


Abstract
Background: Over the last years, evidence has accumulated that an increased expression of pyruvate kinase M2 isozyme (PKM2) is related to neoplastic transformation as well that its plasma concentrations might be a marker of lung cancer progression. Materials and Methods: In the present manuscript an immunohistochemical technique was used to detect the expression of two pyruvate kinase isoforms: PKM1 (muscle isozyme of PK) and PKM2 as well Ki-67 antigen on paraffin sections of 218 cases of non-small cell lung cancer (NSCLC) of different histological types and grades of malignancy. Results: A significant correlation between expressions of both pyruvate kinase isoforms in all NSCLC types was found (r=0.42, p<0.0001). Expression levels of PKM1 and PKM2 were independent of the histological classification of the tumor and patients' clinicopathological data. Conclusions: PKM2 and PKM1 have no value as predictive markers of NSCLC regardless of the histological type and grade of malignancy.
Lung cancer is the leading cause of cancer-related death worldwide and a trustworthy diagnosis of patients is crucial for a successful therapy of the disease. It is the most frequent malignant tumor in men and despite advances in diagnosis and treatment, prognosis remains unfavorable (1). However, European cancer mortality predictions for lung cancer in 2013 report a continuing reduction in males, but a continuing increase in females. For the first time in females, mortality from lung and breast cancers should be equivalent (2, 3).
Pyruvate kinase (PK), catalyzing the rate-limiting final step of glycolysis, is a regulatory enzyme of the mentioned pathway. In mammals, four isoforms of pyruvate kinase have been distinguished. The L and R isozymes are expressed, in liver and red blood cells respectively, whereas the M1 isoform, which is the predominant isozyme of PK in striated muscle, is widely expressed in most tissues. The M2 isoform is a splice variant of the M1 and it is expressed during embryonic development (4, 5).
Interestingly, it has been shown that PKM2 plays an important role during carcinogenesis (4) and it is suggested that tissues neoplastically changed exclusively express the M2 isoform (5, 6). Several studies on the expression of PKM2 in various tumors (i.e. lung, breast, renal, colon and rectal) revealed that an increased expression of PKM2 correlates with the grade of malignancy (5, 6). It was also shown that plasma levels of PKM2 might be a marker for monitoring lung cancer disease (7). The involvement of PKM2 in the process of tumorigenesis and proliferation suggests that the level of the enzyme expression correlates with the stage of cancer disease.
The aim of the present study was to evaluate the efficiency of PKM2 and PKM1 as markers of different as well-histological types of non-small cell lung cancer (NSCLC) defining grades of malignancy in lung cancer disease.
Materials and Methods
Patients. All the procedures and protocols used in this study were approved by the Commission of Bioethics at Wroclaw Medical University. The study was performed on archival 218 cases of NSCLC embedded in paraffin blocks (96 squamous cell carcinomas; – SQC, 104 adenocarcinomas; – AC and 18 large cell carcinomas; – LCC). Patients were operated between 1997-2011 at the Lower Silesian Centre of Pulmonary Diseases in Wroclaw and specimens were obtained before treatment initiation. Clinical and pathological data of the study cohort are presented in Table I. The whole study group was followed up for 29.64±36.15 (range 1-147) months. During this period, 114 (52.3%) of the patients died of their disease.
Clinicopathological features.
Immunohistochemistry (IHC). Reactions were performed on the whole patient cohort. The paraffin sections, stained with haematoxylin/eosin (HE), were used to verify the diagnosis and grade of tumor malignancy. Briefly, IHC was performed on 4-μm thick paraffin sections according to a previously established protocol (8). Target Retrieval Solution, in a PT Link Rinse Station was used to deparaffinize the sections and retrieve the antigens (pH 9.0 for PKM1 and PKM2, and pH 6.0 for Ki-67; 97°C, 20 min) (DakoCytomation, Glostrup, Denmark). The sections were then washed in TBS/0.05% Tween buffer and endogenous peroxidase was blocked using EnVision FLEX Peroxidase-Blocking Reagent (5-min incubation at room temperature; RT) (DakoCytomation). Subsequently, the sections were washed in TBS/0.05% Tween and primary antibodies directed against PKM1 (15821-1-AP, 1:200, Proteintech, Chicago, IL, USA), PKM2 (15822-1-AP, 1:200, Proteintech) and Ki-67 (MIB-1; ready-to-use, DakoCytomation) were applied and incubated at RT for 20 min in an automated staining platform (Link48 Autostainer, DakoCytomation) to ensure repeatable reaction conditions. After washing the sections in TBS/0.05% Tween, EnVision FLEX/horseradish peroxidase (HRP) secondary antibodies were applied (20 min at RT) (DakoCytomation). Sections were then washed in TBS/0.05% Tween and EnVision FLEX the substrate for peroxidase, diaminobenzidine (DAB+ chromogen), was applied and the sections were incubated for 10 min at RT. Finally, the sections were counterstained with Mayer's haematoxylin, dehydrated in alcohol (70%, 96%, 99.8%) and xylene and then mounted using SUB-X Mounting Medium (DakoCytomation).
