


Abstract
Aim: Imatinib mesylate (IM) has substantial efficacy in patients with metastatic gastrointestinal stromal tumors (GISTs), and pathological complete response (pCR) following IM treatment has been sporadically reported; however, its clinical significance for GIST needs to be clarified. Patients and Methods: From 2001 to 2010, 26 out of 171 patients with metastatic GIST who received IM with response or stable disease underwent operation. Among them, 12 operations with pCR were compared to 14 operations without pCR regarding clinicopathological features, mutation status, progression-free survival (PFS), and overall survival (OS). Following the operation, each tumor was assessed immunohistologically, and genetic analysis was performed on the tumor tissue. Results: Twelve out of 26 (46.2%) patients with metastatic GIST who received IM with response or stable disease had pCR. After a median follow-up of 40.8 months, patients with pCR had significantly better PFS and OS than those without pCR [2-year PFS and OS: 82.5% and 100% versus 35.6% and 49.4%, (p=0.014 and p=0.004) respectively]. Predictive factors for pCR were: origin of GIST, response after IM therapy, and duration of IM use before operation. Patients without pCR had a significantly higher frequency of secondary mutation when compared to those with pCR (47.4% versus 0%; p=0.004). Conclusion: Patients with colorectal GIST receiving IM who responded more quickly to IM treatment prior to surgery had a higher chance of pCR. pCR results in significantly favorable PFS and OS, however, IM cannot be withdrawn. Patients without pCR had a significantly higher frequency of secondary mutation when compared to those with pCR.
Gastrointestinal stromal tumor (GIST) is the most common mesenchymal tumor of the gastrointestinal tract. Patients with primary localized GIST who undergo radical resection often develop tumor recurrence, especially high-risk patients (1-3). In 1998, Hirota et al. identified gain-of function mutations in the KIT proto-oncogene encoding cluster of differentiation 117 (CD117) in GIST (4). Subsequent reports demonstrated that KIT mutations are responsible for up to 85% of GISTs, while another 3% to 5% have a mutation in platelet-derived growth factor receptor (PDGFR) (5-8). Imatinib mesylate (IM) inhibits KIT and PDGFR tyrosine kinases and was successfully used to treat GIST in 2001 (9). IM achieves a partial response or stable disease in almost 80% of patients in the West and in Taiwan, and the 2-year overall survival rate in advanced GIST is now 75% to 80% (6, 9, 10). However, patients with GIST eventually develop resistance and face disease progression at 2 years or more (10, 11). The major mechanisms of this acquired resistance to IM in GIST have been reported in several studies (12-15).
To improve the outcome of patients with GIST who have begun to show disease progression following targeted-therapy, a multimodality approach, i.e. a salvage therapy [including increased IM doses (16), alternative tyrosine kinase inhibitors (17), or surgery (18)] should be considered. We have demonstrated that surgery can have an adjuvant role in combination with IM treatment to extend the time which patients can remain on the drug (18). Operation may also have a role in selected patients with GIST with partial response, stable disease, and locally progressing disease (18). Pathological complete response (pCR) after surgery highlighting the therapeutic efficacy of IM has been reported (19). pCR has also been reported in breast (20), colon (21), and esophageal cancer (22), however, its clinical impact on GIST needs to be clarified. The aim of our study was to determine the incidence of pCR in patients with GIST receiving IM with response or stable disease and to clarify its impact on long-term survival rates.
Patients and Methods
From 2001 to 2010, 171 patients with metastatic GIST received IM treatment. Among them, we performed 26 operations on 26 patients with metastatic GIST who were being treated with IM with response or stable disease. Pathological diagnosis for GIST was confirmed using standard hematoxylin/eosin staining and CD117 immunohistochemistry on formalin-fixed, paraffin-embedded tissues. Patient data were prospectively collected and the study was approved by the local Institutional Review Board of Chang Gung Memorial Hospital, Taipei, Taiwan (IRB number: 101-4847B). Written informed consent for drug administration and analysis of tumor-associated genetic alteration was obtained from each patient.
