


Abstract
Breast cancer is one of the leading causes of death among women and the renin–angiotensin system (RAS) has been associated with breast tumor growth and metastasis. Inhibition of the RAS limits such effects and several efforts have been made to develop new inexpensive strategies for breast cancer treatment. We herein provide additional evidence that breast cancer chemotherapy can be influenced by losartan and PD123319, antagonists of angiotensin receptors AT1 and AT2, respectively. Perhaps the most important result was that this occurred without interfering with the expression or activity of the multidrug resistance-associated protein, ABCC1, which is associated with defensive cellular mechanisms. Moreover, they increased intracellular doxorubicin accumulation, which could increase cytotoxicity.
Breast cancer is one of the leading causes of death among women worldwide. The renin-angiotensin system (RAS) has been associated with local tumor growth, inflammation, angiogenesis and facilitation of metastasis (1). Some data suggested that drugs that inhibit RAS have the potential to limit such effects of angiotensin II (angiotensin) and in recent years, several efforts have been made to develop new inexpensive strategies of cancer treatment with the use of angiotensin-converting enzyme inhibitor (ACEi) or angiotensin receptor antagonists (ARAs) (2-8). However, it is still unclear if these anti-hypertensive drugs can potentiate or hamper cancer chemotherapy.
Although the studies above indicated that hormones could alter the response of breast cancer cells to chemotherapy, there are no conclusive studies regarding the interaction between such hormones and chemotherapeutics. Therefore, the aim of the present study was to evaluate the interaction between doxorubicin, one of the main chemotherapeutics used worldwide in breast cancer treatment, and the hormones related to hypertension: angiotensin II, aldosterone and vasopressin, in the MCF-7 breast cancer cell line. MCF-7 is a hormone-responsive cell line, like the majority of breast cancer cases. It has been shown that MCF-7 cells expresses several members of the RAS, such as angiotensinogen, prorenin, angiotensin II receptor 1 (AT1) and 2 (AT2) (9, 10); this cell line also expresses all vasopressin receptor subtypes (11).
Materials and Methods
Cells and culture conditions. The human breast adenocarcinoma cell line MCF-7 was kindly provided by Dr. Rachel Maia (National Institute of Cancer, Rio de Janeiro, Brazil), and it was grown in Dulbecco's modified Eagle's medium (DMEM) low glucose supplemented with 10% fetal bovine serum (FBS; GIBCO, Grand Island, NY, USA), in disposable plastic bottles at 37°C. Cells were sub-cultured using Trypsin 0.05% in 0.53 mM EDTA (GIBCO) every 3-4 days. All experiments were performed 24 h after seeding in DMEM 10% FBS to ensure uniform attachment of the cells at the onset of the experiments.
Trypan blue assay. Cells were seeded in 24 microwell plates (TPP, Biosystem, Curitiba, Brazil) at a density of 1×104 cells/ml (1 ml/well). After 24 h the cells were treated with vasopressin, aldosterone, angiotensin, or combinations of 1 nM angiotensin, 1 nM losartan (an antagonist of AT1) or 1 mM PD123319 (an antagonist of AT2) with/without 500 nM doxorubicin for up to 72 h in DMEM without serum. After incubation, the supernatant was collected, transferred to microtubes and centrifuged in a clinical centrifuge (650 × g, 6 min). The remaining cells in the wells were detached with 200 μl of trypsin-EDTA and mixed to the corresponding pellet collected from the supernatant. Total cells were stained with a 0.4% Trypan Blue solution and counted in a Neubauer counting chamber. Each experiment was repeated at least three times (manual counting) and was also performed using a Beckman Coulter Vi-Cell automated cell viability analyzer.

Effect of vasopressin (ADH) and aldosterone (ALDO) on MCF-7 cell growth. The cells were incubated for 48 or 72 h with different concentrations of each hormone and cell viability was measured by Trypan blue assay.
