


Abstract
Background: Lung cancer is the leading cause of death in the United States, with reported inferior survival among African-Americans. Patients and Methods: Kaplan–Meier and Cox regression methods were used to compare survival outcomes of 569 patients diagnosed with stage I non-small cell lung cancer from 2001-2010. Results: African-Americans and Whites differed significantly by age, sex, and insurance type. The median follow-up was 2.3 years. The 2-, 5- and 8-year overall survival was 72%, 47%, and 38%, respectively. Age, stage, insurance type, and surgery were significant predictors of overall survival which remained significant after adjusting for other variables, including race, gender, histology, smoking history, treatment era, chemotherapy or radiotherapy which were not. Conclusion: Insurance status but not race is an important predictor of survival in patients with stage I non-small cell lung cancer.
Lung cancer continues to be the leading cause of death for both men and women. In 2014, approximately 224,210 new cases of lung cancer were diagnosed, with 159,260 estimated deaths, which is about 28% of all deaths from cancer (1). Worldwide, lung cancer-related deaths account for approximately 1.35 million patients each year, which is more than deaths from the four most common types of cancer combined (of the colon, breast, prostate, pancreas) (2, 3).
About one fifth of all patients newly diagnosed with lung cancer in the United States will have early-stage disease for which surgical resection remains as the gold standard-of-care for those with adequate cardiopulmonary reserve. Without treatment, the 5-year survival rate for those with early-stage non-small cell lung cancer (NSCLC) is poor (<5%) (4). The National Comprehensive Cancer Network recommends surgical resection alone or with adjuvant chemotherapy for stage I and II lung cancer.
There are reports of higher age-adjusted death rates among African–Americans (~96 per 100,000) compared to whites (~73 per 100,000 population) with a 1.3:1 death rate ratio (1, 5). It has been suggested that a reason for this disparity is a disproportionate disadvantage for African–Americans with regard to receipt of treatment for NSCLC compared to Whites (6-9). It has also been reported that African–Americans have unequal access to optimum therapy to treat lung cancer, including both surgery for early-stage disease and chemotherapy for more advanced disease (6-12).
In addition to race insurance status has also been reported to be a possible factor for disparate outcomes (13, 14). For a deadly cancer such as NSCLC, where appropriate treatment is crucial to improve survival, unfortunately, healthcare insurance status can dictate whether such treatment can be delivered in a timely fashion. In addition, differences in race, ethnicity, income, education, and other factors that are related to insurance status directly or indirectly may also have an impact on treatment receipt and related survival outcome (15-19). With the implementation of the Affordable Care Act (ACA), major changes are expected in the insurance system. Therefore, it is important to investigate the effect of differences in healthcare insurance status on cancer care and outcomes. Even though it is often suggested that African–American race is associated with under-insured or poor socioeconomic status, there is however, no study to have looked into race and insurance status together and into their effect on treatment receipt and outcome in early-stage lung cancer.
The Eastern part of North Carolina in the USA is unique in many aspects. It has a higher percentage of African–American population than the national average, relative lower socioeconomic status with a higher percentage under the poverty level and a high incidence of tobacco use (20, 21). The purpose of this study was to examine the outcome of stage I NSCLC in relationship with race and insurance status, as well as other clinical factors, for patients who were diagnosed and treated at the Leo Jenkins Cancer Center, the largest cancer facility in Eastern North Carolina.
Patients and Methods
Data source. This is a retrospective study. Patients who were diagnosed from 2001 through 2010 at the Leo Jenkins Cancer Center were identified from the facility's cancer registry. Further refinement of the search was carried out to select only patients with NSCLC and stage I disease. An Institutional Review Board approval was obtained for this study (UMCIRB# 11-0351).
Variables. We collected data on age, race, histology, stage, smoking history, and healthcare insurance information. We also collected treatment history, including surgery, chemotherapy and radiation therapy. The age was divided into three categories: 50 years or less, 51 to 70 years, and over 70 years. Race was categorized as White or African American. The histology was grouped as squamous cell, adenocarcinoma, non-small cell lung cancer not otherwise specified (NSCLC-NOS), large cell neuroendocrine cancer (LCNEC) and broncho-alveolar carcinoma (BAC). The small cell subtype and other categories were excluded. The smoking history was divided into three groups: never smokers, current and previous smokers, and unknown. The healthcare insurance information was categorized into Medicare with and without supplement, Medicaid, no insurance/self-pay, and private. The treatment variables were divided into surgery, chemotherapy and radiation therapy. Chemotherapy was given adjuvantly at the discretion of the treating physician. Radiotherapy was used as definitive treatment using standard fractionation where surgical resection was contraindicated owing to medical comorbidities. Finally, the treatment period was divided into an early era (2001-2005) and later era (2006-2010).
