


Abstract
Aim: Up-regulation of caveolin-1 (CAV1) is associated with aggressive prostate cancer. Among Caucasian and African-American patients, plasma CAV1 levels are elevated in patients with castration-resistant prostate cancer (CRPC), but not in those with hormone-sensitive prostate cancer (non-CRPC), which implies that CAV1 could be a therapeutic target for CRPC. Here, we evaluated associations between plasma CAV1 levels and these types of cancer in Japanese men, and CAV1 expression in PC3 (CRPC) and LNCaP (non-CRPC) cell lines. Materials and Methods: Plasma samples were obtained from 58 patients with prostate cancer: 36 with CRPC and 22 with non-CRPC. Enzyme-linked immuno sorbent assay (ELISA) kits were used to determine CAV1 plasma levels; qRT-PCR and western blots were used to evaluate the expression of CAV1 mRNA and protein in cell lines. Results: Plasma CAV1 levels in patients with CRPC were greatly higher than in those with non-CRPC (1.46±1.37 ng/ml in CRPC; 0.56±0.32 ng/ml in non-CRPC, p<0.004). Western blot and real-time qRT-PCR showed CAV1 protein and mRNA in PC3 cells to be significantly overexpressed compared to its expression in LNCaP cells (p<0.0001). Conclusion: Our results showed a relationship between CAV1 expression and prostate cancer progression, and support the possibility of CAV1 as a therapeutic target for CRPC.
Prostate cancer is the sixth leading cause of cancer-related death among Japanese men (1). In most cases, death from prostate cancer results from metastatic disease. Understanding the mechanisms underlying the progression of prostate cancer will facilitate the development of biomarkers and novel therapeutic strategies to control this devastating malignancy. Caveolin-1, encoded by CAV1, is a major structural component of the caveolae, which are specialized plasma membrane invaginations involved in multiple cellular processes such as molecular transport, cell adhesion and signal transduction (2). Although CAV1 may suppress tumorigenesis under some conditions (3), it is associated with, and contributes to, malignant progression through various mechanisms (4, 5).
The role of CAV1 in cancer cells remains controversial. It is down-regulated in tumors such as human ovarian carcinoma (6) and head and neck squamous cell carcinoma (SCC) (7), which implies a tumor-suppressor role. However, CAV1 overexpression is associated with more aggressive behavior, increased recurrence and poorer prognosis in prostate cancer in Caucasian patients (8) and in hepatocellular carcinoma (9). As these discrepancies show, whether CAV1 up- or down-regulation is an optimistic sign in tumorigenesis, is unclear.
Emerging evidence of a role for CAV1 in prostate cancer prompted us to investigate its activity in different prostate cancer types, such as castration-resistant prostate cancer (CRPC) and hormone-sensitive prostate cancer. We, therefore, aimed to determine the plasma CAV1 levels and their association with prostate cancer progression. We also analyzed CAV1 expression in the PC3 (CRPC model) and LNCaP (non-CRPC model) cell lines. To the best of our knowledge, this is the first study to evaluate the contribution of plasma CAV1 levels to different types of prostate cancer among Japanese patients.
Materials and Methods
Study participants. The study population consisted of 58 Japanese men with prostate cancer, including 36 with CRPC and 22 with non-CRPC, such as organ-confined tumors. These patients were treated at the Department of Urology, in the Miyazaki Medical University Hospital and its related hospitals between August 2011 and October 2012. Tumor grade was evaluated in these samples using the Gleason scoring system. All participants were informed of the details, procedures and objectives of this study. This study was approved by the Ethics Committee of Miyazaki Medical University and related hospitals (Approved number 847, August 2011).
