


Abstract
Background/Aim: Known risks factors for bladder cancer progression and recurrence are limited regarding their prognostic ability. Therefore identification of molecular determinants of disease progression could provide with more specific prognostic information and could be translated into new approaches for biomarker development. In the present study we evaluated, the expression patterns of somatostatin receptors 1-5 (SSTRs) in normal and tumor bladder tissues. Materials and Methods: The expression of SSTR1-5 was characterized in 45 normal and bladder cancer tissue samples using reverse transcriptase-polymerase chain reaction (RT-PCR). Results: SSTR1 was expressed in 24 samples, SSTR2 in 15, SSTR3 in 23, SSTR4 in 16 and SSTR5 in all but one sample. Bladder cancer tissue samples expressed lower levels of SSTR3. Co-expression of SSTRs was associated with superficial disease. Conclusion: Our results demonstrate, for the first time, that there is expression of SSTR in normal and bladder cancer urothelium. Further studies are required to evaluate the prognostic and therapeutic significance of these findings.
Bladder cancer is the 4th most common cancer in males and the 9th most common cancer in females in developed countries (1). Urothelial (transitional cell) carcinoma is the prevalent histological type accounting for almost 90% of all bladder cancer cases (2). Nearly 70% of newly-diagnosed cases are superficial, i.e. tumors confined to the mucosa or sub-mucosa, so-called superficial non-muscle-invasive bladder cancers, with the remainder being muscle invasive.
The prognosis of patients with bladder cancer worsens with advancing stage. Five-year survival rates drop from 80-90% in superficial cancer to 5% in metastatic cancer (3). Risk factors for tumor progression and recurrence include prior tumor recurrence rate, number of tumors, tumor diameter, stage, grade and presence of carcinoma in situ (4). Unfortunately, these clinicopathological parameters are limited in their prognostic ability. Therefore, identification of molecular determinant of disease progression could provide with more specific prognostic information and could be translated into new approaches for drug and biomarker development (5).
Somatostatin is a neuropeptide that displays a broad range of biological actions including control of endocrine and exocrine secretions as well as inhibitory effects on the proliferation and survival of normal and tumor cells (6). These biological effects are mediated through interaction with the five known, specific somatostatin receptors subtypes (SST1-5). Somatostatin receptors are expressed on a number of human cancer cells. There are mainly two biologically-active forms of somatostatin: somatostatin-14 and somatostatin-28 (6, 7). Because of their very short plasma half-life (1-3 min), native somatostatins have a limited clinical role. Therefore, synthetic somatostatin analogues have been developed and used in different clinical settings. The effects of these compounds in cancer have been shown in several in vivo and in vitro studies (6-12).
Until now, no studies have examined the expression of somatostatin receptor subtypes in human bladder cancer. Therefore, the objective of this study was to determine the expression of five somatostatin receptors, (SSTR1-5), in normal and in cancerous bladder tissues and to investigate their expression is correlated to clinicopathological parameters.
Materials and Methods
Patients. We evaluated 73 bladder tissue samples from 64 patients who underwent cystoscopy under general anaesthesia in a large tertiary Hospital from August 2009 to October 2010. Samples were obtained from tumor, adjacent normal tissue and from normal-looking bladder mucosa. Samples were obtained with transurethral resection of bladder tissue or with cold cup biopsy based on the clinical indication. All patients had been informed of the study purpose and provided their written consent prior to participation, according to a protocol approved by the Institutional Ethics Committee (University of Athens, Greece). Diagnosis of bladder cancer was confirmed based on the histopathological evaluation and patients were classified based on the tumor node metastases (TNM) pathological staging and world health organization (WHO) grading system.