Survival. Overall survival (OS) was defined as the number of months from the day of diagnosis to the day of death. All-cause mortality was used in the survival analysis. Patients were censored if they were alive at the last date of contact.
Statistical analysis. All statistical analyses were performed using SAS 9.3 statistical software (SAS institute, Inc., Cary, NC, USA). Comparisons of demographic, clinical and pathologic variables between African–Americans and Whites were made using Fisher's exact (categorical) and Deuchler-Wilcoxon (continuous) tests. Univariable survival rate analyses were estimated using the Kaplan–Meier method, with comparison made between the groups using log-rank test. Multivariable analysis was performed using Cox proportional hazard model. Statistical significance was assumed for a two-tailed p-value of less than 0.05.
Results
Of 569 patients, 141 (25%) were African–Americans while 428 patients were White. The median age for the entire population was 66 years (range=44-85 years). The median follow-up time was 2.3 years (SD=2.5 years; interquartile range=3.9 years). The predominant histology was squamous cell carcinoma with 249 patients (44%), followed by 34% (n=195) of adenocarcinoma, NSCLC-NOS (11%, n=63), large cell neuroendocrine type (5%, n=28) and BAC (6%, n=34). About 60% of the patients were male, with 59% of patients being diagnosed with stage IA disease. Surgery was the primary form of therapy (72%). Two-thirds of the patients were treated before 2006.
Table I shows the distribution of patients and treatment variables between the two races. There were more patients aged >70 years among Whites compared to African–Americans. Similarly, there were more women patients among Whites. Examining the insurance sub-types, Whites had more private insurance, Medicare with supplement and less Medicaid compared with African–Americans. These differences were statistically significant for age distribution (p<0.0042), gender distribution (p=0.022) and insurance type (p<0.0001). There was no significant difference in smoking prevalence, stage distribution, year of treatment or receipt of surgery, radiation or chemotherapy treatment.
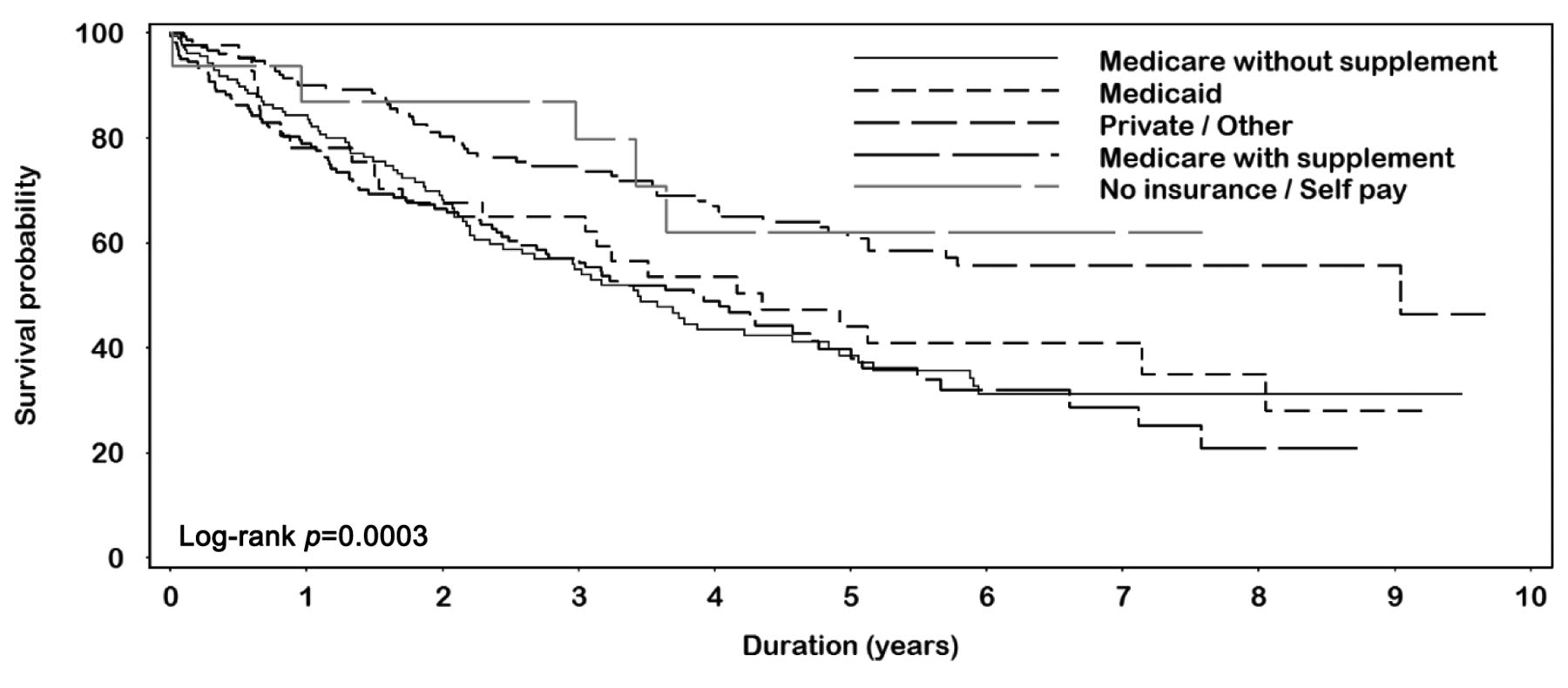
The 2-, 5- and 8-year OS rates for the entire group were 72%, 47% and 38%, respectively. On univariable analysis using Kaplan–Meier survival, younger age (p≤0.0001) (Figure 1) and stage IA (p=0.0043) (Figure 2) were significantly better. Surgical treatment provided significant survival benefit (Figure 3). Race was not a significant predictor of survival on univariate analysis (p=0.47). Among insurance types, Medicaid and Medicare with or without supplement were inferior compared with private (Figure 4). There were significant differences by histology, with BAC providing the best survival outcome (0.0059).