Preoperative management. The response to targeted-therapy was evaluated every 3 to 6 months after treatment by computed tomography (CT) according to the Response Evaluation Criteria in Solid Tumors criteria (RECIST) (23). Clinical complete response (CCR) was defined as the absence of any lesion or residual cystic degeneration at the site of the initially detected metastases on all imaging modalities. Preoperative imaging was reviewed by a radiologist (J. H. Tseng) for all patients with GIST.
Conduct of operation. All procedures were performed at the Department of Surgery, Chang Gung Memorial Hospital, Taoyuan, Taiwan. All patients discontinued the use of IM the day before elective operation (the optimal interval for being off-drug was still unknown). The primary goal of surgery was to remove all sites of disease in patients with response or stable disease while sparing function to the greatest extent possible. Progression-free survival (PFS) was defined as the length of time from the date of operation to the date of documented progression of residual disease, recurrent disease, or to death from any cause, whichever occurred first. Overall survival (OS) was defined as the length of time from the date of operation to death from any cause. Surgical mortality was defined as death within one month after operation.
Tumor samples and immunohistochemstry (IHC) for CD117 and vimentin in GIST. Formalin-fixed paraffin-embedded tissue sections were processed for IHC. A 4-μm section of each specimen was stained for CD117 and vimentin. IHC was performed on a Bond Max autostainer (Leica Microsystems, Bannockburn, IL, USA) according to the manufacturer's protocol. Briefly, slides were dewaxed in Bond Dewax solution and re-hydrated in Bond Wash solution (Leica Microsystems). For vimentin, antigen retrieval was performed at pH 6 using Epitope Retrieval 1 solution (Leica Microsystems) for 20 min at 100°C. For CD 117, antigen retrieval was performed at pH 6 using Epitope Retrieval 2 solution (Leica Microsystems) for 20 min at 100°C. Slides were then incubated for 15 min at room temperature with primary antibodies against CD117 (C-KIT) (A4502; Dako, Carpinteria, CA, USA) and Vimentin (M0725; Dako) at dilutions of 1:500 and 1:75, respectively. Antibody detection was performed using the biotin-free Bond Polymer Alkaline Phosphatase Red and Refined systems (Leica Microsystems). Slides were then counterstained with hematoxylin. The slides were mounted and blindly analyzed under a microscope and labeling of GIST was scored as either negative or positive immunostaining for the relevant antigens. At a microscopic level, pCR was defined as tumor cells with myxoid degeneration and without CD117 expression in the surgical specimen as previously described (19).
Demographic data and procedures for 26 surgeries for metastatic GIST.
Analysis of KIT and PDGFRA mutations. Tissue samples from the 26 tumors were assessed for genetic mutations before and after surgery. Formalin-fixed, paraffin-embedded tissue specimens were trimmed to enrich for tumor cells. Polymerase chain reaction amplification of genomic DNA for KIT and PDGFRA was performed and amplification was analyzed for mutations as previously described (24).
Clinicopathological features of 26 patients with GIST undergoing surgery after imatinib mesylate treatment, comparing between those with (Group A) and those without pathological complete response (Group B).
Follow-up. Patients were assessed at 1 month postoperatively and then every 3 to 6 months with abdominal CT, clinical examination and laboratory testing.
Statistical analysis. All data are presented as the percentage of patients or the mean with standard deviation. All numerical continuous data were compared by Mann-Whitney U-test. Categorical data were compared by Pearson's Chi-square test or Fisher's exact test and multiple forward stepwise logistic regression analysis when appropriate. The survival rates were calculated with the Kaplan–Meier method. The survival analysis was performed by the log-rank test. SPSS for Windows (SPSS version 13.0; SPSS, Chicago, IL, USA) was used for the statistical analysis. p<0.05 was considered to be statistically significant.