Collection of samples and qualitative detection of SSTRs mRNA by RT-PCR. Samples were immediately immersed in RNA later solution (Ambion, Austin TX) and frozen in liquid nitrogen and stored at −80°C. Subsequently, mRNA extraction was based on an in-house protocol of the laboratory of Experimental Physiology of Medical School University of Athens. All tissue samples underwent tissue homogenization using an Ultra Turrax T25 homogenizer (Fisher Scientific, Cheshire, UK) at 15,000-20,000 rpm for 15-30 sec and total cell RNA was isolated using Tri-Reagent Kits (MRC, Cincinnati, OH, USA) per the manufacturer's instruction. After homogenization samples were kept on ice for 30 sec and then were centrifugated in 12,000 × g for 5 min at 4°C. Following centrifugation, the supernatant was collected and transferred in 1.7-ml Ependorf tube in which was added 50 μl solution of 4-bromoanisole (MRC Inc., Cincinnati, Ohio, USA), left at room temperature for 5-15 min and then centrifugated at 2000 × g for 15 min at 4°C. Nearly 500 ml of supernatant were transferred in a new 1.7-ml Eppendorf tube which contained equal quantity of isopropanolol and then was centrifugated at 12000g for 12 min at 4°C. The supernatant was then removed and 1 ml of 75% ethanol was added. Following a new centrifugation at 8,000 × g for 5 min at 4°C, 50-100 μl of nuclease-free water was added and the solution was warmed at 60°C for 5 min followed by a quick spin for 2 sec. RNA concentration and purity was evaluated by spectrophotometry (Biospec-Nano, Shimadzu Inc.) by assessing the ratio of absorbance at 260 and 280 nm. Quality and integrity of total RNA was assessed by electrophoresis in 1% agarose gel. Extracted RNA was then reverse-transcribed to cDNA. SSTR expression in the samples and was evaluated by Polymerase Chain Reaction (PCR). For PCR a Master Mix PCR from Qiagen (Qiagen, GmbH, Hilden, Germany) was used from the Multiplex Kit of the company (MPCR Mix). PCR was performed using the PTC-200 Peltier Thermal Cycler (MJ Research Inc., Waltham, MA, USA). The products of the PCR were analyzed by agarose gel electrophoresis.
Statistical analysis. All statistical analyses were performed using R (Foundation for Statistical Computing, Vienna, Austria) (13). Categorical variables were compared using Fisher's exact tests.
Results
Out of 73 samples (59 cancerous tissues and 14 normal urothelium tissues) collected from 64 patients, 45 (34 cancerous and 11 normal) were adequate for further analysis with RT-PCR (Figure 1). Clinicopathological characteristics of the patients are presented in Table I.
There were 18 patients with stage Ta, 8 patients with pT1 and 8 patients with pT2. With regard to histological grade 10 patients were Grade I, 10 patients Grade II and 14 patients were Grade III.
Results of the RT-PCR are presented in Table II. Among the 24 samples that expressed SSTR1, 19 (79.1%) were cancerous and 5 (20.8%) were normal (p=0.73). Among the 19 cancerous samples that expressed SSTR1, 2 (10.5%) were muscle-invasive and 17 (89.4%) were superficial, 4 (21%) were recurrent and 15 (78.9%) were from initial tumor presentation. In total, SSTR1 was expressed in 19 out of 34 (55.8%) cancer samples and in 5 out of 11 normal samples (45.4%), in 2 out of 8 (5%) muscle-invasive cancers and in 17 out of 26 superficial cancers (62.9%) and in 4 out of 6 (66.6%) recurrent cases and 15 out of 28 (53.5%) initially presented cases. There was no statistical association between SSTR1 expression and bladder cancer (p=0.7), muscle invasive disease (p=0.1) and recurrence (p=0.67).
Among the 15 samples that expressed SSTR2, 9 (60%) were cancerous and 6 (40%) were normal. Among the 9 cancerous samples that expressed SSTR2, all were superficial and none was muscle-invasive 3 (33.3%) were recurrent and 6 (66.6%) were initially presented. In total, SSTR2 was expressed in 9 out of 34 (26.4%) cancerous samples and in 6 out of 11 normal samples (54.5%), in 9 out of 26 (34.6%) superficial cancers and in none of muscle-invasive tumors and in 3 out of 6 (50%) recurrent cases and in 6 out of 28 (21.4%) initially presented cases. There was no statistical association between SSTR2 expression and bladder cancer (p=0.14), muscle invasive disease (p=0.08) and tumor recurrence (p=0.31).