Table II shows multivariable analysis using a Cox-regression model. OS for those younger than 50 years was significantly better compared with those 51-70 years (p=0.05) or >70 years (p=0.008). As expected, survival of those with lower disease stage was significantly better. Surgery significantly conferred OS benefit (p<0.0001) as well, while radiation did not. Compared with private insurance, Medicare without supplement (p=0.048) and Medicaid (p=0.034) remained significantly inferior for OS, while Medicare with supplement and no insurance/self-pay were not significant. Other variables including race, gender, smoking status, chemotherapy, year of treatment did not statistically significantly affect OS.
Discussion
The reasons for survival disparities could be multi-factorial, including low socioeconomic status, lack of trust or misbelief in the current healthcare system, lack of education, and ethnicity. Rather than one single factor being responsible for disparate outcomes, these are often interrelated.

Overall survival by age group.

Overall survival by stage.
There has been a wealth of literature regarding racial disparities in cancer treatment outcomes for many cancer subtypes including NSCLC (22-24). While some reports suggested the existence of racial disparities, particularly between Whites and African–Americans (22-24) with inferior survival for African–Americans, others have found similar outcomes when treatment is accessible and adequate (25-27).
Many reports have shown disparate access to treatment by race for all stages of NSCLC. Lathan et al. reported that African–American patients were 45% less likely to undergo surgery for early-stage disease (27). Similarly, Greenwald et al. (7) and Hardy et al. (5), found that African–Americans were 23% and 37% less likely to receive optimal surgery, respectively, for early-stage disease than Whites. For advanced-stage cancer, several reports found less access to chemotherapy or radiotherapy for African–Americans (5, 10, 28). In addition, African–Americans are also noted to receive single-agent chemotherapy compared with platinum-based doublet for advanced lung cancer, the latter of which has been shown to improve survival (9).
In contrast to the above reports, Hardy et al. noted no difference in survival between the two races in patients aged 65 years or more using the Surveillance, Epidemiology, and End Results Program (SEER) database after adjusting for other variables (5). Blackstock et al. looked at survival outcomes in patients with stage IV NSCLC who were treated on Cancer and Leukemia Group B protocols and found no difference in survival after adjustment for other variables such as healthcare coverage and income (25).