Measurement of intracellular accumulation with doxorubicin. Cells were seeded on 24-microwell plates (TPP, Biosystem, Curitiba, Brazil) at a density of 5×105 cells/ml (1μl per well) in DMEM 10% FBS for 24 h. Cells were then treated with 500 nM doxorubicin in the presence or absence of 1nM angiotensin with/without losartan for 24 h in DMEM without serum at 37°C. After incubation, cells were harvested with Trypsin-EDTA, transferred to microtubes and the fluorescence of intracellular doxorubicin was measured in the FL3 channel in a BD FACSCalibur flow cytometer (BD Biosciences, São Paulo, SP, Brazil).
Optical and fluorescence microscopy. Cells were seeded on 24-microwell plates (TPP) with (for fluorescence) or without (for phase-contrast microscopy) round glass coverslips deposited at the bottom of the wells, at a density of 1×105 cells/ml (1 ml per well) and treated as described above. For optical phase-contrast microscopy, the photographs were directly taken from the wells. For fluorescence, the coverslips were layered on glass slides before taking the pictures. Photographs were taken with a Zeiss Color AxioCam attached to a Zeiss Axiovert 100 microscope, using a ×40 non-oil PhI Zeiss Acrophot objective (all from Carl Zeiss, São Paulo, SP, Brazil).
Multidrug resistance associated protein (ABCC1) expression and activity. For measurement of ABCC1 expression, cells were seeded onto 24-well plates and the labeling assay was performed as described in previous work by our group (12, 13). Polyclonal rabbit antibody A23 (Alexis Biochemicals, San Diego, California, USA) and Alexa Fluor 488 (Biosystem, Curitiba, Brazil) were used as primary and fluorescent secondary antibodies, respectively. For evaluation ABCC1 activity, the procedure is also described in (13). Briefly, cells were cultured as explained above and then incubated with carboxyfluorescein diacetate N-succinimidyl ester (CFDA) (1 μg/ml, 105 cells/well, for 30 min) in DMEM without serum.
After loading, the medium was replaced and cells were treated with or without transporter inhibitor MK571 (Biosystem, Curitiba, Brazil) (25 μg/ml) to allow efflux of carboxyfluorescein (CF). The transporter activity was evaluated as the difference between intracellular fluorescence intensity with and without the inhibitor, measured in a BD-FACS Calibur flow cytometer.
Statistical analysis. Each experiment was repeated from three to seven times. Data are expressed as means±standard error of the mean (SEM) and were analyzed by paired one-tailed t-test or one-way analysis of variance with Dunnett post test. Values of p<0.05 were considered statistically significant.
Results
Aldosterone and vasopressin did not alter cellular growth (Figure 1) and did not alter doxorubicin sensitivity (data not shown). On the other hand, angiotensin increased the growth of MCF-7 cells, as expected, and the proliferative effects were seen when MCF-7 cells were treated with 1 and 0.01 nM of angiotensin for 72 h (data not shown). Therefore, 1 nM angiotensin was used to investigate the effects of the AT1 and AT2 antagonists losartan and PD123319, respectively, on cell proliferation. Figure 2 shows that both losartan and PD123319 blocked the proliferative effect of angiotensin on MCF-7 cells. Moreover, neither losartan nor PD123319 alone-altered cell growth.

Effect of angiotensin (ANG), losartan (LOS) and PD123319 (PD) on MCF-7 cell viability. The cells were incubated for 72 h with the drugs alone and in combination, and the cell viability was measured by the Trypan blue assay. *Statistically diferent from the control (CTR) at p<0.05.
The next step was to study whether angiotensin, losartan, PD123319 and their combination could alter the toxicity of doxorubicin, widely used in breast cancer chemotherapy. Figure 3 shows that angiotensin, whether alone or in the presence of losartan or PD123319, was not capable of altering the toxicity of doxorubicin. Neither losartan, PD123319, vasopressin nor aldosterone modified doxorubicin toxicity (data not shown).
Although doxorubicin toxicity remained unaltered by the treatments, we observed an increase in intracellular accumulation of doxorubicin in some cells, as seen in Figure 4, in both nuclei and cytoplasm, when cells were treated for 24 h with doxorubicin in the presence of angiotensin with losartan. Since doxorubicin is transported by ABCC1 (14) and we observed that MCF-7 cells express this protein (data not shown), we evaluated whether treatment with angiotensin-plus-losartan altered the expression or activity of this protein.
