


Abstract
Background/Aim: We have previously reported that low expression of excision repair cross-complementing-1 (ERCC1), class III β-tubulin (tubulin), thymidylate synthase (TYMS) and ribonucleotide reductase-M1 (RRM1) is indicative of a favorable prognosis in patients with c-N2,3 non-small cell lung cancer (NSCLC) treated with surgery after induction chemoradiotherapy. In the present study, we prospectively explored the tailor-made treatment menu for induction chemotherapy according to the status of biomarkers, and evaluated the biomarker status pre- and post-chemotherapy. Patients and Methods: Twenty-five patients with pathologically-proven NSCLC who were not appropriate candidates for initial surgery were enrolled (October 2010 to June 2012, stage IIIA/B/IV1a/1b;14/5/2/4 respectively). Immunohistochemistry was performed to evaluate intratumoral expression of biomarkers. Epidermal growth factor receptor (EGFR) mutation was evaluated by direct sequencing. Two to four cycles of chemotherapy were performed with or without concurrent radiation (50 Gy). Results: Docetaxel (n=12), pemetrexed (n=4), S-1 (n=4), docetaxel-plus-bevacizumab (n=3), and pemetrexed-plus-bevacizumab (n=2), in combination with platinum were selected for the therapeutic regimen. Twenty-one (84.0%) patients exhibited good partial response, and underwent complete resection without major morbidity or mortality. Of these 21 patients, four achieved a pathologically-complete response (PCR), and 10 achieved a major pathological response. The 3-year overall survival rate was 58.7% for the 25 patients overall, and the 2-year overall survival rate was 73.6% for patients who underwent surgery. Among the 17 patients who underwent resection (except for four with PCR), the status of ERCC1, tubulin, TYMS, RRM1 and EGFR changed markedly after chemotherapy in six patients, eleven patients, eight patients, nine patients and one patient, respectively. Conclusion: Chemotherapy followed by surgery on the basis of biomarker examination is a challenging approach for patients with advanced NSCLC who otherwise have poor outcomes. Post-chemotherapy biomarker status changed markedly in many cases.
Recent reports have demonstrated that levels of several biomarkers correlate with the response to chemotherapy (1-6). We reported that patients with non-small cell lung cancer (NSCLC) of cN2 or 3 with low protein expression of both expression of excision repair cross-complementing-1 (ERCC1) and class III β-tubulin (tubulin) are promising candidates for surgery after carboplatin-taxane chemoradiotherapy and that the expression levels of ERCC1, tubulin, ribonucleotide reductase-M1 (RRM1) and thymidylate synthase (TYMS) were significant prognostic factors (7). There was no correlation shown between RRM1, ERCC1 and tubulin expression. Furthermore, no significant differences were observed in the relationship between the percentage of tumor cells positive for each biomarker and patient variables, such as tumor status, nodal status, clinical stage, and histology. This suggests that effective drugs can be selected even for patients with advanced NSCLC. If an optimum chemotherapy regimen can be selected for an individual on the basis of the tumor biomarker status, salvage surgery and cure may be possible. However, our previous study was retrospective and investigated only post-chemotherapy biomarker levels; therefore, any changes in the biomarker profiles according to treatment were not characterized.
Although there has been considerable progress in the development of targeted therapy and new-generation cytotoxic agents (8), chemoresistance (innate or acquired) remains a problem in many cases (9, 10). Various investigators have attempted to characterize the molecular mechanisms of chemoresistance. These mechanisms include efflux of the chemotherapeutic agent from the tumor cell, modification of drug targets, mutation in mitotic checkpoint signals, drug sequestration, de-toxification of cytotoxic agents, and enhanced DNA repair mechanisms (10). Another possible mechanism of chemoresistance may be related to changes in biomarker profiles.
In the present prospective study, we examined the pre- and post-chemotherapy biomarker status and tailored treatment with chemotherapy followed by surgery on the basis of pre-treatment biomarker profiles for patients with advanced NSCLC who were not appropriate candidates for upfront surgery. Furthermore, we examined the relationship between chemoresistance and changes in the biomarker profile.
Patients and Methods
Patients and treatments. This study was approved by the Institutional Review Board of Kagawa University (Heisei 14-7), and written informed consent was obtained from all patients. Between October 2010 and June 2012, 25 patients with pathologically proven advanced NSCLC were enrolled. Most cases were bulky N2-N3 tumor (17/25; 68%), including treatable single brain metastasis and adrenal metastasis. Pre-treatment biopsy was performed in all patients in this study. The intratumoral expression of ERCC1, tubulin, TYMS and RRM1 were measured by immunohistochemistry as reported previously (7). Epidermal growth factor receptor (EGFR) mutation status was analyzed by direct sequencing (11).