Among the 23 samples that expressed SSTR3, 14 (60.8%) were cancerous and 9 (39.1%) were normal. Among the 14 cancerous samples that expressed SSTR3, 4 (28.5%) were muscle-invasive and 10 were superficial (71.4%) and 2 (14.2%) of the 12 (85.7%) were initially presented. In total, SSTR3 was expressed in 14 of 34 (41.1%) cancerous and in 9 out of 11 normal samples (82%), in 4 out of 8 muscle invasive cases (50%) and in 10 out of 26 superficial cases (38.4%) and in 2 out of 6 recurrent cases (33.3%) and in 12 out of 28 (42.8%) initially presented cases. SSTR3 gene expression was significantly lower in bladder cancer samples compared to normal tissue samples (p=0.03). There was no statistically significant association between SSTR3 expression and muscle invasive disease (p=0.69) and tumor recurrence (p=1.0).
Among the 16 samples that expressed SSTR4, 12 (75%) were cancerous and 4 (25%) were normal. Among the 12 cancerous samples that expressed SSTR4, 2 (16.6%) were muscle invasive and 10 (83.3%), were superficial, 1 (8.3%) was recurrent and 11 (91.6%) were initially presented. In total, SSTR4 was expressed in 12 out of 34 cancerous samples (35.2%) and in 4 out of 11 normal samples (36.3%), in 2 out of 8 muscle invasive cancer (25%) and in 10 out of 26 superficial cases (38.4%) and in 1 out of 6 (16.6%) of recurrent and in 11 out of 28 (39.2%) initially presented cases. There was no statistically significant association between SSTR4 expression and bladder cancer (p=1.0), muscle invasive disease (p=0.68) and recurrent disease (p=0.39).
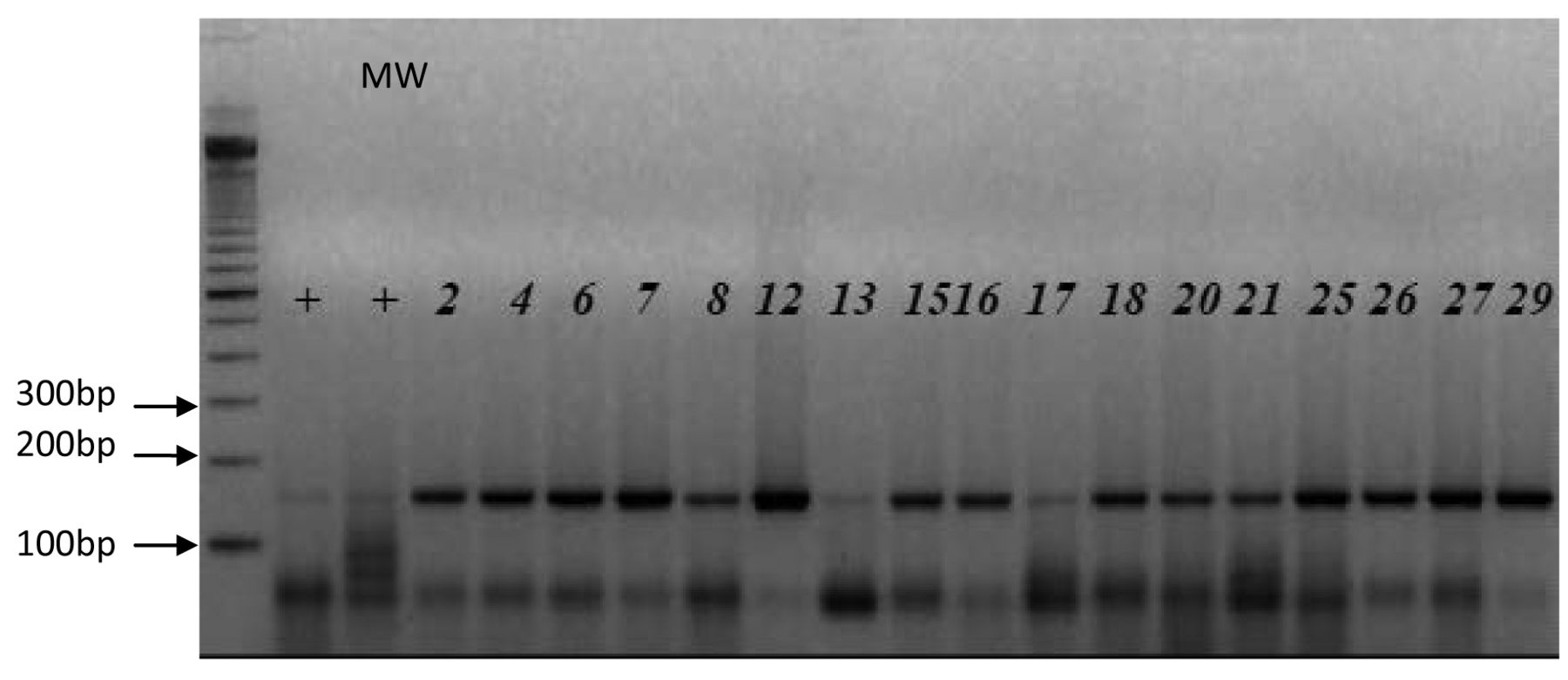
SSTR5 expression detected by semi-quantitative RT-PCR in human bladder in comparison to positive markers (+). The amplified DNA fragments were separated by agarose gel electrophoresis. Lane MW shows 100 bp marker (DNA ladder). Numbers correspond to numbered tissue samples. The PCR products correspond to the predicted size of 180 bp.
Clinicopathological characteristics of the patients.
SSTR5 was expressed in all but one sample. Therefore, no statistical analysis was performed.
When considering only the 34 cancerous samples, expression of only SSTR5 was noticed in 8 samples, in 8 there was co-expression between SSTR5 and one other SSTR (SSTR1 in 3 cases, SSTR2 in 1 case, SSTR3 in 2 cases and SSTR4 in 2 cases). In 17 cases more than 2 SSTRs were co-expressed in the samples, while in only one case there was no SSTR expression. Among the 8 cases that presented co-expression between SSTR5 and one other SSTR, there were 3 tumor recurrences (p=0.1) and there was no invasive disease (p=0.05). On the other hand, among the 9 cases with only SSTR5 expression there were 4 cases with muscle invasive disease and 2 recurrence cases.