Enzyme-Linked Immuno Sorbent Assay (ELISA) protocols. Blood (5 ml in EDTA2Na) were collected by venipuncture and immediately after blood sampling, plasma was obtained by centrifugation at 12,000 rcf ×g for 15 min at 4°C and stored at −80°C until later analysis. To determine plasma CAV1 levels, the Human Caveolin-1 ELISA Kit (Uscn Life Science, Inc., Wuhan, China; detection range=0.24-15 ng/ml) was used according to the manufacturer's instructions. To detect the concentration of plasma CAV1 levels using this ELISA kit, the 60 ng/ml CAV1 standard was diluted to a concentration range of 0.24-16 ng/ml in duplicate experiments and the absorption was measured
Cell cultures. The androgen-dependent LNCaP and androgen-independent PC3 cancer cell lines (ATCC, Manassas, VA, USA) were grown in Dulbecco's modified Eagle's medium (DMEM; Gibco, Carlsbad, CA, USA) supplemented with 10% fetal bovine serum (FBS; Gibco). Cells were grown in 9.6-cm2 cell culture dishes at 37°C in a humidified atmosphere of 5% CO2. Cells were grown to 80% confluence and harvested between passages four and six by trypsinization for analysis. For western blots, cells were seeded in 9.6 cm2 dishes into 2.5 ml of culture medium for LNCaP cells and PC3 cells respectively. Media were changed every day for five days; cells grown to 90% confluence were passaged by trypsinization. After centrifugation, the cell pellet was resuspended in 1 ml of protease inhibitor, and the cells were counted on a hemocytometer. Aliquots containing 50×103 cells in protease inhibitor were frozen at −80° until used.
Western blot analysis. To analyze protein expression, a western blot method was used. Briefly, samples of protein of 50×103 cells were separated on a 12% polyacrylamide gel and the proteins transferred to a polyvinylidene fluoride (PVDF) membrane (transblot transfer medium; BioRad, Hercules, CA, USA). The membrane was probed with rabbit anti-cav1 (Cell Signaling Co., Boston, MA, USA), 1:1,000 diluted in Phosphate Buffered Saline (PBS) with 0.02% (v/v) Tween-20 and 3% (w/v) milk powder. Membranes were incubated with horseradish peroxidase-conjugated goat anti-rabbit immunoglobulins (Dako, Glostrup, Denmark), before detection of antibody binding by chemiluminescence (GE, Tokyo, Japan). Band intensity was measured using a LAS3000 (FUJIFILM, Tokyo, Japan) imaging densitometer and quantified by densitometry using the Image J software (National Institutes of Health, Bethesda, MD, USA).
Real time qRT-PCR. Total RNA was extracted from cells using the RNA Mini kit (Ambion, Paisley, OR, USA) according to the manufacturer's instructions. Genes of interest were amplified from 2 mg DNase I-treated total RNAs using Thunderbird Reverse Transcriptase (ToYoBo, Tokyo, Japan) and random primer. The primers used for real time qRT-PCR were as follows: CAV1: forward: 5’-CGCGACCCTAAACACCTCAA-3’, reverse: 5’-GCCGTCAAAACTGTGTGTCC-3’ (63°C, 40 cycles); and Glyceraldehyde-3-phosphate dehydrogenase (GAPDH): forward: 5’-ACCACAGTCCATGCCATCAC-3’, reverse: 5’-TCCACCACCC TGTTGCTGTA-3’ (63°C, 40 cycles). For real-time qRT-PCR, transcripts were quantified using Applied Biosystems 7300 Real-Time PCR System (Life Technologies, Carlsbad, CA, USA) and Thunderbird SYBR qPCR Mix (ToYoBo, Tokyo, Japan). Experiments were repeated at least three times in triplicate; GAPDH was used as an internal control.
Clinicopathological features.
Statistical analysis. Statistical analysis was performed using the R i386 2.15.1 software package (Wirtschaftsuniversität Wien, Vienna University of Economics and Business, Vienna, Austria). The significance of differences in plasma CAV1 levels among CRPC and non-CRPC patients were determined by Student's t-tests. p<0.05 was considered statistically significant.
Results
Patients' backgrounds and plasma CAV1 levels. Clinicopathological characteristics of patients with CRPC and non-CRPC are summarized in Table I. The mean ages (in years) of patients in the CRPC and non-CRPC groups were 68.3±7.4 (range=61-75) years and 66.9±8.3 (range=59-75) years, respectively. There were no significant differences between the two groups in terms of mean age distribution (p=0.18). The mean serum prostate-specific antigen (PSA) levels of the CRPC and non-CRPC groups differed significantly (41.8±28.4 ng/ml and 8.8±4.1 ng/ml, respectively; p<0.001). In addition, patients in CRPC and non-CRPC groups differed significantly in clinicopathological characteristics such as Gleason grade, T grade and metastasis (extent, lymph node and bone) (Table I). Mean plasma CAV1 levels in the CRPC group were much higher than in the non-CRPC group (CRPC=1.46±1.37 ng/ml, non-CRPC=0.56±0.32 ng/ml; p<0.004; Figure 1).

