type II carcinogenesis, which is derived from serous endometrial intraepithelial carcinoma (SEIC). If immunohistochemistry of surgical specimens could detect aggressive populations in low-grade, low-stage EC, a close follow-up or adjuvant therapy could be offered. Therefore, we performed an immunohistochemical study of the Hh pathway in surgically-obtained tissues of patients with SEIC and endometrioid adenocarcinoma grade 1 or 2 at International Federation of Gynecology and Obstetrics (FIGO) stage IA with myometrial invasion (18).
Feng et al. further reported that cyclopamine, a specific inhibitor of the Hh pathway, suppressed EC cells in vitro (4). However, whether itraconazole, another inhibitor of the Hh pathway, effectively treats EC has not been reported. Therefore, we examined the effects of itraconazole on human EC cell lines using a modified methylthiazol tetrazolium (MTT) assay and a migration assay.
Materials and Methods
Immunohistochemistry. We reviewed cases of patients with SEIC, and patients who were diagnosed with EC with endometrioid adenocarcinoma grade 1 or 2 at FIGO stage IA with myometrial invasion and negative cytology of ascites and who recurred at our Institution from January 2005 to December 2013. We also reviewed cases with endometrioid adenocarcinoma grade 1 or 2 at FIGO stage IA with myometrial invasion and negative cytology of ascites without recurrence over 5 years after surgery during 2006 and 2007. Stages were retrospectively assigned according to the FIGO staging system for EC (2008) (18).
Paraffin block sections were treated with antigen retrieval solution according to the manufacturer's instructions (Target Retrieval Solution™ S1699; Dako Japan Inc., Tokyo, Japan); reacted with antibodies against sonic Hedgehog (sHh) (1:100; Millipore, Billerica, MA, USA), GLI1 (glioma-associated oncogene homolog 1, 1:50; Santa Cruz Biotechnology Inc., Santa Cruz, CA, USA), PR (1:50; Dako Japan, Inc., Tokyo, Japan), p53 (1:100; Proteintech, Chicago, IL, USA), and chemokine ligand 18 (CCL18, 1:125; Sigma-Aldrich, Tokyo, Japan); and stained using ImmPRESS™ reagent, secondary antibodies, and 3,3’-diaminobenzidine peroxidase substrate kit (Vector Laboratories, Burlingame, CA, USA).
Cell culture. The human EC cell line HEC-1A was obtained from the American Type Culture Collection (Manassas, VA, USA). The Ishikawa human endometrial cancer cell line was kindly provided by Dr. Masato Nishida (Tsukuba University, Ibaraki, Japan) (19, 20). Ishikawa cells were cultured in RPMI-1640 medium, and HEC-1A cells were cultured in McCoy's 5A Modified Medium (GIBCO, Rockville, MD, USA) supplemented with 10% heat-inactivated foetal bovine serum (FBS; Omega, Tarzana, CA, USA) and 1% Penicillin-Streptomycin-Amphotericin B suspension ×100 (Wako Pure Chemical Industries, Ltd., Osaka, Japan).
MTT viability assay. HEC-1A and Ishikawa cells (5×103 cells/well) were plated into 96-well culture plates and left overnight to adhere. When 400 mg of itraconazole oral solution was administered, the serum concentration was measured at around 10−5 M (706 ng/ml) after 48 h according to the label. Attached cells were treated with up to 10−5 M of itraconazole (Sigma-Aldrich, Tokyo, Japan) for 48 h, 72 h, or 96 h. Cell viability was measured using an MTT assay according to the manufacturer's protocol (MTT Cell Proliferation Assay Kit; Cayman Chemical Company, Ann Arbor, MI, USA). Briefly, cells were incubated with MTT reagent for an additional 4 h, and dissolved formazan products were measured by reading the absorbance of samples at 570 nm on a microplate reader. Each experiment was repeated at least three times.
Cell migration assay. A Radius 96-well cell migration assay (Cell Biolabs, San Diego, CA, USA) was used to measure cell migration according to the manufacturer's instructions. Briefly, HEC-1A and Ishikawa cells were seeded and incubated until the wells were 80-90% confluent. The RadiusGel was removed, and the cells were allowed to migrate to a cell-free area for 24 h in the presence of up to 10−5 M itraconazole (Sigma-Aldrich). The circular space was quantitatively evaluated using Adobe Photoshop software (Adobe Systems Incorporated, San Jose, CA, USA). The assays were performed with three replicates and repeated twice.