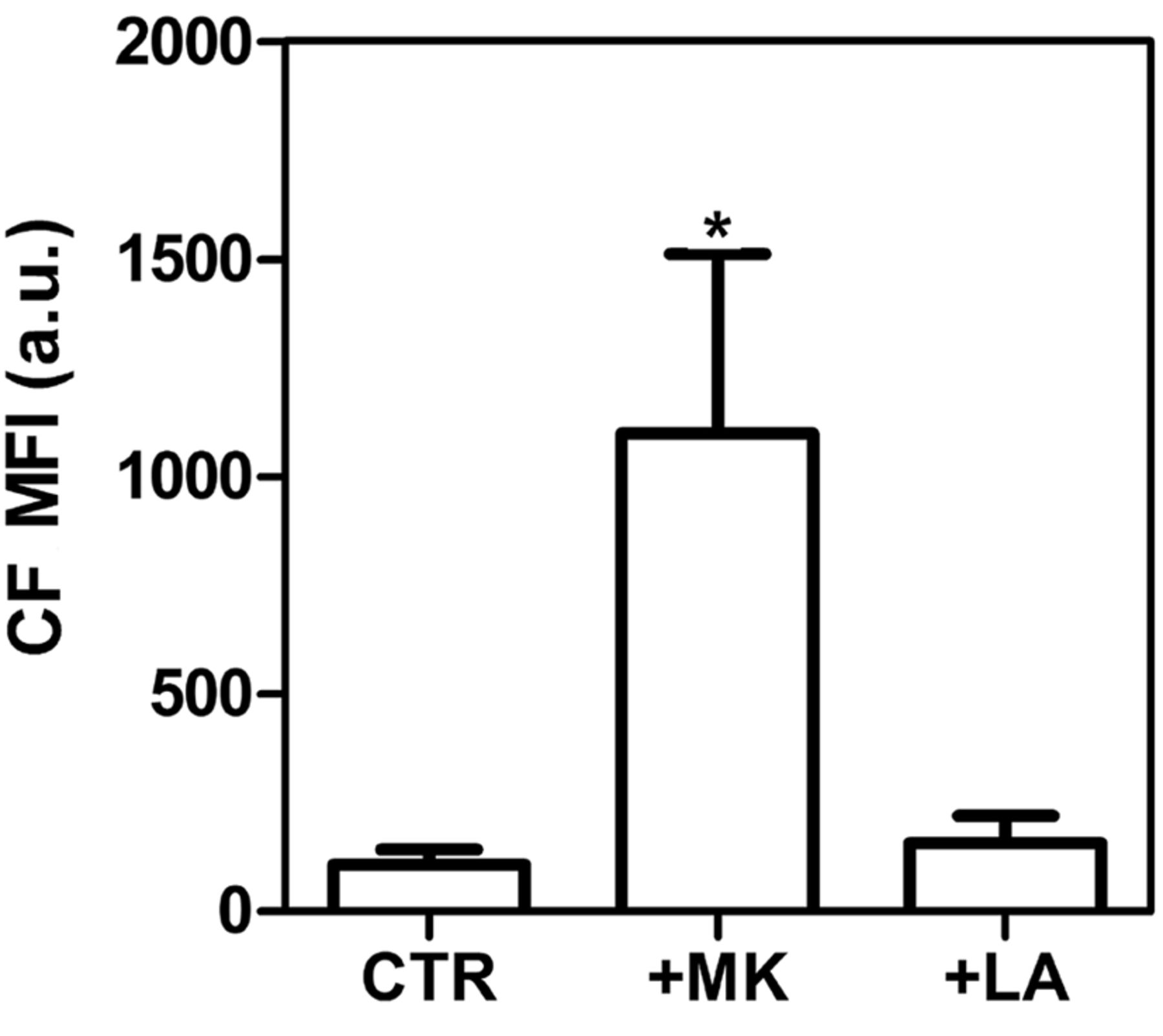
ABCC1 expression was evaluated by flow cytometry after treatment of cells for 24 h with angiotensin with/without losartan in DMEM without FBS. It was observed that the expression of the transporter remained the same (Figure 5). Moreover, the activity of the transporter was not altered by angiotensin with losartan (Figure 6).
