


Abstract
Claudin dysregulation has been described in various tumor types; however, its clinical relevance is poorly understood. We present a study in which we assessed the expression of claudin 1 (CLDN1) and CLDN4 in oral squamous cell carcinoma (OSCC), as well as their prognostic relevance. Immunohistochemical analysis of CLDN1 and CLDN4 expression was carried out on tissue sections from 65 OSCCs. The presence of CLDN1 in the invasive front of tumor islands was associated with neck node metastasis, and the expression of CLDN4 was associated with higher histological grade, and tumor recurrence. Membranous staining for CLDN4 in tumor cells, and weak intensity of CLDN4 immunoexpression were predictive for poorer survival. In a multivariate analysis for disease recurrence, CLDN1 immunostaining was statistically significant. Specifically, CDLN1 expression in the tumor invasive front was associated with tumor recurrence. Our results indicate that CLDN4 expression is correlated with poor prognosis, and CLDN1 expression may be an indicator of recurrence of OSCC.
Oral squamous cell carcinoma (OSCC), which accounts for 24% of all head and neck cancers (1), is characterized by an aggressive growth pattern, a high degree of local invasiveness and cervical lymph node spread (2). Overall, the 5-year survival rate is approximately 50%, and despite recent treatment advances, this rate has not changed in the past 30 years (3). Treatment failure in patients with OSCC can include local recurrence, cervical recurrence, distant metastases or development of a second primary cancer. Despite intensive treatment of the primary disease, approximately 50% to 60% of patients will later develop locoregional recurrence, and even when a surgical resection with negative histopathological margins is achieved, approximately 20% of patients will have local recurrence (4). The most important factor in the prognosis of oral cancer is the presence of metastases in the lymph nodes of the neck (5). However, in 10-20% of the patients clinically diagnosed with lymph node metastases, no lymph node metastasis is actually found (6). Conversely, 24-50% of patients who are clinically diagnosed with no neck lymph node metastases, and have not had a neck dissection do develop regional recurrence (7).
Based on the hypothesis that the expression of certain genes confers on a tumor the ability to progress and metastasize, many biomarkers have been studied for the prediction of metastatic potential in OSCC. The invasive and metastatic activities of cancer cells largely depend on cell cell and cell extracellular matrix adhesion (8).
Epithelial cells adhere tightly to their neighbors through specialized junctional complexes. Loss of cell-cell adhesion is considered an essential step in the process of invasion and metastasis, making cell cell adhesion proteins potential predictive biomarkers for both metastasis and recurrence (7). There are four main types of intercellular junctions: desmosome, tight, adherens, and gap junctions. Tight junctions (TJs) occur in stratified epithelia, and are located at the most apical part of the cells. TJs consist mainly of occludins and claudins, and are critical for maintaining normal structure and physiological function of the epithelium (9). TJs serve not only as physical barriers to the transport of ions, water, and proteins (gate function), but also play critical roles in maintaining cell polarity (fence function) and signal transduction (9, 11). However, cancer cells frequently exhibit abnormal TJ function (12) and, in fact, one of the hallmarks of malignant transformation of epithelia is the loss of TJs (13). Claudins, the major components of TJs, belong to a family of transmembrane proteins (28 identified to date) that are crucial for the fence and gate functions in epithelia (9, 12, 14). Claudins were named after the Latin verb ‘claudere’, which means ‘to close’, reflecting that they are the key proteins for the sealing of the extracellular space. They are integral transmembrane proteins with four transmembrane domains and two extracellular loops through which they bind to claudins on adjacent cells forming homodimers or heterodimers (15). The expression pattern of claudins is usually tissue-specific; however, most tissues express multiple claudins that can interact in either a homotypic or heterotypic fashion to form TJs (9). It is the exact combination of claudins within a given tissue which determines the selectivity, strength and tightness of the TJs (12). Claudins are also capable of recruiting signaling proteins, thereby regulating various cellular processes including cell growth, differentiation and tumorigenesis (16, 17). Claudins are de-regulated in several tumor types (18), and loss or gain of claudin expression has been associated with biological behavior in certain cancers (19). Claudin 1 (CLDN1) and CLDN4 are among the most frequently de-regulated members of the claudin family (12). The down-regulation of several claudins in cancer is consistent with the disruption of TJs during tumorigenesis, but claudin overexpression has also been reported in several cancers (12). Furthermore, increased expression of claudins may promote tumorigenesis, disease recurrence (20), and tumor progression through their positive effects on cell migration, invasion and metastasis (21); these relationships are poorly understood. Conversely, low expression of CLDN4 is associated with poor prognosis in certain subtypes of breast (22), pancreatic (23) and colonic (24) cancer. As yet, there have been very few studies on CLDN1 and CLDN4 expression in OSCC, and their prognostic significance is still unclear.