Negative controls were prepared by omitting the primary antibody, whereas tumor sections known to have high expression of the analyzed marker were used as positive control.
Evaluation of IHC reactions. IHC reactions were analyzed under a BX-41 light microscope (Olympus, Tokyo, Japan). Expression of PKM1 and PKM2 was evaluated in the cytoplasm of cancer cells utilizing a 12-point semi-quantitative immunoreactive score (IRS) according to Remmele and Stegner (9), also used in our previous study for MT-I/II and MT-III assessment in NSCLC (1, 8). The scale is based on the percentage of tumor cells showing positive reaction (0: absence of cells with positive reaction, 1: 1-10% cells, 2: 11-50%, 3: 51-80%, 4: over 80% cells with positive reaction), as well as the intensity of the reaction (0: no reaction, 1: low intensity reaction, 2: moderate intensity reaction, 3: intense reaction). Nuclear expression of Ki-67 antigen expression was evaluated in whole-tumor sections, as previously described using a semi-quantitative five-grade scale based on the proportion of cancer cells with reaction product and is encoded as follows: 0 points: absence of reaction, 1: 1-10% cells with positive reaction, 2: 11-25%, 3: 26-50%, 4 points: more than 50% cells with positive reaction (1).

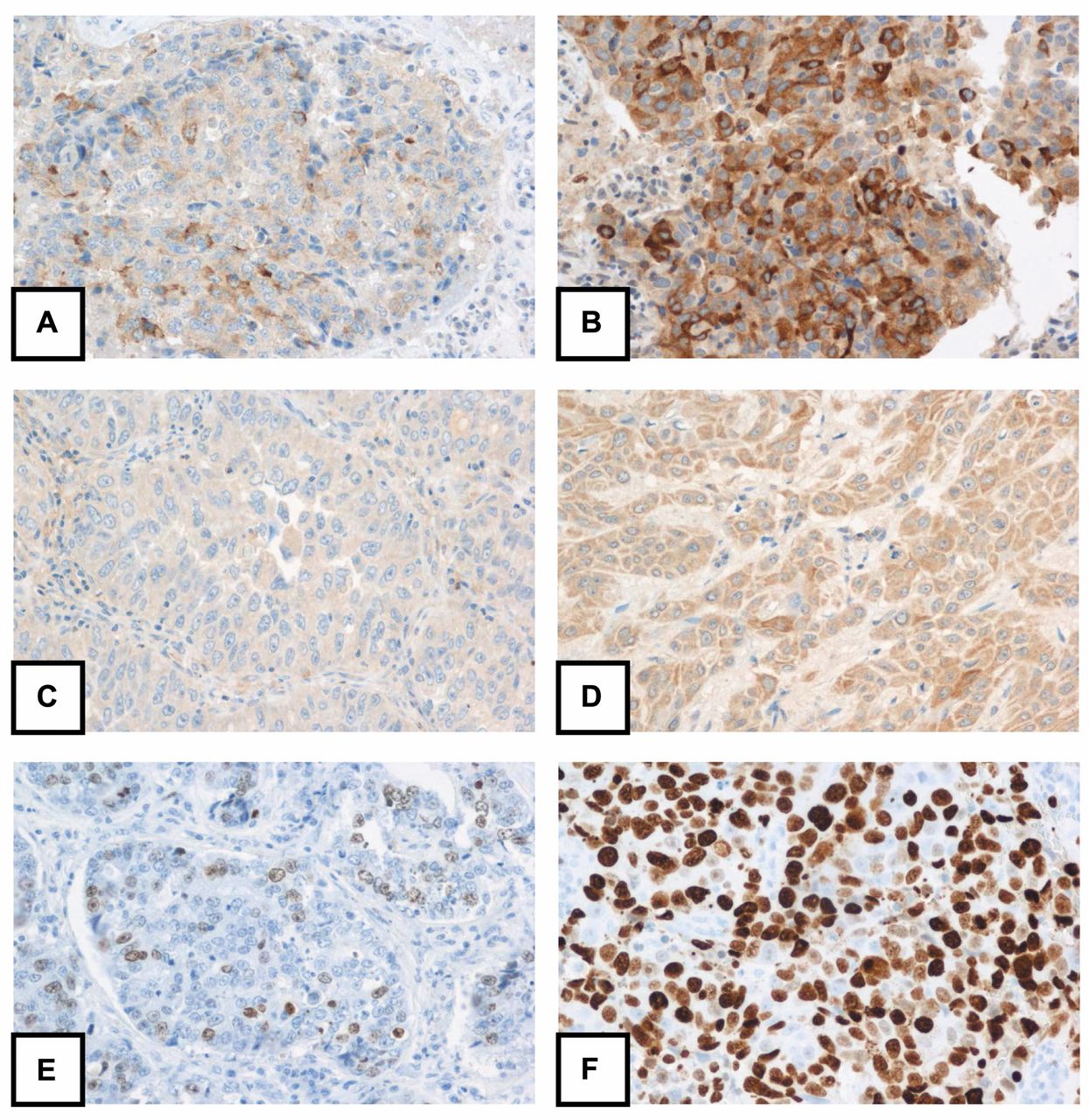
Expression of pyruvate kinase 1 (A, B), pyruvate kinase 2 (C, D) and the Ki-67 antigen (E, F) in cancer cells of non-small cell lung cancer. Weak (A, C, E) as well as strong (B, D, F) immunoreactivity of the studied antigens can be noted. Magnification ×200.