Results
Demographic data. Table I presents a summary of the clinicopathological features. There were 8 male and 18 female patients, with a median age of 58.5 years (range=42-76 years). We performed 26 operations on 26 patients with metastatic GIST who were being treated with IM with response or stable disease (Table I). The small bowel was the most common site of origin of GIST (11/26), followed by the stomach (9/26), and then the colon and rectum. Patients received IM treatment for a median of 12.5 months before surgery. At the time of operation, all patients were being treated with IM at 400-800 mg/day and no patient had been switched to sunitinib. The median sum of the size of five measurable tumors in these 26 patients was 11.0 cm However, after the operation, 17 patients maintained IM at 400 mg per day, seven were being treated with IM at 600-800 mg/day, and two had been switched to sunitinib (Table I).
Exon 11 of KIT gene is the site where mutations were most commonly found to occur in the 26 tumor specimens tested (76.3%), followed by exon 9 (16.9%).
Predictive factors for pCR after surgery. A total of 26 out of 171 patients with GIST who received IM with response or stable disease underwent 26 operations. Twelve (7%) patients presented with pCR; the remaining 14 patients formed the comparison group for this study. Among the 12 patients with pCR, there were seven men and five women with a median age of 57.0 years (range=46-76 years). The median measurable tumor size was 9.6 cm (range=3.7-42.8 cm) at diagnosis. For patients without pCR, the median measurable tumor size was 14.5 cm (range=1.6-57.6 cm) at diagnosis (Table II).