Plasma Caveolin-1 (CAV1) levels (ng/ml). Plasma CAV1 levels were significantly higher in the CRPC group (1.46±1.37 ng/ml; n=36) than in the non-CRPC group (0.56±0.32 ng/ml; n=22, p<0.004). Boxplot; The boundary of the box closest to zero indicates the 25th percentile, a line within the box marks the median, and the boundary of the box farthest from zero indicates the 75th percentile. Error bars above and below the boxes indicate the 90th and 10th percentiles, respectively.
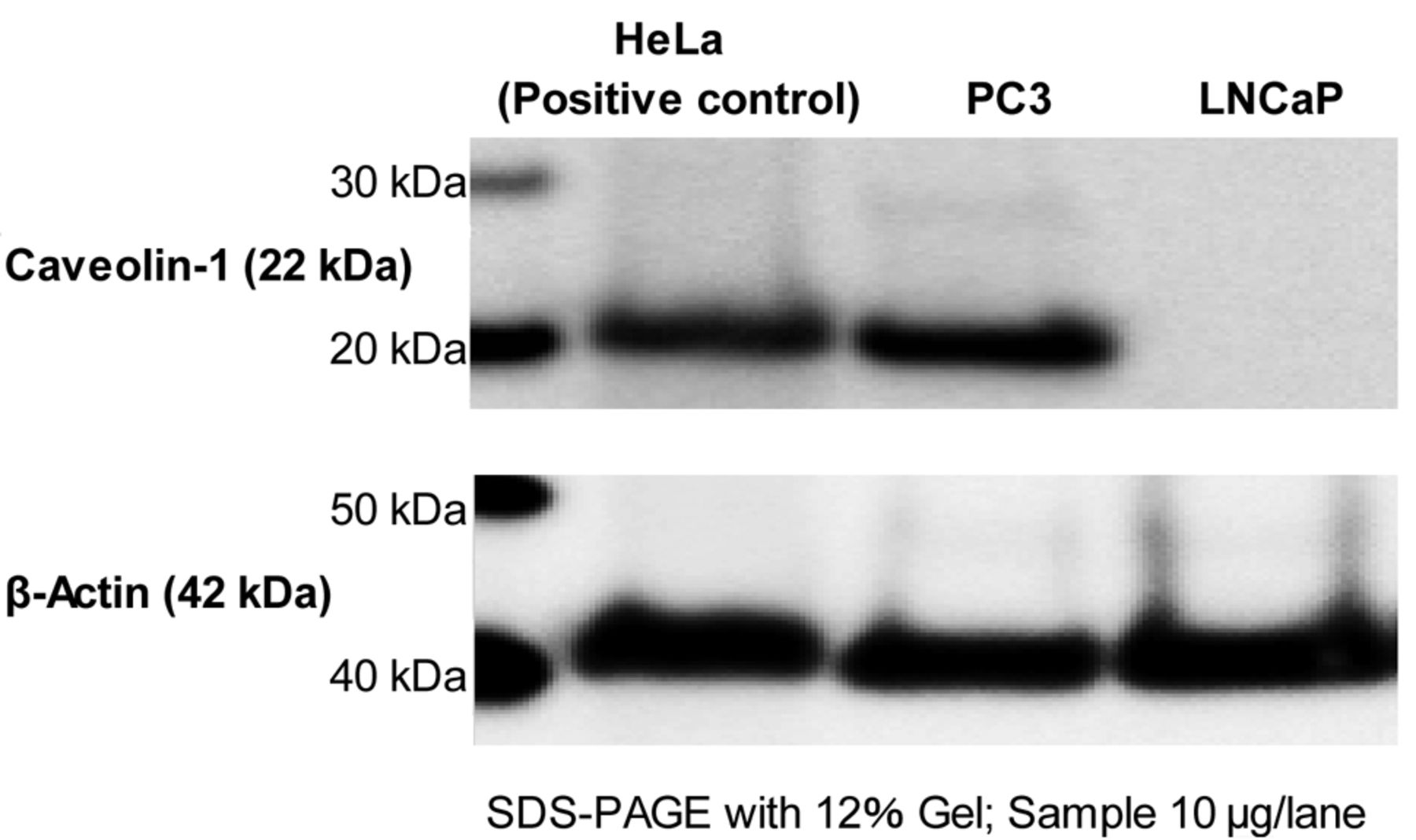
Western blot analysis. Western blot showed a single immunoreactive band for the CAV1 protein expression at 22 kDa. The loading control, β-Actin at 42 kDa, confirmed that there was equal protein loading (Figure 2). Western blot analysis showed that CAV1 expression was significantly greater in PC3 cells than in LNCaP cells.