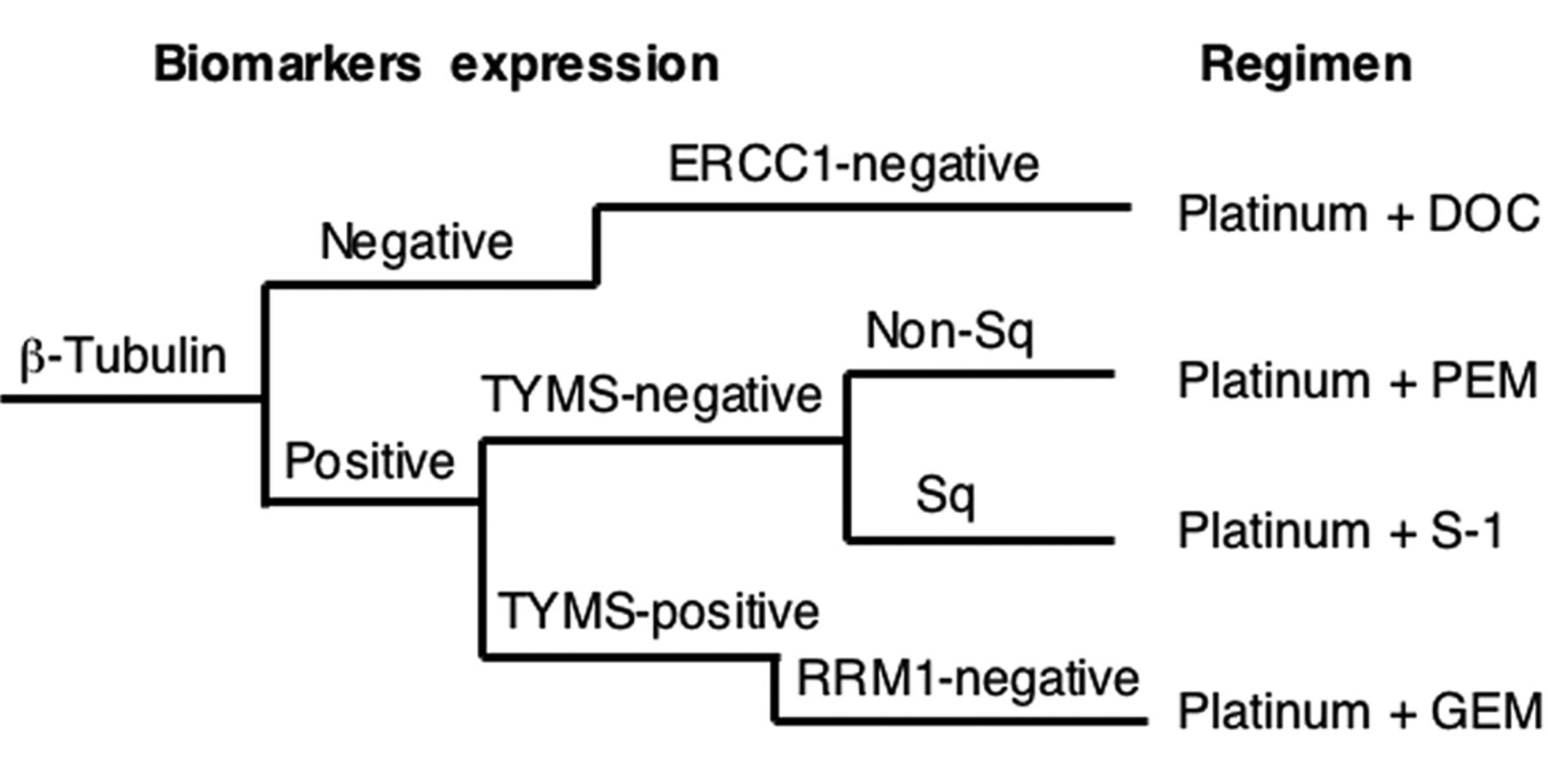
Drug selection was conducted as follows: i) patients with tubulin-negative carcinoma received platinum and docetaxel; ii) patients with TYMS-negative and tubulin-positive non-squamous carcinoma received platinum and pemetrexed; iii) patients with TYMS-negative and tubulin-positive squamous carcinomas received platinum and S-1; iv) patients with RRM1-negative tumors received platinum and gemcitabine; v) when all biomarkers were positive or when the patient was allergic to the assigned drug, alternative selection was docetaxel or second-best drug; and vi) bevacizumab was given to patients with stage IV non-squamous carcinoma who were not candidates for local radiotherapy. Concurrent thoracic irradiation at a dose of 50 Gy was performed in patients with stage III disease (Figure 1). All patients underwent a previously described induction therapy for up to four cycles (7). Briefly, this regimen consisted of carboplatin (area under the curve, 6 mg/ml min; 30-min intravenous infusion), docetaxel (60 mg/m2, 3-h intravenous infusion), pemetrexed (500 mg/m2) or bevacizumab (7.5 mg/kg) on day 1 at weeks 1, 2, 3, and 5 plus concurrent thoracic irradiation at a dose of 50 Gy. For the carboplatin and S-1 arm, S-1 (80 mg/m2) was given from day 1 to day 15 in every cycle, Gemcitabine chemotherapy was not given as a result. For radiotherapy, an area including the hilum of the lung and mediastinum with a 1.5-cm margin from the periphery of the primary lesion was irradiated with 2 Gy/day from week 5 along with concurrent thoracic irradiation to a dose of 50 Gy. The patients received irradiation five times per week, with two non-irradiation days.