Compared to patients who did not show pCR, patients with colorectal GIST receiving IM with response at a shorter duration of IM use before surgery had a higher chance of pCR (Table II).
With regard to the laboratory data, patients with GIST who had pCR were not significantly different from those who did not have pCR.
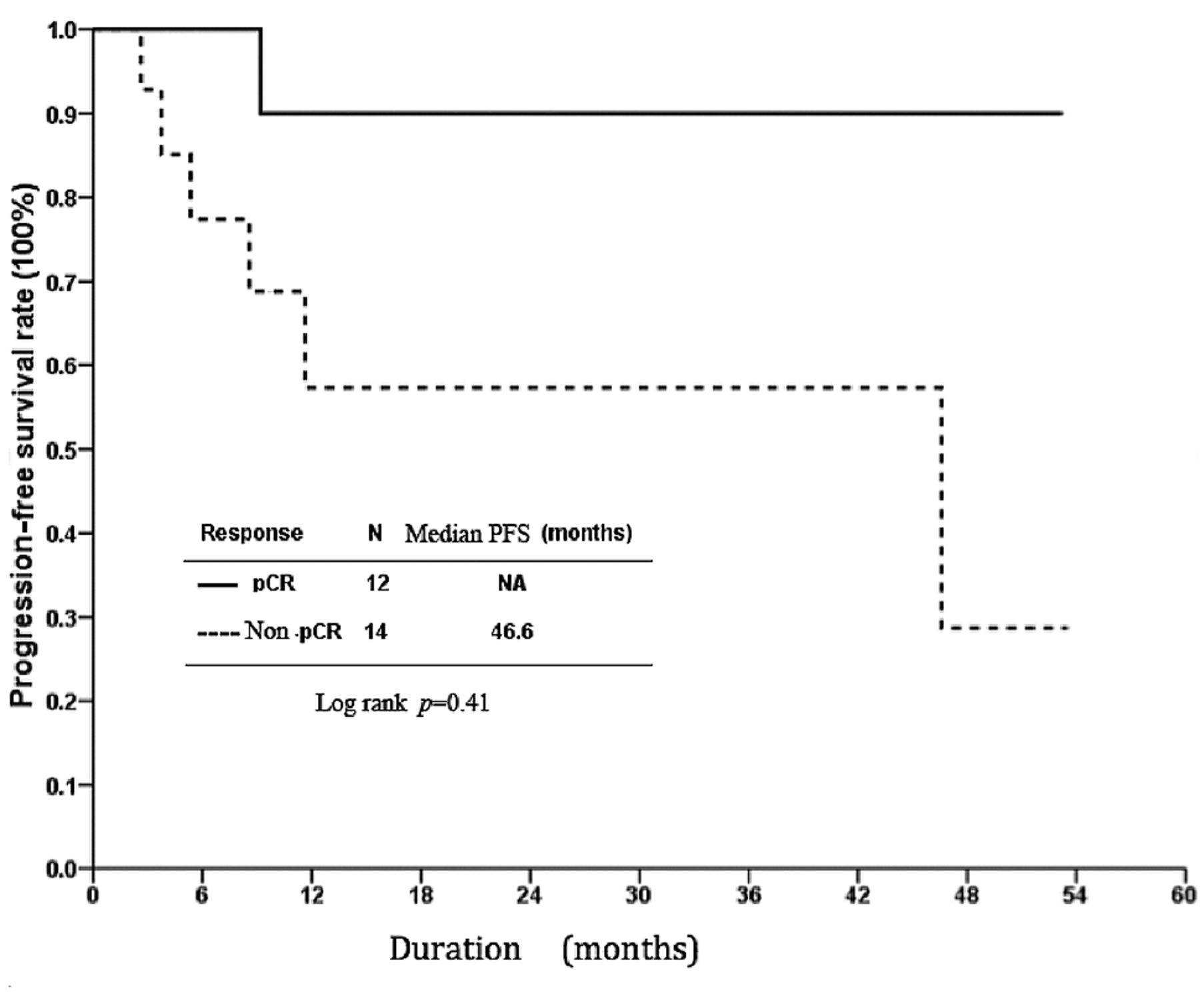
Surgical outcomes. No surgical mortality was noted in this study. The median follow-up time for these 26 patients was 40.8 months (range=8.1-93.3 months). Patients with pCR had superior 2-year PFS and OS, although statistical significance was not achieved (Figures 1 and 2). The 2-year PFS and OS was 82.5% and 100% for patients with pCR compared to 35.6% and 49.4% for patients without (p=0.041 and 0.177, respectively).

Progression-free survival (PFS) rate for 56 Taiwanese patients with advanced gastrointestinal stromal tumors treated with imatinib and surgery in terms of pathological complete response (pCR) versus non-pathological complete response.
Nearly all the operations were performed on an elective basis. Resection of peritoneal tumor (17/59; 26.3%) comprised the most common surgical procedure, followed by hepatic resection (13/59; 18.4%) to remove all tumors (Table I). One patient with systemic progression underwent tumor debulking to control tumor hemorrhage induced by a response to IM. There were no perioperative deaths. However, eight patients suffered operative morbidities, including four wound infections, two pleural effusions, one case of upper gastrointestinal bleeding, and one of pneumonia.