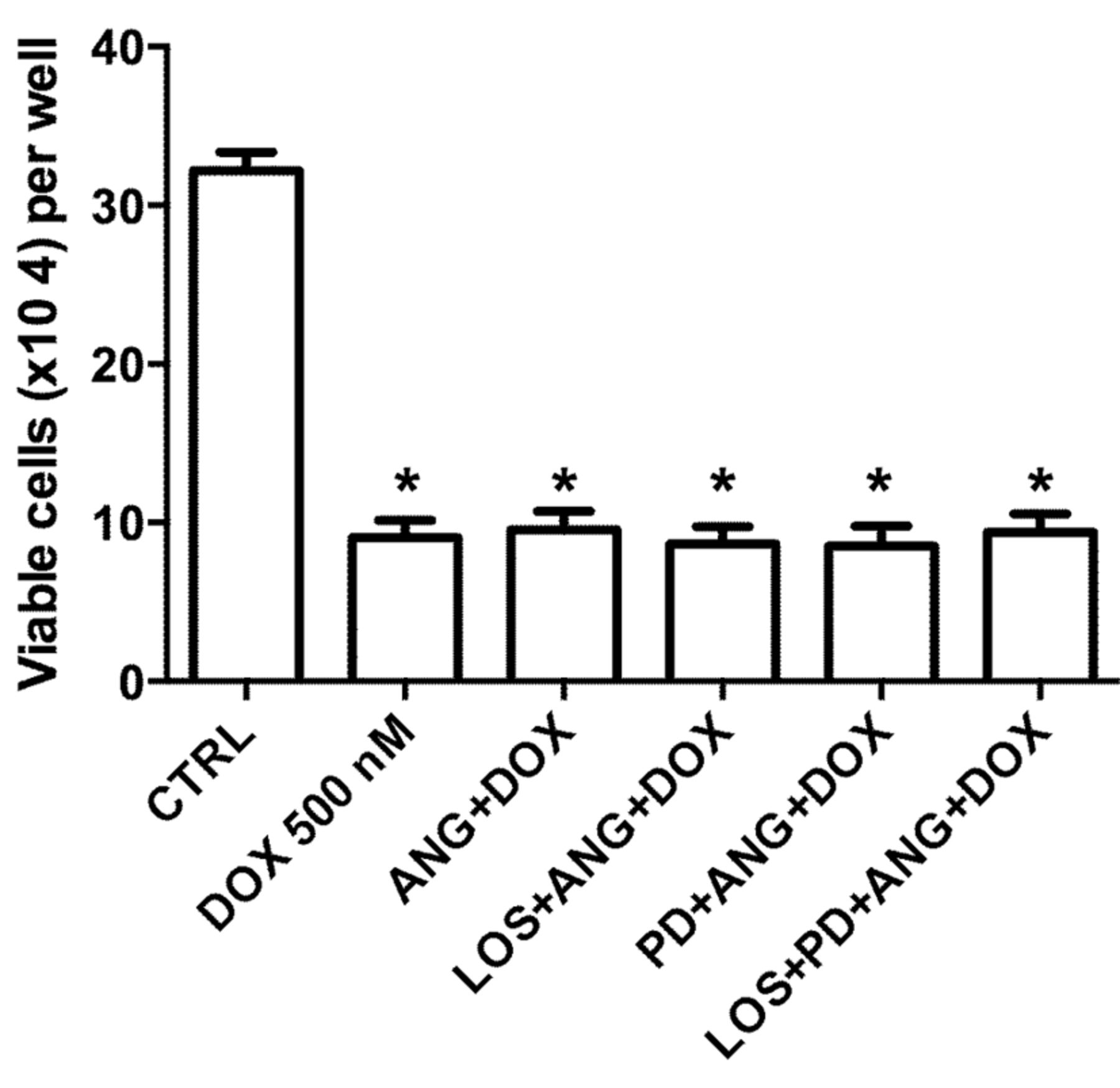
Effect of angiotensin (ANG), losartan (LOS) and PD123319 (PD) in MCF-7 cell sensitivity to doxorubicin (DOX). The cells were incubated for 72 h with the drugs alone and in combination, and after 72 h, the cell viability was measured by Trypan blue assay. *Statistically diferent from the control (CTR) at p<0.05.