Real-time qRT-PCR. Real-time qRT-PCR was performed by prostate cancer cells to examine the CAV1 mRNA expression, which was found to be significantly greater in PC3 cells than in LNCaP cells (CAV1/GAPDH, PC3 vs. LNCaP=1 vs. 0.002; p<0.001).
Discussion
This study investigated whether CAV1 expression varied between Japanese patients with CRPC and in patients with androgen-sensitive prostate cancer. We also investigated differences in CAV1 protein and mRNA expression between PC3 cells (CRPC model) and LNCaP cells (non-CRPC model). Our data showed increasing levels of plasma CAV1 to have prognostic potential for prostate cancer progression.
Western blot analysis showed significantly greater expression of Caveolin-1 (CAV1) in PC3 cells than in LNCaP cells.
CAV1 has been linked with various types of cancers over the past decade, during which it was most extensively studied in breast and prostate cancer. It was found that CAV1 levels in tumor tissue and in plasma may be associated with tumor protection or progression (10). In prostate cancer, in particular, elevated CAV1 expression was observed in tumor tissues in humans and in a mouse model, compared to non-tumor tissues (11-13). Another study implied that CAV1 and cancer-promoting growth factors collaborate in prostate cancer progression, although more evidence is needed (14). CAV1 is thought to suppress tumor growth and metastasis in human breast and colon cancer (15, 16). However, CAV1 function may differ among different organs, and CAV1 could thus exert opposing effects, resulting in promotion or suppression of tumor progression. For example, CAV1 expression increased in tumor samples from the kidney, prostate and stomach, and re-expression has been found in some advanced adenocarcinomas (17). Elevated CAV1 expression is associated with progression of some adenocarcinomas, such as prostate carcinoma (18), and in adult T-cell leukemia (19). Interestingly, activated CAV1 expression is associated with higher grades of prostate cancer, although few significant relationships have been identified between CAV1 expression and tumor multiplicity, recurrence, progression, or overall survival (16).
Li et al. showed that CAV1 was secreted by mouse and human prostate cancer cell lines, and that secreted CAV1 promoted cancer cell survival and clonal growth in vitro (20, 21). They further showed that tumor cell-secreted CAV1 promoted pro-angiogenic activities in prostate cancer through the phosphoinositol-3-kinase (PI3K)–protein kinase B (AKT)–endothelial nitric oxide synthase (eNOS) signaling pathway (22). Regarding the mechanisms through which CAV1 mediates oncogenic activities, they showed CAV1 to hold AKT in an activated form in prostate cancer cells by binding to and inhibiting the serine/threonine protein phosphatases PP1 and PP2A (14). Thus, engagement of CAV1 as a tumor metastasis promoter depends on the cellular context, and at the molecular level, by the signaling molecules and signaling pathways affected and regulated by CAV1. We hypothesize that altered CAV1 expression interferes with homeostasis, and increases the frequency of prostate cancer.
Our results also show that CAV1 is associated with tumor progression and metastasis, and is distinctly elevated in androgen-resistant tumors. Therefore, CAV1 could be a marker for an aggressive form of cancer (18, 22, 23-27).
Suppression of CAV1 expression has been shown to restore sensitivity to androgens in androgen-insensitive tumors (13). Our findings, together with data from other studies, suggest that CAV1 is involved in disease pathogenesis and progression. Further study of its role in prostate cancer can contribute to the understanding of this disease, and possibly offer novel targeted therapeutic approaches. Although associations between CAV1 and high-risk tumors were identified in this study, we still cannot confirm CAV1 to be a marker for high-risk aggressive tumors, even at the phase when tumors are localized in the prostate and thus are still curable. To do so would require monitoring CAV1 levels in a follow-up study over the course of prostate cancer progression from its initial stages. Our results should also be verified in a larger group of patients, including those with disseminated disease.
Footnotes
-
Conflicts of Interest
The Authors have no potential conflicts of interest.
- Received February 28, 2013.
- Revision received March 28, 2013.
- Accepted March 29, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}