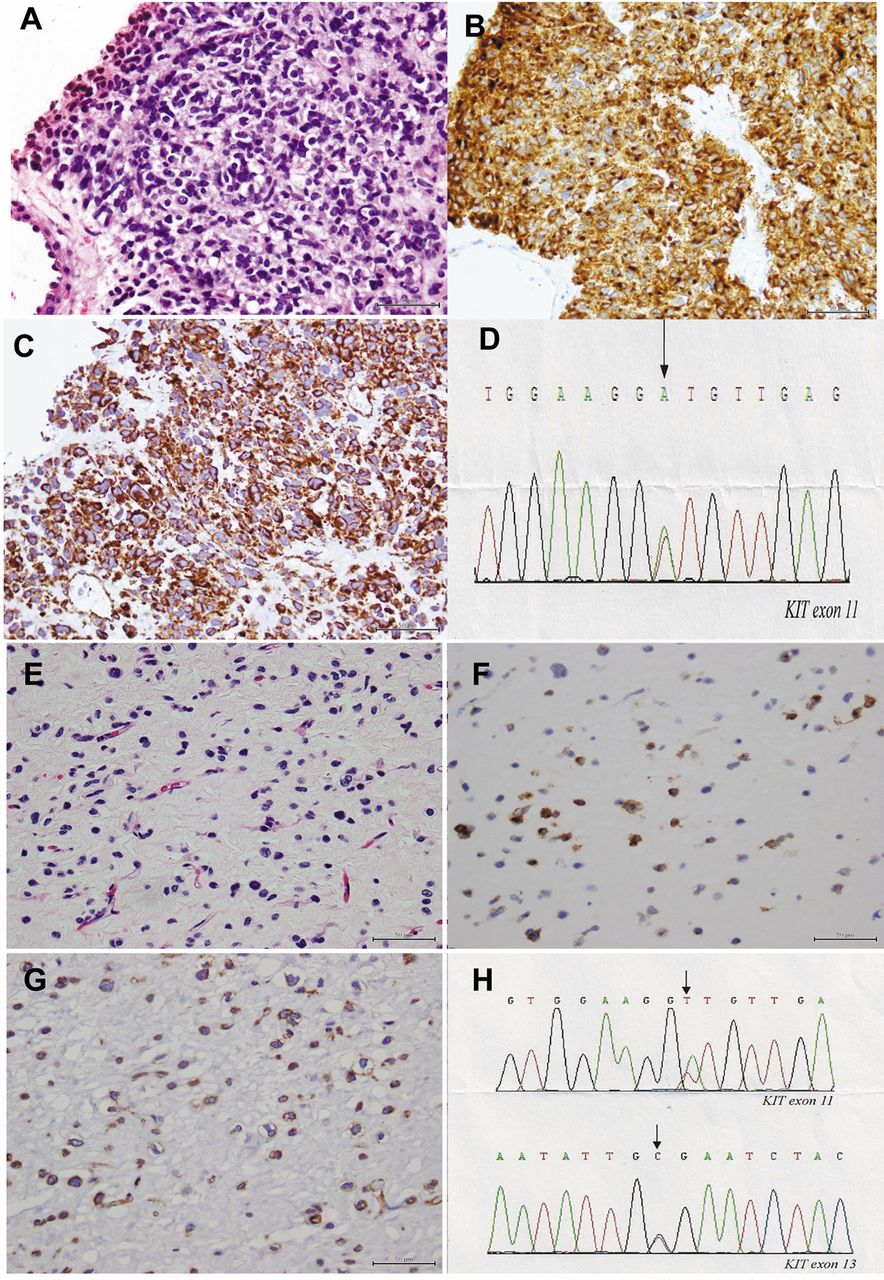
Immunohistochemical study with CD117 and vimentin. Figure 3A shows a histopathological representation of a patients with GIST with typical CD117-positive spindle tumor cells before IM treatment (Figure 3B). Further IHC study revealed positive vimentin immunostaining in the spindle tumor cells (Figure 3C). The patient underwent surgery for the responsive lesion after IM treatment and subsequent histopathological study revealed no viable tumor cells with myxoid degenerative changes (Figure 3E). Further immunohistochemical study revealed negative CD117 immunostaining, supporting the diagnosis of pCR; however, staining for vimentin was positive for the spindle tumor cells (Figure 3F and G). Figure 4A shows the histopathological analysis of another representative patient with typical CD 117- and vimentin-positive spindle tumor cells before IM treatment (Figure 4B and C). The patient underwent surgery for the responsive lesion after IM treatment and subsequent histopathological study revealed viable CD117- and vimentin-positive tumor cells (Figure 4E and F), supporting the diagnosis of non-pCR.

Overall survival (OS) rate for 56 Taiwanese patients with advanced gastrointestinal stromal tumors treated with imatinib and surgery in terms of pathological complete (pCR) response versus non-pathological complete response.