Statistical analysis. The Prism 5.0 (GraphPad, La Jolla, CA, USA) statistical software was used to analyze the obtained results. Relationships between the expression of the studied antigens and patients' clinicopathological parameters were analyzed using the Kruskal-Wallis, Mann-Whitney U-test, Fisher's exact and Spearman's correlation tests. The Kaplan-Meier method and the log-rank test were used to analyze patient survival. For each variable, the hazard ratio (HR) and 95% confidence interval (CI) were estimated. Results were considered statistically significant when p<0.05.
Results
Expression of PKM1, PKM2 and Ki-67 antigen. Cytoplasmic PKM1 expression was noted in cancer cells of 204 out of the 218 (93.6%) analyzed cases. Out of these 135 (61.9%) were characterized by low expression (IRS 1-4) (Figure 1A), whereas 79 (36.3%) presented high PKM1 immunoreactivity (IRS 6-12) (Figure 1B). Similarly, PKM2 expression was noted in the cytoplasm of NSCLC cancer cells in 197 out of the 218 (90.4%) analyzed cases. Low PKM2 (IRS 1-4) immuoreactivity was noted in 144 (66.1%) cases (Figure 1C), whereas 53 (24.3%) cases were characterized by high (IRS 6-12) PKM2 expression (Figure 1D). The Ki-67 antigen expression was observed in cancer cells nuclei of all the analyzed cases. One hundred one samples (46.3%) were characterized by its low expression (scores 1 and 2) (Figure 1E), whereas in 117 (53.7%) its high expression (scores 3 and 4) was noted (Figure 1F).

Correlations (Spearman correlation test) between pyruvate kinase 1 (PKM1), pyruvate kinase 2 (PKM2) expression in the whole patients cohort (A; r=0.42, p<0.0001), squamous cell carcinoma (B; r=0.37, p<0.0001) and adenocarcinoma (C; r=0.44, p<0.0001) cases.