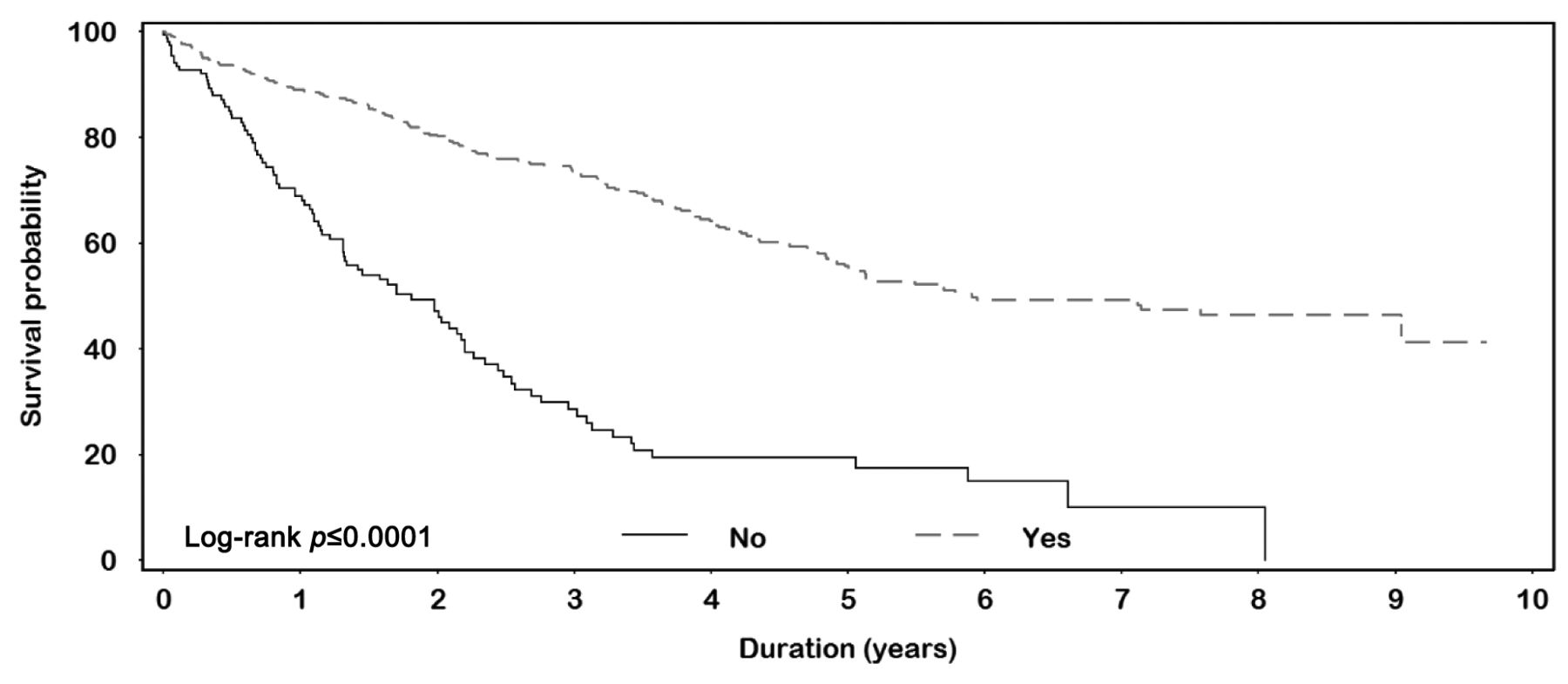
Overall survival by surgery.

Overall survival by insurance type.
In our study, we found no difference in outcomes between the two races neither independently nor after adjustment for other confounding factors. In addition, we found the receipt of treatment, including surgery, radiation and chemotherapy, to be well-balanced between the two groups with no differences. These findings indicate that access to care and equivalent treatment may prevent significant disparities in outcomes for patients with stage I NSCLC.
Similarly, differences in insurance status can also contribute to disparities in cancer treatment outcomes. The insurance system in the United States is divided between public and private providers, with an estimated 24% of adults under 65 years currently being uninsured (19). Slatore et al. published a large meta-analysis and found that patients with lung cancer who have Medicaid or no insurance had significantly worse outcomes compared with other insurance types (13). Groth et al. used the California Cancer Registry and noted private insurance was more likely to offer curative cancer surgery, including lobectomy for early-stage lung cancer compared with Medicare, Medicaid or no insurance (4). In addition, they noted African–Americans were less likely to undergo lobectomy, although they did not observe a significant interaction between race and insurance status. Bradley et al. used the State of Michigan Tumor Registry to look at Medicaid insurance enrollment after or before cancer diagnosis for three of the most common types of cancer of the breast, lung and colorectal and compared with other insurance types (14). They reported patients who were enrolled in Medicaid after cancer diagnosis had a significantly worse 8-year survival compared with those with other types of insurance and with those who were enrolled into Medicaid prior to diagnosis of cancer.