Clinical features of 65 patients with oral squamous cell carcinoma.
Statistical relationship between patterns of immunostaining of CLDN1 and several clinicopathological characteristics.
Statistical relationship between intensity of staining for CLDN1 and several clinicopathological characteristics.
The aim of the present study was to analyze the immunoexpression of CLDN1 and CLDN4 in OSCC and their relationship with patient prognosis and survival. Specifically, we wanted to address whether there was an association between the immunoexpression of CLDN1 or CLDN4 and disease recurrence and patient survival.
Materials and Methods
Patients. A total of 65 formalin-fixed and paraffin-embedded tumor samples were obtained from 65 patients who underwent curative surgical resection from primary OSCC at the Central University Hospital of Asturias (HUCA) between 1998 and 2004. All patients provided written informed consent according to institutional guidelines. No patients had received preoperative chemotherapy or radiotherapy. Fifty patients were male and 15 were female. The mean age was 58.9 years (range=24-88 years). Postoperative radiotherapy was administered to 22 (32%) patients. The characteristics of the patients studied and the clinicopathological features of their tumors are provided in Table I. The stage of disease was determined after the surgical resection of the tumor according to the TNM system of the International Union Against Cancer (sixth edition) (25). Tobacco and alcohol consumption history was determined from medical records. Alcohol consumption was described in terms of beer, wine or hard liquor. A drinker was defined as a person who self-reported consuming four or more drinks of any alcoholic beverage type per day for at least 10 years. For comparability, one drink is equivalent to 14 g of ethanol, which generally corresponds to 330 ml of beer, 150 ml of wine, and 36 ml of hard liquor (26).
Statistical relationship between pattern of immunostaining for CLDN4 and several clinicopathological characteristics.
Patients were followed-up every two months for the first six months after completing the treatment, every three months until the second year, and every six months thereafter. This study was retrospective and all investigations were performed with the permission of the Ethical Committee of HUCA to the project number PI070675.