Statistical analysis. Statistical significance was determined using a Mann–Whitney U-test comparison between two groups. Asterisks shown in the figures indicate differences with p-values of less than 0.05, which were considered significant. The analyses were performed using XLSTAT 2014 (Addinsoft, Paris, France).
Results
Immunohistochemistry. We identified a case of SEIC with adjacent endometrioid adenocarcinoma grade 1 at FIGO stage IA and three recurrent cases with recurrent endometrioid adenocarcinoma grade 1 or 2 at FIGO stage IA. We analyzed the surgical specimens from these four patients and 10 patients with EC with low-grade FIGO stage IA without recurrence. Both sHh and GLI1 staining was positive among all cases. Immunohistochemistry of SEIC specimens revealed expression of sHh, GLI1, and epithelial-to-mesenchymal transition (EMT)-related molecule CCL18 (Figure 1) (21). Immunohistochemical evaluation of sHh and GLI1 did not distinguish between recurrent and non-recurrent low-grade FIGO stage IA EC.
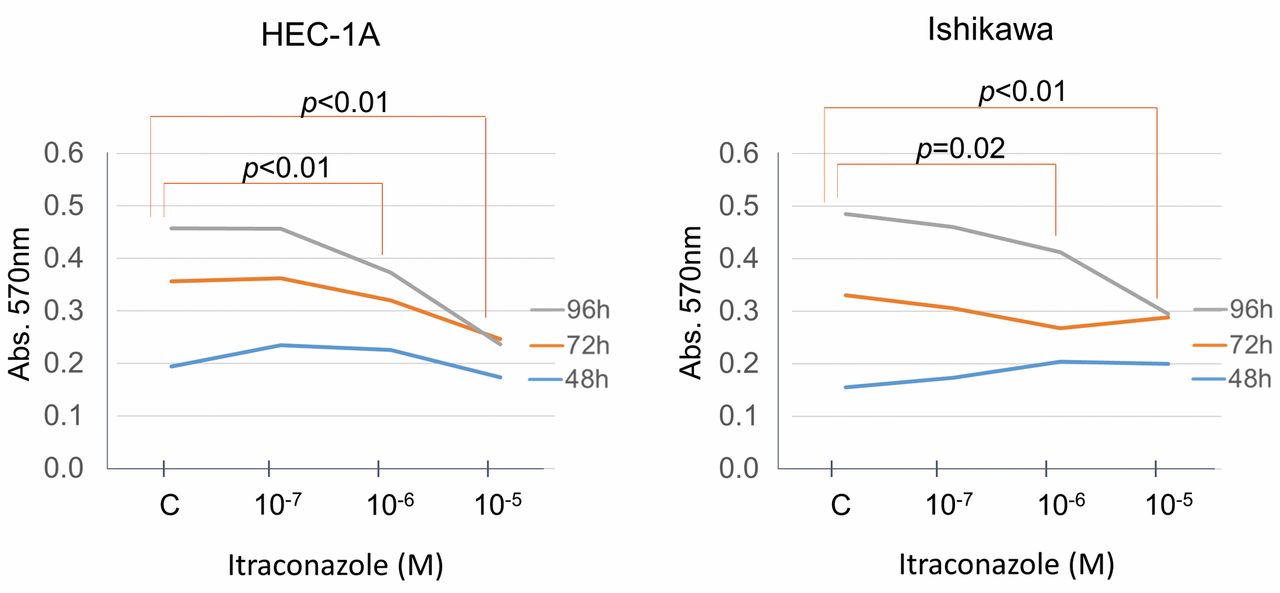
MTT assay. The MTT assay revealed that itraconazole significantly inhibited the growth of Ishikawa and HEC-1A cells in a dose-dependent and time-dependent manner (Figure 2). However, migration was not significantly effected for either Ishikawa or HEC-1A cells (Figure 3). HEC-1A cells exhibited dose-dependent migration retardation (p=0.05 with 10−5 M itraconazole).
Discussion
In the present study, we found that all low-grade, low-stage ECs expressed both sHh and GLI1, indicating that the Hh pathway might play a role in EC carcinogenesis and that its inhibition could be a potential target for suppressing tumour growth. We also found that itraconazole inhibited EC cell growth in vitro, indicating that itraconazole could have anticancer effects in EC at an anti-fungal dose.