SSTR expression in study samples. Summary of RT-PCR results.
Discussion
Bladder cancer is the second most common cancer of the genitourinary tract (1). Bladder cancer is a heterogeneous disease with a variable natural history. Superficial tumors frequently recur and 9% of them can progress to muscle invasive growth (14). Identification of superficial tumors with an adverse disease outcome from those unlikely to become invasive could provide individualized prognostications and allow for risk-stratified clinical decision making and appropriate treatment based on the tumors predicted natural history. For this reason, extensive effort have been made to identify genes and molecular pathways implicated in the development and progression of bladder cancer (5). Several reports have noted a role for the somatostatin receptor signaling pathway in different types of tumors (6). In the present study we evaluated for the first time, the expression of the five somatostatin receptors SSTR1 to SSTR5 in normal and in cancerous bladder tissues.
In our study, we demonstrated that SSTR1-5 are expressed in normal and cancerous bladder tissues. Almost all tissue samples expressed SSTR5 while SSTR1, 2, 3 and 4 were expressed in 53%, 33%, 51% and 35% of the samples, respectively. We also analyzed the co-expression pattern of the SSTRs. Co-expression of two SSTRs was observed in 30 samples whereas co-expression of three SSTRs was noticed in 24 samples. SSTR3 expression was significantly lower in bladder cancer compared to non-malignant bladder tissue samples. Our results suggest that the SSTR signaling pathway might play a role in bladder cancer progression. Current available data, thus far, have suggested an important role of the SSTR signaling pathway in cancer and cancer progression through multiple mechanisms which can be directly intergrated through cell-cycle arrest and inhibition of apoptosis downstream and indirectly through inhibition of angiogenesis and production of tumor growth factors (6). It is known that SSTR2 and SSTR5 are able to inhibit overexpression of growth hormone (GH) in acromegaly patients (15). GH in turn, increases the production of insulin growth factor-I (IGF-I) which has been shown to have an important role in oncogenesis (16). Additionally, somatostatin can inhibit angiogenesis via a pathway that mainly involves SSTR2 (17). The somatostatin signaling pathway is also able to participate in the control of cell-cycle arrest and apoptosis, whereas SSTR3 has been shown to increase wild-type p53 through a dephosphorylation-dependent conformational change (18, 19).