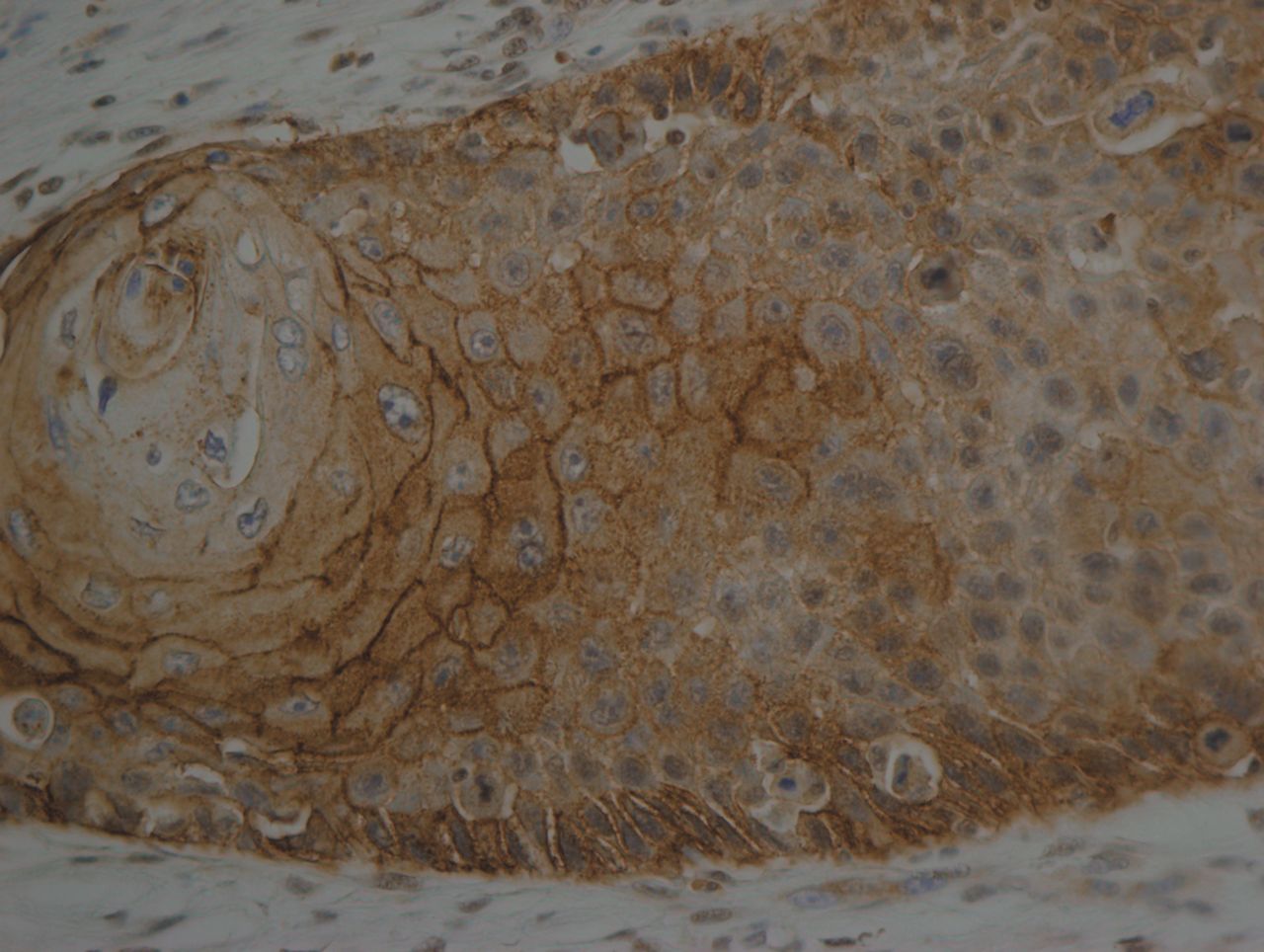
Immunohistochemical expression of claudin 1 in oral squamous cell carcinoma, well differentiated type. Strong membranous immunostaining (H&E, original magnification ×40).