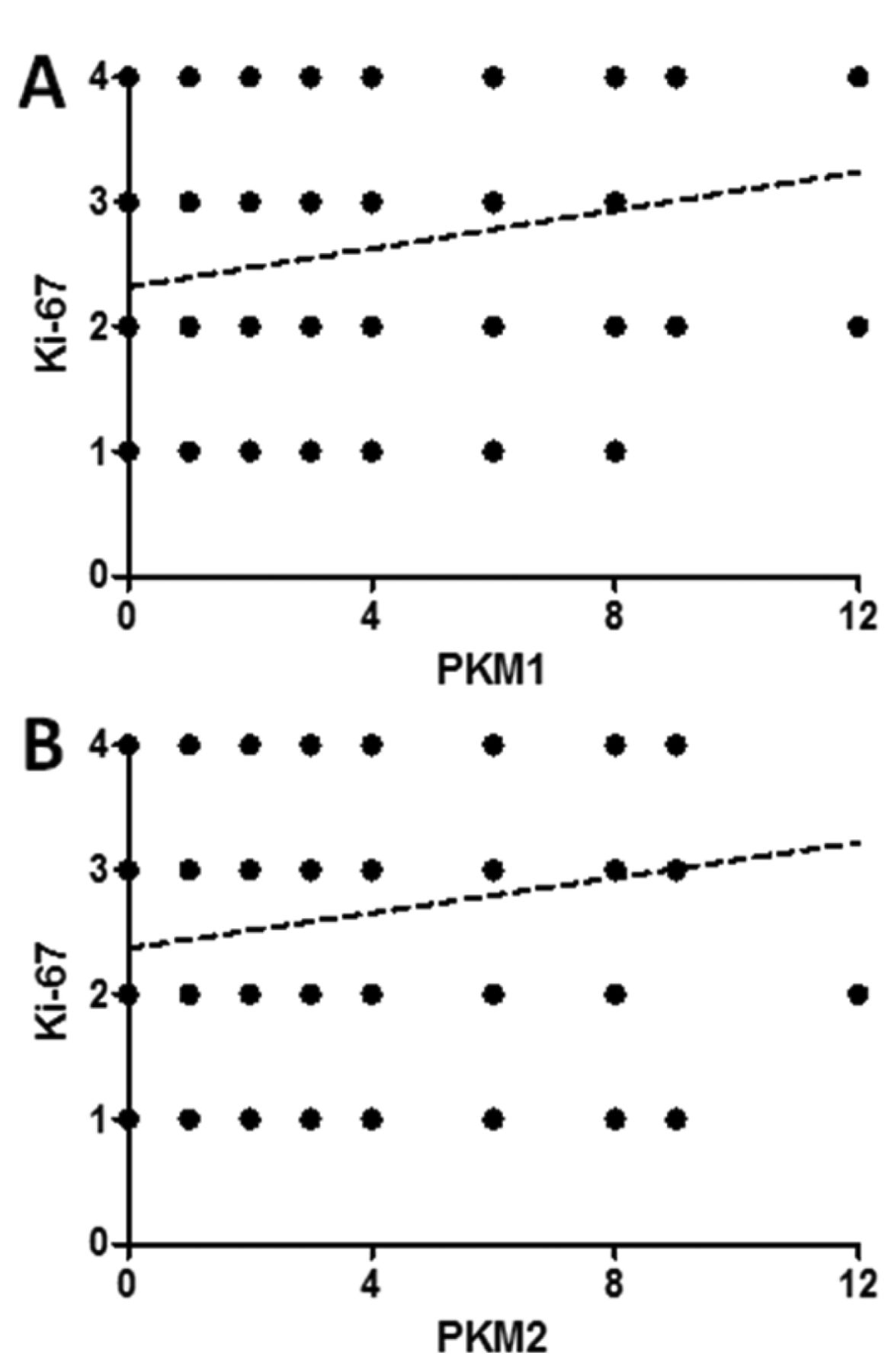
Correlations (Spearman correlation test) between the expression of the Ki-67 antigen and the expression of pyruvate kinase 1 (PKM1; r=0.17, p=0.014; A) and pyruvate kinase 2 (PKM2; r=0.16, p=0.016; B) in the 218 analyzed non-small cell lung cancer patients.
Spearman test revealed significant, moderate positive correlations between PKM1 and PKM2 immunoreactivity in the whole patients' cohort (r=0.42, p<0.0001) as well in SQC (r=0.37, p<0.0001) and AC (r=0.44, p<0.0001) cases (Figure 2). Significant positive correlations were found between the expression of PKM1 and the Ki-67 antigen in the whole cohort of patients (r=0.17, p=0.014; Figure 3A). Similarly, PKM2 correlated with the Ki-67 antigen expression in the whole patients' cohort (r=0.16, p=0.016; Figure 3B). Almost significant correlation of Ki-67 antigen with PKM1 and PKM2 expressions were noted in the SQC cases (r=0.18, p=0.068, and r=0.19, p=0.063; respectively).
Relationship between expression of pyruvate kinase M1 (PKM1), pyruvate kinase M2 (PKM2) and Ki-67 antigen and selected clinicopathological parameters for a group of 218 patients with NSCLC. Significant p-values are given in bold.
Relationship between immunohistochemical markers expression and patients' clinicopathological data. Significantly higher PKM1 expression was noted in NSCLC cancer cells of female patients as compared to men in the whole patients' cohort (IRS 4.75±2.50 vs. IRS 3.81±2.33, p<0.018; Mann-Whitney U-test). However, no differences were noted when SQC and AC cases were analyzed separately in regard to patients sex. Statistical analysis revealed no significant differences between expression intensities of PKM1 and PKM2 with patients' age tumor, histological type, primary tumor size, presence of lymph node metastases, stage of the disease and malignancy grade in all the analyzed cases (Table II). Similarly, no significant relationships between PKM1 and PKM2 expressions were noted when the data was analyzed only in the SQC and AC cases.