Patient's characteristics, stage I lung cancer (N=569).
Multivariable hazard ratios for stage I lung cancer (N=569).
More recently, Walker et al. looked at the SEER database for 10 most deadly cancer types, including lung cancer, and found that having Medicaid or no insurance was more frequently associated with risk of death compared to other insurance types, even after adjusting for other variables (19).
In our study, we observed a significant impact of insurance status on survival. Medicaid continued to be associated with inferior survival. In addition, Medicare without supplement was also associated with inferior survival. This difference remained significant even after adjusting for other variables. We also noted a significant difference in the distribution of insurance type between the two races with African–Americans having more Medicaid and Medicare without supplement. However, we were unable to note any significant difference in survival between the two races. These findings suggest that different insurance coverage may lead to different survival outcomes for individuals with lung cancer, regardless of race and stage of disease at presentation.
A hypothesis that may also be associated with such results is that enrollment in Medicaid often occurs after cancer is diagnosed. Patients who are diagnosed with cancer due to symptoms may have more advanced disease than those who routinely have health evaluations and screenings owing to available insurance. This can potentially cause lead-time bias, accounting for the inferior outcomes for those with more advanced disease that is associated with Medicaid (14). In our study, having patients with only stage I disease excluded this potential confounding factor.
There exists a strong interaction between race, socioeconomic status, access to adequate health care and the ability to have insurance. As Walker et al. found, lack of insurance was more commonly associated with male sex, non-White race, rural residence and higher county poverty level, all of which were statistically significant. In a 2010 survey, about 44% of adults aged 19-64 years were either underinsured or uninsured (19), totaling 81 million individuals. With the ACA, an increase in Medicaid enrollment of 105 million individuals by 2019 is expected (19). Therefore, it remains important to understand this complex relationship between insurance, race, and cancer-related outcomes.
Our study has several relevant findings. This is a large cohort of patients with stage I NSCLC who were diagnosed and treated at a single institution, which eliminated the inter-institute treatment variation. The population was drawn from one geographic area and presumably represents a group with similar access to care. Our dataset has a large representation of African–Americans in the patient population. Comparing access with treatment, we found similar access for both African–Americans and Whites, including access to surgery, radiation and chemotherapy. There was no difference in survival between the two races on univariable or multivariable analysis. However, examining the distribution of insurance types, there was a significant difference between the two groups, with Whites having more individuals with private insurance and Medicare with supplement, versus African–Americans with more Medicaid and Medicare without supplement. Similar to previous studies, we found having Medicaid was associated with significantly inferior survival, which existed even after adjustment for other variables. In addition, we also found that Medicare without supplement was associated with an adverse survival outcome. In contrast to other studies, we did not find an inferior outcome for the uninsured group, which could be due to the small number of patients or association of self-pay in that category. Our study included only patients with stage I disease, which may have lowered the possibility of having confounding factors such as lead-time bias. Younger age, lower disease stage and receipt of surgery also remained important prognostic factors on multivariable analysis. Our study is the first to examine the complex interaction between race and the insurance status for patients with stage I NSCLC and its impact on survival.
Like any other study, ours also has several limitations including its retrospective nature with inherent bias. In addition, we do not have information on the time interval between the diagnosis and the receipt of Medicaid insurance, which may have influenced the results. We also do not have information regarding household income.
In conclusion, having Medicaid and Medicare without supplement is associated with inferior survival, which remained significant on multivariable analysis after adjustment for other variables. In addition, young age, lower disease stage and undergoing surgery are associated with significant improvement in survival. Race alone is not a predictor for survival outcomes, neither on univariable nor on multivariable analysis. Given the complex interaction between several factors with insurance status and the likelihood of an increase in Medicaid enrollment under the ACA, it is important to understand their relationship to improve healthcare-related outcomes. More studies are warranted in order to understand the influence of insurance status on survival outcomes in lung cancer.
Footnotes
Funding
None.
Disclosures
None.
Conflicts of Interest
The Authors have no conflicts of interest to report in regard to this study.
- Received March 22, 2015.
- Revision received April 21, 2015.
- Accepted April 24, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}