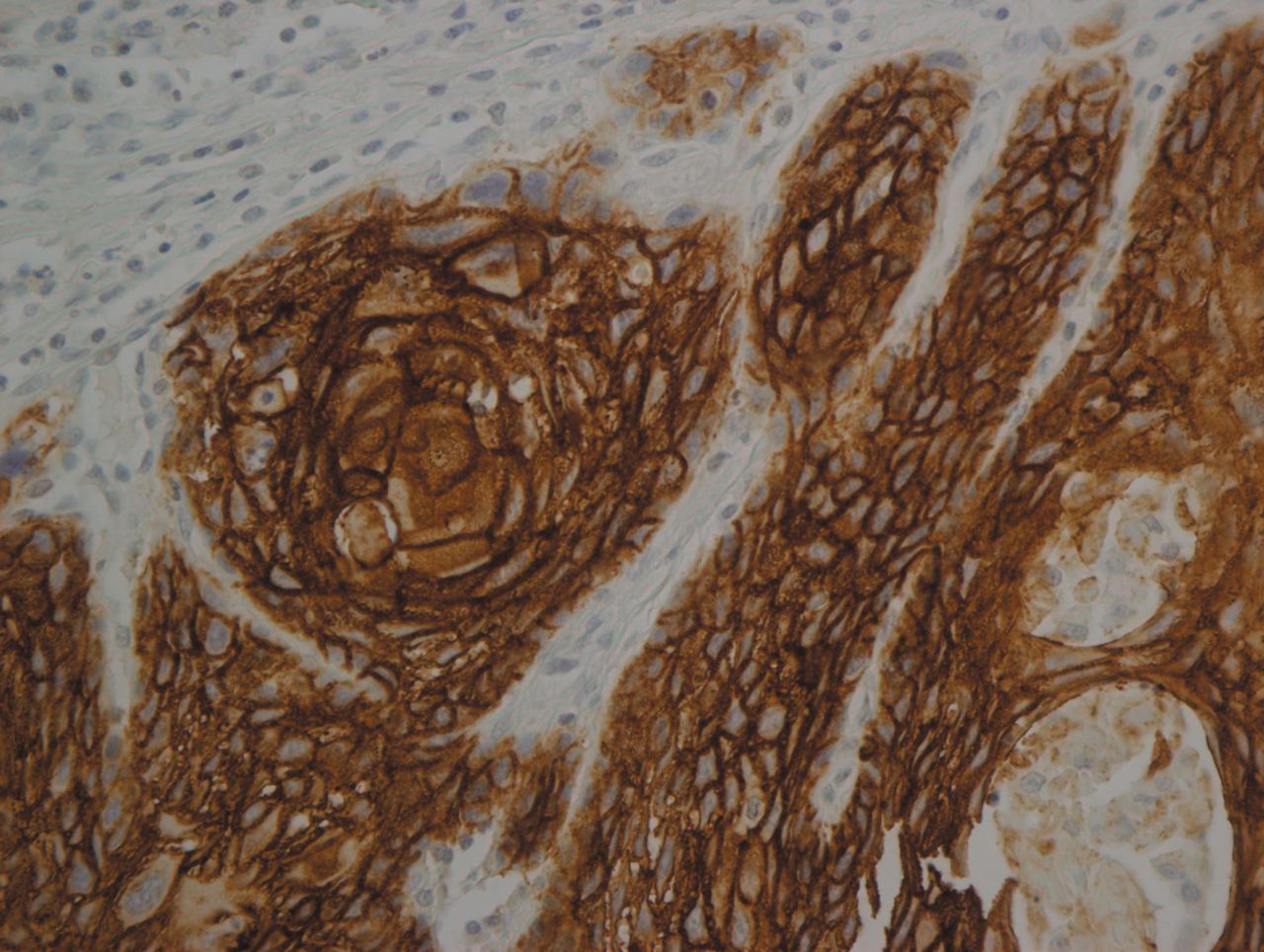
Immunohistochemical expression of claudin 4 in oral squamous cell carcinoma, well differentiated type. The immunostaining was stronger in the invasive front compared to the inner part of the tumor (H&E, original magnification ×40).
Immunohistochemistry. The formalin-fixed, paraffin-embedded tissues were cut into 4-μm sections and dried on capillary-gap glass slides (DakoCytomation, Dako, Carpinteria, CA, USA). The sections were deparaffinized with standard xylene and hydrated through graded alcohol into water. Antigen retrieval was performed using Target Retrieval Solution pH 9.0 for claudin 1 and pH 6.0 for claudin 4 in PTLink (Dako). Staining was carried out at room temperature on an automatic staining workstation (Dako Autostainer Plus) with rabbit IgG polyclonal antibody to CLDN1 (Catalog No. RB-9209-P; Thermo Scientific, Waltham, MA, USA,) at 1:100 dilution for 20 min, and rabbit IgG polyclonal antibody to CLDN4 (Catalog No. RB-9266-P, Thermo Scientific, Waltham, MA, USA) at 1:50 dilution for 20 min. The Dako EnVision Flex-+ Visualization System (Dako Autostainer) was used. Counterstaining with hematoxylin was the final step. After staining, the slides were dehydrated through graded alcohols and mounted with a coverslip using a standard medium. A negative control with an omission of the anti-serum from the primary incubation was also included. Breast carcinoma and tonsil samples were used as positive controls for CLDN1 and -4, respectively.