The biological effects of somatostatins are mediated through the SSTR1-5 receptors. These receptors differ in their signaling pathways, patterns of expression, pharmacological properties and cellular and tissue distributions. A feature common in all SSTRs is their ability to couple to Gi, to inhibit adenylate cyclase and to lower cAMP (20). On the other hand, SSTR1, 2 and 3 may exert anti-proliferative actions by activation of one or more protein tyrosine phosphatases (PTP), which in turn are associated with the MAPK pathway and the survival phosphatidylinositol 3-kinase pathway (6). Contrary, SSTR5 exerts its antiproliferative actions mainly through PTP-independent pathways (6).
Our results indicate a potential clinical benefit by targeting SSTRs in bladder cancer. Of particular note, our results are slightly different from those of other investigators who suggest a predominant expression of the SSTR2 in different types of tumors (21,22). We noticed a prevalent expression of SSTR5 in bladder tissues. Our results suggest that bladder neoplasms may be a likely target for treatment with high affinity multi-ligand binding analogs. Currently available long-acting analogues of somatostatin octreotide and lanreotide demonstrate a high affinity for SSTR2 and SSTR5. On the other hand, pasireotide (SOM 230) is a new SSTR analogue that additionally shows high affinity for SSTR1 and 3 (23).
Over the last years, there have been extensive studies of the anti-neoplastic activity and the clinical utility of the somatostatin analogues in different types of cancers. In acromegalic patients, treatment with somatostatin analogues can reduce the levels of GH and insulin-like factor (24). Furthermore, somatostatin analogues were shown to reduce pituitary tumor size by 30-80% (25,26). Expression of SSTRs mainly SSTR2 has been demonstrated in different types of lung cancer including typical carcinoids, atypical carcinoids, large cell neuroendocrine, and small cell lung cancer (27). In addition, an inverse correlation may exist between SSTR2 up-regulation and tumor aggressiveness (28). Although early experimental studies recognized a potential therapeutic role of SSTR2 analogues in small-cell lung cancer, so far clinical trials have not shown that treatment with SSTRs analogues improve patient survival (29, 30). In prostate cancer, Koutsilieris et al. showed that a combination of tripterolin, lanreotide and dexamethasone reduced prostatic specific antigen and improved performance status in patient with metastatic disease (31-37). Several other studies suggest that in prostate cancer somatostatin analogue although ineffective when given as monotherapy, might be beneficial when combined with androgen deprivation regimes (38, 39). SSTR subtypes are expressed in colon cancer (40) and Colucci et al. showed that somatostatin decrease COX 2 expression and function via activation of SST3 and SSTR5 receptors (41). In liver cancer, Kouroumalis et al. showed an increase in overall survival in patient treated with octreotide (42). On the other hand HECTOR which is a randomized double-blinded clinical study failed to demonstrate survival advantage in patients with inoperable hepatocellular carcinoma treated with octreotide (43). Despite not being effective as mono-therapy, somatostatin analogues can be used in combination with other treatment approaches to increase their efficacy without worsening toxicity.
In conclusion, our data provide, for the first time, evidence for the expression of SSTRs in normal and cancerous bladder tissue. Differential expression of the SSTRs raises the possibility that SSTRs might be related to proliferative activity and tumor differentiation. Further studies are required to elucidate the precise relevance of SSTR expression in bladder cancer tumorigenesis and progression and to evaluate the diagnostic and therapeutic implications of SSTRs in bladder cancer.
- Received February 15, 2014.
- Revision received April 1, 2014.
- Accepted April 2, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.