EMT is essential for metastasis by conferring migratory, invasive, and stem-cell-like properties on cancer cells (22, 23). Activation of Hh signaling has been shown to promote EMT (24, 25). We reported frequent and high expression of CCL18 in EC compared to the normal endometrium (21). In the present study, immunohistochemistry of SEIC specimens demonstrated coordinated expression of sHh, GLI1, and CCL18, implying their involvement in type II carcinogenesis of EC (26).
The surgical specimens in all cases of low-grade, low-stage ECs expressed sHh and GLI1. Feng et al. reported significant expression of Hh signals in EC compared to the normal endometrium and hyperplasia (4). Although the number of EC samples subjected to immunohistochemistry was small, the current study suggests potential involvement of the Hh pathway with carcinogenesis of EC.
Itraconazole inhibited EC cell proliferation in a time-dependent and dose-dependent manner. To our knowledge, the anticancer effect of itraconazole for EC has not been reported, and this is the first report to demonstrate its possible clinical use for EC. Notably, our results showed that the most effective dose (400 mg) was equivalent to an oral anti-fungal dose. Itraconazole at this dose is well tolerated with mild side-effects and has been safely used in our studies with other carcinoma types (13-17). In contrast, metformin, a commonly used diabetes medication that has been extensively studied in clinical trials as an anticancer drug, requires an excess of a 100-fold higher concentration of the physiological doses in pre-clinical studies (27).

Results of histopathology and immunohistochemistry in serous endometrial intraepithelial carcinoma (SEIC). A: Transition between normal endometrium and SEIC in hematoxylin and eosin (HE) staining; original magnification, ×40. B: Transition zone in the dashed-line inset of A in HE staining, ×200. C: SEIC lesion in the solid-line inset of A in HE staining, ×200. D: Immunostaining for sonic Hedgehog (sHh) (×40). sHh is highly expressed in the SEIC lesion. E: Inset of D, ×200. sHh is expressed in the cytoplasm of SEIC cells. F: Lack of immunostaining for progesterone receptor (PR) (×40) in SEIC. G: Positive immunostaining for p53 (×40) in SEIC. H: Positive immunostaining for chemokine ligand 18 (CCL18) (×40) in SEIC. I: Positive immunostaining for GLI1 (×40) in SEIC. J: Inset of I, ×200. GLI1 is expressed in the cytoplasm and nucleus in SEIC cells.

Itraconazole inhibits the growth of endometrial cancer cells in a dose-dependent and time-dependent manner. The incubation medium was supplemented with itraconazole (10−5 M, 10−6 M and 10−7 M) or with formamide alone as a control. Each line indicates the median absorbance of each sample following culture with or without (C) itraconazole. Cell viability was compared to the control using the Mann-Whitney test. A value of p<0.05 was considered statistically significant. Abs, Absorbance measured at 570 nm using a microplate reader.

Itraconazole did not significantly inhibit migration of HEC-1A or Ishikawa cells. The graph indicates the percentage closure of the circular space in cell cultures. The bars indicate the median percentage. Asterisk indicates that HEC-1A migration was slightly inhibited by 10−5 M itraconazole (p=0.05).
For clinical use, our study indicates that itraconazole as an Hh inhibitor has a high potential for anticancer effects in EC treatment used either alone or in combination with cytotoxic chemotherapy. Furthermore, recurrent EC may be particularly responsive to itraconazole, which is more effective for recurrence of other carcinoma types, such as pancreatic and ovarian cancer, as we previously reported (14, 16). Based on the results herein, we are conducting a window-of-opportunity trial of single itraconazole therapy (UMIN000018388) and a phase II trial of combination chemotherapy with itraconazole (MIN000013951).
Our study examined only a small number of EC cases for immunohistochemistry and made no comparison to benign controls at our Institution. sHh and GLI1 could be markers for a high risk of recurrence but cannot completely distinguish patients whose disease might recur from those in whom it might not. Furthermore, although itraconazole effectively treated EC in vitro, its utility must be verified in vivo, and its potential relationship with positive immunohistochemical identification of sHh and GLI1 certainly requires further investigation.
In conclusion, our study suggests involvement of the Hh pathway with carcinogenesis of EC and demonstrated in vitro efficacy of itraconazole at an antifungal dose for EC. These results will be further examined in our ongoing window-of-opportunity trial.
Acknowledgements
The Ishikawa human EC cell line was kindly provided by Dr. Masato Nishida (Tsukuba University, Ibaraki, Japan). This study was supported by Grant-in-Aid for Researchers, Hyogo College of Medicine (Hiroshi Tsubamoto).
- Received October 12, 2015.
- Revision received November 6, 2015.
- Accepted November 23, 2015.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}