Subsequent genetic changes in terms of response and genetic background. Tissue specimens from before and after the operation were available for 49 out of the 59 resected GISTs (83.1%). No PDGFRA mutations were found in this study. None of the 11 patients (0%) with pCR tested for genetic changes were found to have a secondary mutation after surgery (Table III). However, 18 out of 38 patients without pCR tested positively for secondary genetic mutations (47.4%) after the operation (Figure 3H and 4H). Thus, patients without pCR had a significantly higher frequency of secondary mutation when compared to those with pCR (47.4% versus 0%; p=0.004). Two out of the 9 patients with primary mutations in exon 9 of KIT had de novo mutations discovered after surgery (found in exon 17, 2/9; 22.2%). However, 16 out of 39 patients with KIT exon-11 mutations (41.0%) were found to have a secondary mutation after surgery. Of the secondary mutations, 81.3% (13/16) were found to be in exon 17, and exon 13 comprised the remaining 18.7% (3/16). Patients with exon-11 mutations of KIT tended to have a higher frequency of secondary mutation, but this was not statistically significant (41.0% versus 22.2%; p=0.451).
Discussion
Since 2001, IM has been demonstrated to have substantial efficacy in most patients with metastatic GISTs. As far as we are aware, this is the first reported study investigating the clinical impact of pCR on a Taiwanese population of patients with metastatic GIST. Several issues of interest have emerged during this study.
Genetic changes in KIT for 26 tissue samples from patients with advanced inoperable/metastatic GIST during imatinib mesylate (IM) treatment in terms of complete pathological response.
Firstly, pCR was observed in 7% of 171 patients with metastatic GIST treated with IM. Additionally, patients with colorectal GIST who received IM with response at a shorter duration of IM use before operation had a higher chance of pCR.
Secondly, similar to reports of pCR for breast, colonic, and esophageal cancer, pCR does have a clinical impact on patients with GIST who received IM. Patients with metastatic GIST with pCR after operation had superior PFS and OS than those without pCR. Similar to Rau et al., Rutkowski et al., and Andtbacka et al.'s reports, we found that the chance of reaching the goal of surgery by reducing the tumor burden in pCR is significantly high to cure selected patients (25-27). Such achievements may not only prolong the time to progression but may also potentially cure the disease, as demonstrated by longer PFS and OS when compared with those patients who did not have pCR.
Thirdly, while consensus on this issue has not been reached, the continued use of IM for patients with GIST with pCR is recommended based on this study. Histopathological examination demonstrated tumor cells with myxoid degeneration and a loss of CD117 expression after pCR (19), mimicking the absence of viable tumor cells after IM treatment. However, the suppression of downstream signaling pathways of the KIT gene was not an indication that the cancer cells were dead. Frequent vimentin expression in stromal tumor cells was still evident in the tissues assessed in this study, indicating that the cancer cells remained viable (19). The above observation supports the findings of two French clinical trials investigating cessation of IM after response; they showed that IM interruption is associated with a high risk of relapse, even for patients with CR (28-19). Mearadji et al. also reported that a decrease in CD117 expression may be a prognostic factor for outcome in patients undergoing resection after neoadjuvant IM. (30). Thus, IM should not be discontinued in patients with GIST until the onset of IM intolerance or until the patient refuses such therapy.
Finally, the secondary mutation rate for patients with pCR was lower than that for patients without pCR, although not to a statistically significant level (0% versus 21.4%; p=0.004). Therefore, surgery for selected responsive lesions may play a role in preventing potential development of secondary mutations, which is the main cause of the development of resistance and eventual disease progression. As such, surgery might be viewed as having an adjuvant role to IM treatment (18, 23, 31). However, a prospective randomized study aimed at understanding whether surgery can prolong the duration of IM activity is still needed for responding patients. Secondary KIT mutations were also found to occur more frequently in patients with a primary exon 11 mutation than in those with primary exon 9 mutations [41.0% (3/26) versus 0% (0/2); p=0.451], although this difference was not significant. The mechanism underlying the lower frequency of secondary mutations in exon 9 is still unknown. Similarly to Antonescu et al.'s report describing molecular analysis of KIT and PDGFRA mutations in a cohort of patients who were treated with IM and then underwent surgical resection (12), secondary KIT mutation seems to be a common factor in acquired resistance to IM. The incidence of mutation in the first (exons 13 or 14) or second (exon 17) KIT kinase domain in untreated GIST is about 1% (32, 33). Another similarity to Antonescu et al.'s report was that in our study, we found that the most common site for secondary mutations was in exon 17 of the KIT gene [81.3% (13/16)], followed by exon 13 [18.7% (3/16)]. The long duration of imatinib therapy (median=15.6 months) in patients with acquired resistance who developed a secondary exon 17 mutation makes it less likely that a pre-existing clone is responsible for the acquired resistance (12). This is in contrast to patients with chronic myeloid leukemia with primary resistance, whose tissue samples have breakpoint cluster region-Abelson (BCR–ABL) kinase domain mutations. In these patients, the relapse in the blast-phase occurs within 1-3 months, and the identification of multiple mutations in patients with resistance is suggestive of clonal selection of pre-existing mutations that confer IM resistance.