In this study two independent examiners evaluated both the intensity of immunohistochemical staining and the proportion of the stained tumor cells. Staining intensity was further classified as follows: (+) weak, (++) moderate, or (+++) strong. Positively stained cells were quantified as a percentage of the total number of tumor cells. In addition, we also evaluated the location of the staining in the tumor masses (invasive front, center, or the whole tumor masses), and tumor cell staining (membrane, cytoplasm, nucleus).
Statistical analyses. Categorical data were compared using χ2 or Fisher's exact tests. Cause-specific survival time was calculated from the time of diagnosis (which was never performed more than 21 days prior to surgical treatment) until the time of death. The Kaplan Meier method was used to estimate the survival curves, and the comparison between survival functions for different strata was assessed with log-rank analyses. Multivariate Cox proportional hazards model was used to examine the relative impact of variables shown to be statistically significant in univariate analysis or variables likely to have an effect on the outcome. All tests were two-sided with p-values ≤0.05 as the threshold to be considered statistically significant. All statistical analyses were performed using the computer package PASW Statistics 18 (SPSS Inc., Chicago, IL., USA).
Results
Immunohistochemical analysis of CLDN1 and CLDN4 expression was carried out on tissue sections from 65 OSCCs and normal oral mucosa as internal control, and we attempted to correlate the expression of these proteins with clinicopathological parameters and cause-specific survival in this series. CLDN1 and CLDN4 immunoexpression were not correlated (p=0.63). CLDN1 was expressed in normal oral epithelium, but not in its basal layer.
CLDN1 protein expression in OSCC. In 61 out of 65 (93.9%) tumors, CLDN1 was expressed in a membranous pattern, while in two cases (3.1%), staining in the tumor was only cytoplasmic. In the remaining two cases, no immunoexpression was observed. The typical immunohistochemical expression pattern of CLDN1 is shown in Figure 1. This expression was variable between cases: Eight (12.3%) cases showed weak expression; 21 (32.3%), moderate expression, and 34 (52.3%) cases showed strong expression. CLDN1 staining was seen in all areas of OSCC. In 24 (37%) cases, CLDN1 immunostaining was observed in the invasive front of tumor nests or cords, while in 33 (51%), the presence of CLDN1 was detected in the center of tumor areas. In the remaining six cases (9%), simultaneous central and peripheral immunoexpression was observed.
In univariate analysis (Table II), immunoexpression in the invasive front of the tumors was associated with neck node status (Fisher's exact test, p=0.04), and that in tumor cells was positively associated with tumor stage (Fisher's exact test, p=0.05). However, there was no statistically significant relationship between CLDN1 tumor and cell immunoexpression patterns and clinical variables such as gender, histological grade, tumor size, disease recurrence, and tobacco or alcohol consumption. The intensity of CLDN1 immunostaining was associated with female gender (Fisher's exact test, p=0.03), and negatively associated with tobacco consumption (Fisher's exact test, p=0.02) (Table III), but not with the other studied variables.
CLDN4 protein expression in OSCC. Immunostaining for CLDN4 occurred in a predominantly membranous pattern. Of the 65 tumors investigated, 36 (55.4%) showed CLDN4 immunoreactivity, with 14 (21.5%) samples displaying a cytoplasmic staining. No immunoexpression was observed in the remaining 15 (23%) cases. Out of the OSCC samples investigated, 17 (26.2%) cases showed weak expression; 18 (27.7%), moderate expression, and 15 (23.1%) cases showed strong expression (Figure 2). In 15 (23%) cases, CLDN4 immunostaining was observed in the tumor front, while in 30 (46.2%), the presence of CLDN4 was detected in the center of tumors. In the remaining five cases (7.7%), both central and peripheral immunoexpression was observed.