Discussion
In the present study, we provide additional evidence that breast cancer chemotherapy can be influenced by anti-hypertensive treatment, herein represented by its main mediator, angiotensin, and the AT1 and AT2 antagonists, losartan and PD123319. No effect was observed with vasopressin nor with aldosterone (data not shown).
Perhaps the most important result was that this occurred without interfering with the expression or activity of ABCC1, which is associated with defensive cellular mechanisms. Studies have shown that normal and cancerous breast cells express several elements of RAS, such as angiotensinogen, prorenin, angiotensin-converting enzyme and angiotensin receptors (6, 7, 15), which is enough to consider the breast as a site at which the RAS might contribute directly or indirectly to the proliferation of breast tumor itself (3, 5, 7, 16).
The first studies investigating the effects of angiotensin in breast cancer cells identified that this hormone reduced the expression of integrin β1, suggesting that it might contribute to the progression of metastasis (8); however, integrin expression failed to be identified as an independent short-term indicator of prognosis, progression and metastasis in humans (17). Even though the contribution of RAS to cancer progression and metastasis is still unclear, increasing evidence is emerging in the literature suggesting that treatment for hypertension might contribute to efficacy of breast cancer chemotherapy. Angiotensin is a pro-inflammatory mediator which seems to act as a driving force for atherogenesis and vascular dysfunction (18, 19). Atherogenesis, thrombosis and vascular disease are associated conditions (18, 20). Several studies suggest that angiotensin, through activation of AT1, might activate the sodium potassium pump, producing reactive oxygen species, stimulating secretion of leukotriene C4, via ABCC1 (18-23). This, in turn, could trigger the proliferation of breast cancer cells. However, other researchers believe that proliferation induced by angiotensin is directly promoted by AT1 via phosphatidylinositide 3-kinase (PI3K), activation of protein kinase B (PKB or AKT), up-regulating cyclin-D1 and glycogen synthase kinase 3 beta (GSK-3B), and down-regulating p27, and all events were prevented by treatment with losartan (24).
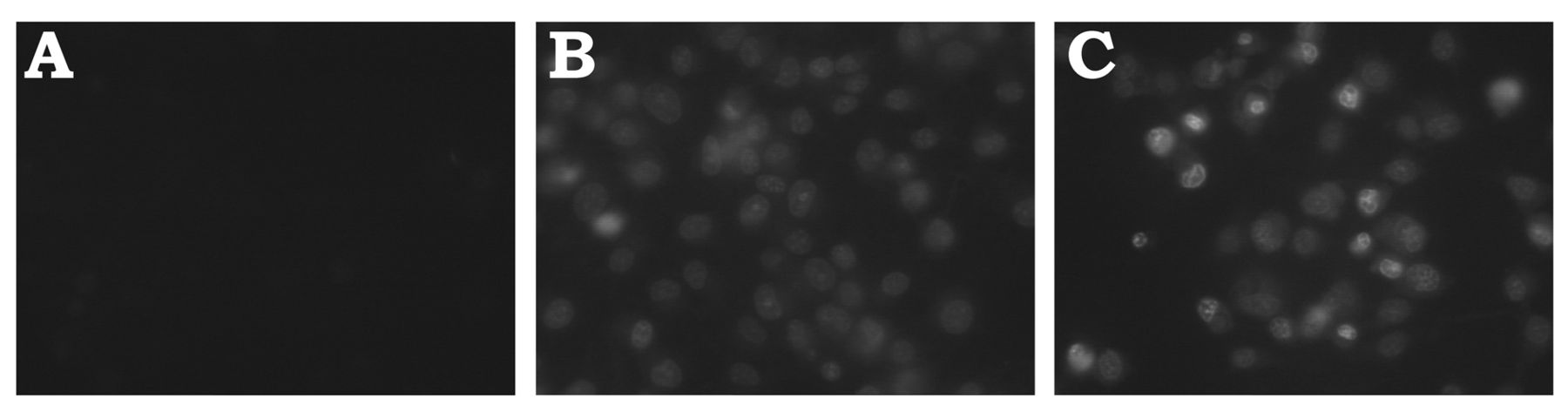
Cellular uptake of doxorubicin. Autofluorescence is shown in (A). The cells were incubated for 24 h with doxorubicin in the absence (B) or presence (C) of angiotensin.