However, many limitations do exist in our study. Firstly, the number of patients was limited. Moreover, in this study, no patient treated with sunitinib underwent surgery, hence we do not know the impact of pCR on patients with GIST receiving sunitinib. Secondly, this was a retrospective study and the patients underwent a selective screening process prior to undergoing any operation and being admitted into the study, thus, it was not a random population.
In summary, pCR was observed in 7% of 171 patients with metastatic GIST treated with IM. Patients with colorectal GIST who received imatinib with response at a shorter duration of IM use before operation had a higher chance of achieving pCR. Patients in whom pCR was observed had superior PFS and OS; however, IM cannot be withdrawn due to the tumor cells still being viable. Patients without pCR had a significantly higher frequency of secondary mutations when compared with those with pCR. Secondary KIT mutations were more frequently associated with a primary mutation in exon 11 than with a primary mutation in exon 9.

Immunohistopathological and molecular study of a patient with gastrointestinal stromal tumor with pathological complete response. Before imatinib treatment: A: Histopathological analysis showed the presence of typical spindle tumor cells B: Immunohistochemical study revealed positive immunostaining for cluster of differentiation 117 (CD117) (magnification×400). C: Immunohistochemical study revealed positive immunostaining for vimentin (×400). D: Direct sequencing analysis of DNA from patient no. 1 showed a deletion mutation at codons 550-558 in exon 11 (arrow) of KIT. After imatinib treatment: E: Histopathological study showed tumor cells with myxoid degenerative changes (HE, magnification×600). F: Immunohistochemical study revealed negative immunostaining for CD117 (magnification×600). G: Immunohistochemical study revealed positive immunostaining for vimentin (magnification×600). H: Direct sequencing analysis of DNA from patient no. 1 with pathological complete response showed a deletion mutation at codons 550-558 in exon 11 of KIT (arrow).

Immunohistopathological and molecular study of a patient with gastrointestinal stromal tumor without pathological complete response. Before imatinib treatment: A: Histopathological study showed the presence of typical spindle tumor cells (magnification×400). B: Immunohistochemical study revealed positive immunostaining for cluster of differentiation 117 (CD117) (magnification×400). C: Immunohistochemical study revealed positive immunostaining for vimentin (magnification×400). D: Direct sequencing analysis of DNA from patient no. 2 showed a point mutation at codon 559 in KIT exon 11. E: Histopathological study showed viable tumor cells even after imatinib treatment (HE, magnification×400). F: Immunohistochemical study revealed positive immunostaining for CD117 (magnification×400). G: Immunohistochemical study revealed positive immunostaining for vimentin (magnification×400). H: Direct sequencing analysis of DNA from patient no. 2 showed a point mutation at codon 559D in KIT exon 11 and a point mutation at codon 654 in KIT exon 13.
Acknowledgements
The Authors would like to thank Novartis (Taiwan) Co. Ltd. for their financial support of the genetic analysis presented in this manuscript.
Footnotes
-
↵* These Authors contributed equally to this study.
- Received July 11, 2014.
- Revision received August 28, 2014.
- Accepted August 29, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}