When we compared CLDN4 expression by clinicopathological parameters, we found that the tumor cell membranous immunostaining pattern was associated with well-differentiated histological grade (Fisher's exact test, p=0.01) (Table IV). CLDN4 staining intensity was also significantly correlated with tumor differentiation (Fisher's exact test, p=0.05) and tumor recurrence (Fisher's exact test, p=0.03) (Table V). However, our findings revealed no significant correlation between the expression of CLDN4 and gender, tobacco or alcohol consumption, T size and N stage (Tables IV and V).
Survival analysis. At the conclusion of the study, 31 patients (48%) were alive and free of disease, while 15 patients (23%) had died or had a non-treatable disease; the remaining 19 (29%) were lost to follow-up. The mean and median disease-specific survival times from treatment were 194.7 months, and 249 months, respectively. The 5- and 10-year cause-specific survival rates were 45% and 26%, respectively. As the univariate analysis shows (Table VI), tumor size (T), neck node status (N), clinical stage, tumor recurrence, tumor cell cytoplasm staining by CLDN4, and CLDN4 immunoexpression intensity were predictive at p<0.05 of cause-specific survival. As shown in the Cox univariate analyses (Table VI) a 6.37 increase in the HR was observed when tumor size was T3 or T4 compared to T1 or T2. Patients with T1 and T2 tumors showed a survival of 90%, compared to 54% in T3 and T4 patients. In addition the mean survival time is significantly shorter in T3 and T4 cases compared to T1 and T2. When the neck node status was N3, the HR was more than 8-fold higher compared to those with N0. Interestingly, in our study, tumor recurrence was the variable which had the highest relative risk (HR=29.5) for poor survival. Among the immunohistochemically studied variables, only CLDN4 presented immunoreaction in the membrane of tumor cells, and a low intensity of CLDN4 immunostaining was associated with a poor survival.
Statistical relationship between intensity of staining for CLDN4 and several clinicopathological characteristics.
In the Cox proportional hazards model analysis, with the exception of the neck node status, disease recurrence and intensity of CLDN4 immunoexpression in tumor cells, the remaining clinical, pathological and immunohistochemical variables were no longer associated with cause-specific survival after adjustment in the Cox multivariate analysis (Table VII). In a multivariate analysis for disease recurrence, only tumor size and CLDN1 tumor immunostaining (center versus invasive front) were of statistical significance (Table VIII).
Discussion
In the present study, we evaluated the immunoexpression patterns of CLDN1 and −4 in OSCC. The intercellular junctions serve two roles: they mechanically link cells, and they generate signals that are sent to the interior of the cell to report on the extent of contact with neighboring cells and the extracellular matrix (10). One of the hallmarks of malignant transformation of epithelia is that these connections are lost (13). Recently, several studies have demonstrated aberrant expression of claudins in many tumor types (18, 19, 22-24, 27-29). Among the claudin subtypes, the expression of CLDN1 and CLDN4 are frequently altered in various tumor types. CLDN1 was the first member of this family to be identified, it forms the backbone of TJs and is crucial for epithelial barrier function (30). A number of studies found CLDN1 is directly involved in the progression of several cancer types, including OSCC (8), and in which CLDN1 overexpression was associated with advanced disease stage (18). In fact, CLDN1 can function as a cancer-promoting and tumor-suppressive factor depending on cancer type (21). CLDN1 expression increases in colon cancer, particularly in metastatic tissues with mislocalization from the cell membrane to the cell nucleus and cytoplasm (31). In OSCC cells, this protein promotes invasion by up-regulating the activity of matrix metalloproteinases (MMPs) (8). In our study, we did not find any relationship between the intensity of CLDN1 immunoexpression and the clinicopathological variables studied. This lack of correlation between CLDN1 overexpression and patient outcomes is likely due to the applied treatment, which in all cases included a therapeutic or elective neck dissection that increased survival of patients (32). Our