Prognostic value of analyzed IHC markers expression in NSCLC. Univariate survival analysis (Mantel-Cox test) of the analyzed patient cohort revealed that advanced patients age (>65 years) at diagnosis (p=0.0089), AC histological subtype (p=0.026), larger primary tumor size (p=0.0193), presence of lymph node metastases (p<0.0001) and advanced disease stages (stage 2A-4; p<0.0001) were associated with poor overall survival (OS). Immunoreactivity of PKM1 and PKM2 had no impact on patients OS in the whole study cohort (Table III), as well as in particular histological type of NSCLC.
Discussion
Pyruvate kinase (PK) catalyzes, practically irreversibly, the last step of glycolysis, in which pyruvate and ATP are formed. All PK isozymes are tetramers, however, PKM2, in contrast to the other PK isoforms, may undergo reversible dissociation into dimers that are thought to be practically inactive forms of the enzyme (2). The ratio of the active tetramers to the inactive dimers determines whether glucose is oxidized to lactate for energy production or used by the pentose phosphate pathway for the synthesis of compounds needed for cell proliferation, i.e. NADPH and ribose (5, 6). The balance between tetramers and dimers of PKM2 is controlled by fructose-1,6-bisphosphate and oncoproteins as A-Raf, HPV-16 E7 and pp60v-src kinase (5, 6). These unique properties, make PKM2 an excellent candidate for being a regulating factor of cell's growth and proliferation. Indeed, the high expression of PKM2 was found in embryonic and proliferating adults tissues. Moreover, there are studies showing expression of this protein in cancer (5, 6). Subsequently, it has been shown that during neoplastic transformation, the tissue-specific PK isoforms (i.e. PKR, PKL, PKM1) disappeared whereas PKM2 expression was increased (10-12). It was also demonstrated that the switching of PK expression to the M2 isozyme led to aerobic glycolysis (Warburg effect) and this correlated with promotion of tumorigenesis (13). Furthermore, it was also shown that PKM2 is a multifunctional protein possibly playing the role of a nuclear protein regulating cancer cell growth and survival (5, 6, 14, 15). Collectively, these data point to PKM2 as predictive marker of cancers. In line with this, some clinical studies demonstrated that PKM2 might be a marker for the detection of some cancers: gastrointestinal tumors (16), lung cancer (17-19) and renal carcinoma (20). Unfortunately, the pilot immunohistochemical study conducted by Schneider et al. (4 cases of various histological types and grades of lung cancer) revealed uselessness of PKM2 for precise diagnosis of cancer (7).
Univariate overall survival analysis of patients with NSCLC. Significant p-values are given in bold.
Our results presented in this manuscript confirmed those preliminary study findings (7). The level of PKM2 expression did not correlate with the type and grade of lung cancers despite the fact that the specimens studied by us significantly differed in their proliferative potential, which was confirmed by the Ki-67 evaluation. The only correlation observed in our study was a moderate positive correlation between PKM1 and PKM2 immunoreactivity. This demonstrates that the increased proliferation of lung cancer cells does not manifest in the elevation of PKM2 level. Our results also clearly show that there is no shift from PKM1 to PKM2 in lung cancers. These findings are consistent with the quantitative spectrometric analysis of Bluemlein et al. (21) who found that the relation of PKM2 to PKM1 in different cancers and matched control tissue is practically constant. Nevertheless, there is no switch in the expression of pyruvate kinase isoforms during carcinogenesis and PKM2 is a predominant isoform of PKM in all tissues. Our and Bluemlein et al. (21) investigations demonstrated that the titer of PKM2 in a cell is not crucial for cancer development and cancer-like metabolism. However, it does not implicate that PKM2 is not important for cell proliferation and cancer-like metabolic adaptations. Over the last decade, several lines of evidence have been delivered showing that post-translational modifications and interactions with oncogenes may regulate PKM2 activity, subcellular localization and moonlighting functions (5, 6).
Thus, presumably PKM2 modifications (e.g. oncogene-mediated phosphorylation and/or dimerization) are phenomena in which tumorigenesis affects cellular metabolism and survival. This implicates that the detection of cancer-specific modifications of PKM2 may be a promising method for monitoring cancer type and stage. Unfortunately, the precise correlation between cancer development and PKM2 modifications are still poorly-understood.
Acknowledgements
This research was supported by Polish Ministry of Science and Higher Education; Contract grant number: N N401 376139.
Footnotes
-
↵* These Authors contributed equally to this work.
- Received March 31, 2014.
- Revision received May 27, 2014.
- Accepted May 28, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}