There is evidence that angiotensin per se might prevent or diminish the efficacy of doxorubicin anti-tumoral effects via activation of PI3/AKT signaling and suppression of caspase-9 in human breast cancer cells (26). Although we did not observe an increase in resistance to doxorubicin in cells treated with angiotensin, our data showing that AT1 and AT2 antagonists abrogated the mitogenic action of angiotensin support the potential benefits of these drugs in breast cancer chemotherapy.
The overexpression of AT1 is found in breast hyperplasia, although it does not correlate with malignancy (26, 27), which may be due to other RAS components. It has been shown that activation of AT1 by angiotensin in MCF-7 cells leads to cell proliferation (16) and increases integrin β1 expression, which has been associated with inhibition of angiogenesis, proliferation (3, 7) and metastasis (8). Some studies favored the use of ARA instead of ACEi because pro-angiogenic effects, possibly due to bradykinin, have been observed (4, 28). In mice, ARAs have been implicated in the inhibition of angiogenesis and metastasis, and therefore would have a positive effect on chemotherapy (7, 29-34). In humans, ACEi was associated with an anti-angiogenic effect during treatment of hepatocellular carcinoma with 5-fluorouracil (35). The major mechanism by which the RAS exerts its effect seems to be its angiogenic effect, although angiotensin II has also been shown to be a growth factor (4, 16). It has been recently proposed that angiotensin would have a protective, but undesirable, effect on cytotoxicity induced by doxorubicin (25).

Expression of multidrug resistance-associated protein (ABCC1) in MCF-7 cells treated with losartan and angiotensin (LOS+ANG). After 24 h of incubation with LOS+ANG, the cells were fixed and labelled with ABCC1 antibody. The cellular fluorescence was measured by flow cytometry. A: Representative histogram of cells labeled with ABCC1 antibody. B: Number of cells positively staining for ABCC1. CTR, Control cells.

Activity of multidrug resistance-associated protein (ABCC1) in MCF-7 cells treated with losartan and angiotensin (LA). After 24 h treatment with LA, the cells were incubated with carboxyfluorescein diacetate N-succinimidyl ester for 30 min. After washing, the mean fluorescence intensity (MFI) was measured by flow cytometry. For comparison, non-treated cells were incubated with the ABCC1 inhibitor MK571 (MK).
Recently, telmisartan and candesartan-cilexetil, both antagonists of AT1 used to treat angiotensin-dependent hypertension have been identified as ABC transporter modulators (36). However, these studies only evaluated mRNA and activity of P-glycoprotein (P-gp), breast cancer resistance protein (BCRP) and multidrug resistance associated protein-2 (MRP2), and the authors did not evaluate the expression or activity of these transporters.
It has been found that 10-20% of estrogen receptor-positive breast carcinomas markedly overexpress AT1 (37). These patients are losartan-sensitive and represent an interesting sub-population of patients receiving ARAs adjuvant treatment (37). Our study corroborates the use of ARAs, suggesting that they are not toxic and do not alter ABCC1 action. Moreover, they seem to increase intracellular doxorubicin accumulation, which could lead to a long-term effect on cytotoxicity. However, there is possibility that such an increase might cause doxorubicin cardiotoxicity. Therefore, more studies are necessary in order to test this hypothesis.
Acknowledgements
Technical support was provided by Mr. Shanserley Leite do Espírito Santo (FAPERJ TCT-4 Fellowship).
- Received November 5, 2013.
- Revision received December 7, 2013.
- Accepted December 10, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}