findings are partially in concordance with the analysis by Pintor dos Reis et al., which found an association between CLDN1 expression and angiolymphatic and perineural invasion (1), but not with the clinicopathological parameters studied herein. When we compared our work to that of Ouban et al. (33) it appears that CLDN1 immunoexpression showed different associations with clinicopathological variables. Specifically, they found a correlation of CLDN1 with histological grade or cellular differentiation, with strong expression in well-differentiated tumors, and loss of expression in less differentiated areas. This allowed us to speculate that well-differentiated tumors up-regulate CLDN1 to increase their invasive potential, while poorly differentiated tumors may use other mechanisms to regulate invasion (34). In fact, Dhawan et al. stated that CLDN1 overexpression induces epithelial-mesenchymal transition and down-regulates expression of E-cadherin in metastatic cancer colon cells (31). However, we did not find any association between CLDN1 expression and tumor differentiation. Some studies have suggested that up-regulation of certain claudins potentially contributes to carcinogenesis by altering TJ function (34). Claudins increase the concentration of MT1-MMP and activate pro-MMP2 (35). Laminin is an important component of the basement membrane, and together with integrin forms hemi-desmosomes (36). The laminin-5 γ2 chain is cleaved by MT1-MMP and MMP2, and the cleaved γ2 chain binds epidermal growth factor receptor (EGFR) on cancer cell surfaces and transmits intracellular signals that promote cell growth and mobility (37). Oku et al. suggest that CLDN1 up-regulates cancer cell invasion activity through activation of MT1-MMP and MMP2 (8). In addition, Dhawan et al. report that when CLDN1 synthetic small-interfering RNA (siRNA) was introduced into a metastatic cell line highly overexpressing CLDN1, its invasive activity was markedly suppressed (31), suggesting that CLDN1 positively regulates cancer cell invasion. In our study, the presence of CLDN1 in the invasive front of tumor masses was more frequently (68%) associated with neck node metastasis compared to N0 cases (40%). As was previously said, the expression of claudins depends on the cell type and tissue. In colonic cancer, reduced expression of CLDN1 is a strong predictor of disease recurrence and poor patient survival (38), and, in breast cancer, it correlates with recurrence (39). Cancer cells showed higher expression of CLDN1 than that of normal epithelia, while in those cancers which start in glandular tissue, such as in the breast and colon, the disappearance of CLDN1 is more characteristic (40).
Univariate survival analysis of clinicopathological variables using Kaplan-Meier and Cox modelling.
Multivariate survival analysis by prognostic factors using Cox proportional hazards modelling.
CLDN4 is a component of TJs, critical for sealing cellular sheets and controlling paracellular ion flux (34). It has been reported that knockdown of CLDN3 and CLDN4 was accompanied by reduced expression of E-cadherin, enhanced migration, increased invasion, and greater metastasis (41). Knockdown of CLDN4 produces an increase in Ser9 phosphorylation of which reduces its ability to mediate the degradation of β-catenin (41). The expressions of CLDN1 and CLDN4 seemed not to be associated with many clinicopathological parameters determined in our patients, although there were some exceptions. In the present study, we found that CLDN4 immunoexpression was significantly associated with histological differentiation and recurrence in OSCC. The well-differentiated group exhibited a high expression of CLDN4 compared to the moderate-differentiated group. In addition, a reduced expression of CLDN4 was correlated with tumor recurrence, which leads to the conclusion that those OSCC that do not overexpress CLDN4 should behave more aggressively. One of the most important mechanisms of claudin gene expression seems to be related to epigenetic regulations, and methylation of 5’-cytosines in CpG islands plays a key role in epigenetic modulation. Sung et al. demonstrated that decreased expression of CLDN4 is associated with poor prognosis in esophageal squamous cell carcinoma and is related to hypermethylation of its promoter (28). CLDN4 is frequently overexpressed in ovarian, pancreatic, prostate, and urothelial cancers, and this overexpression is associated with poor prognosis (40). CLDN4-based implications in prognosis vary depending on the type of organ affected. CLDN4 overexpression in ovarian cancer may lead to an increase in invasion, motility and tumor cell survival (27); conversely, in pancreatic carcinoma, CLDN4 overexpression has been associated with significantly reduced invasiveness (42). The role of CLDN1and -4 for prognosis remains controversial. Michal et al. observed that CLDN4 overexpression in pancreatic carcinoma was associated with significantly reduced invasiveness both in vivo and in vitro (42). On the other hand, Agarwal et al. stated that CLDN4 overexpression may lead to an increase in invasion, motility and tumor cell survival (27), as has been shown in endometrial carcinoma (43). Taken together all these results suggest that the immunoexpression of claudins may vary depending on the cells, tissues and organs of the body. It is possible that different cells in different environments or tissues contribute to different distribution and expression levels of claudins. The mechanism by which claudin overexpression may contribute to tumor progression is not clear, but it is possible that functional implications of claudins can differ among organs. From a theoretical point of view at least, claudin overexpression should result in enhanced cell adhesion and decreased tumor aggressiveness; however, the reverse seems to be the case. Resnick et al. have suggested that up-regulation of claudins may interfere with TJs formation, and may also affect cell signaling pathways through their interaction with ZO1, which in turn interacts with various signaling proteins, such as the RAS substrate, AF6 proteins, and connexin 43 (44). These results suggest that in tumors, claudins may have different functions not related to the formation of TJs. Specifically, Li et al. reported that cells expressing CLDN4 secrete factors that can mediate angiogenesis (45).
Multivariate survival analysis by prognostic factors using Cox proportional hazards modelling.

Kaplan Meier survival curve among oral squamous cell carcinoma patients defined by the intensity of claudin 4 immunostaining (p=0.03).
In this study, we observed mislocalization of CLDN1 and CLDN4 to the cytoplasm, but only the mislocalization of CLDN4 had prognostic relevance. In particular, the presence of CLDN4 in the cytoplasm of tumor cells was related to a higher patient survival compared to immunostaining located only in the cell membrane. Conversely, Blanchard et al. observed mislocalization of CLDN1 in breast cancer, and an increase in invasiveness of cancer cells (46). Consequently, the relationship between CLDN4 immunoexpression and patient survival is controversial. In our case, we found that CLDN4 overexpression was associated with prolonged survival. The reasons for these discrepancies may be explained by the different tumor types used in each study. In esophageal cancer, claudin expression patterns appear to be different between adenocarcinomas and squamous cell carcinomas (28). In our study, only squamous cell carcinomas were included.
Conclusion
To sum up, we showed an association of CLDN1 with neck node status, clinical stage and disease recurrence in OSCC. It is worth noting that only CLDN4 was associated with patient survival, both in univariate and multivariate analyses. Our study strongly suggests that CLDN4 is a promising new candidate marker for predicting the outcome of patients affected with OSCC, whereas CLDN1 may be a useful prognostic marker for determining patients that are at a higher risk for recurrence.
Acknowledgements
This work was supported by a grant for scientific research from the Ministry of Health, Spain (Instituto de Salud Carlos III, PI070675). The Authors wish to thank Marino Santirso, who acted as language consultant for the final edited version.
- Received January 21, 2015.
- Revision received February 7, 2015.
- Accepted February 10, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Polymorphisms in CLDN1 are associated with age and differentiation of triple-negative breast cancer patients
- Tight Junction Protein Claudin-2 Promotes Self-Renewal of Human Colorectal Cancer Stem-like Cells
- Risk Factors Associated with Disease Recurrence in Patients with Stage III/IV Squamous Cell Carcinoma of the Oral Cavity Treated with Surgery and Postoperative Radiotherapy