Routine re-evaluation was carried out according to the New Guidelines for Evaluation of the Treatment Response of Solid Tumors (12). The decision to proceed with surgery was made on the basis of findings from chest computerized tomography (CT) and Fluorodeoxyglucose Positron Emission Tomography (FDG-PET) imaging. Marked shrinkage of the tumor and more than 70% reduction of a maximum standardized uptake value (SUVmax) of tumor were taken into consideration (13). Following re-evaluation, surgery was attempted for patients in whom R0 resection was deemed possible. The pathological effect of induction therapy was evaluated according the General Rules for Clinical and Pathological Record of Lung Cancer, Sixth Edition (14), as a pathologically complete response (complete cancer cell death), a major response (fewer than one-third of cancer cells viable), or a minor response (more than one-third of cancer cells viable). Twenty-five patients with stage IIIA to IV NSCLC were investigated, as shown in Table I. These patients included 12 patients with adenocarcinoma, 11 patients with squamous cell carcinomas, and two with other carcinoma types.

The criteria used for drug selection in the present study. β-Tubulin: class III β-tubulin; TYMS: thymidylate synthase; RRM1: ribonucleotide reductase M1; Sq: squamous cell carcinoma; Non-Sq: non squamous cell carcinoma; DOC: docetaxel; PEM: pemetrexed; GEM: gemcitabin.
Immunohistochemistry. Biopsy was performed on all patients. Tumor cell samples were collected via bronchoscopy, mediastinoscopy or washing solution and were embedded with glucomannan as a cell block (15). Immunohistochemistry was performed as reported previously (6, 7). A mouse monoclonal antibody against ERCC1 (FL-297; Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA; diluted 1:200), a rabbit monoclonal antibody against tubulin (EP1569Y; Epitomics, Inc., Burlingame, CA, USA; diluted 1:500), a rabbit monoclonal antibody against TYMS (diluted 1:500; kindly provided by Dr. M. Fukushima, Tokushima Research Center, Japan), and a rabbit polyclonal antibody against RRM1 (10526-1-AP; Protein Tech Group, Chicago, IL, USA; diluted 1:500) were used. Formalin-fixed paraffin-embedded tissue was mounted on poly-L-lysine-coated slides. The sections were deparaffinized and rehydrated, and the slides were then heated in a microwave oven for 10 min in 10 μmol/l citrate buffer solution at pH 6.0. After quenching the endogenous peroxidase activity with 0.3% H2O2 (in absolute methanol) for 30 min, duplicate sections were incubated overnight with each of the respective primary antibodies. The slides were then incubated for 1 h with biotinylated anti-mouse or anti-rabbit IgG secondary antibodies (Vector Laboratories, Inc., Burlingame, CA, USA). The sections were incubated with avidin-biotin-peroxidase complex (Vector Laboratories, Inc.) for 1 h, and antibody binding was visualized with 3,3’-diaminobenzidine tetrahydrochloride. Lastly, the sections were lightly counterstained with Mayer's hematoxylin.
Patients' characteristics.
All immunostained sections were independently evaluated by two investigators who had no knowledge of the patient characteristics. A sample was classified as: ERCC1-positive tumor if >30% of the tumor cells exhibited positive staining; tubulin-positive tumor if >30% of the tumor cells were positively stained for tubulin; RRM1-positive tumor if >40% of the tumor cells were positively stained for RRM1. For evaluation of TYMS, all sections were scored in a semiquantitative manner according to a method described previously, which reflects both the intensity and percentage of cells showing staining at each intensity. Intensity was classified as 0 (no staining), +1 (weak staining), +2 (distinct staining), or +3 (very strong staining). A value designating the ‘HSCORE’ was obtained for each slide using the following algorithm: HSCORE= ∑(I X PC), where I and PC represent the staining intensity and the percentage of cells staining at each intensity, respectively, and the corresponding HSCOREs were calculated separately on each slide. If the HSCORE for TYMS in a given specimen was >30, the sample was classified as TYMS-positive (7).

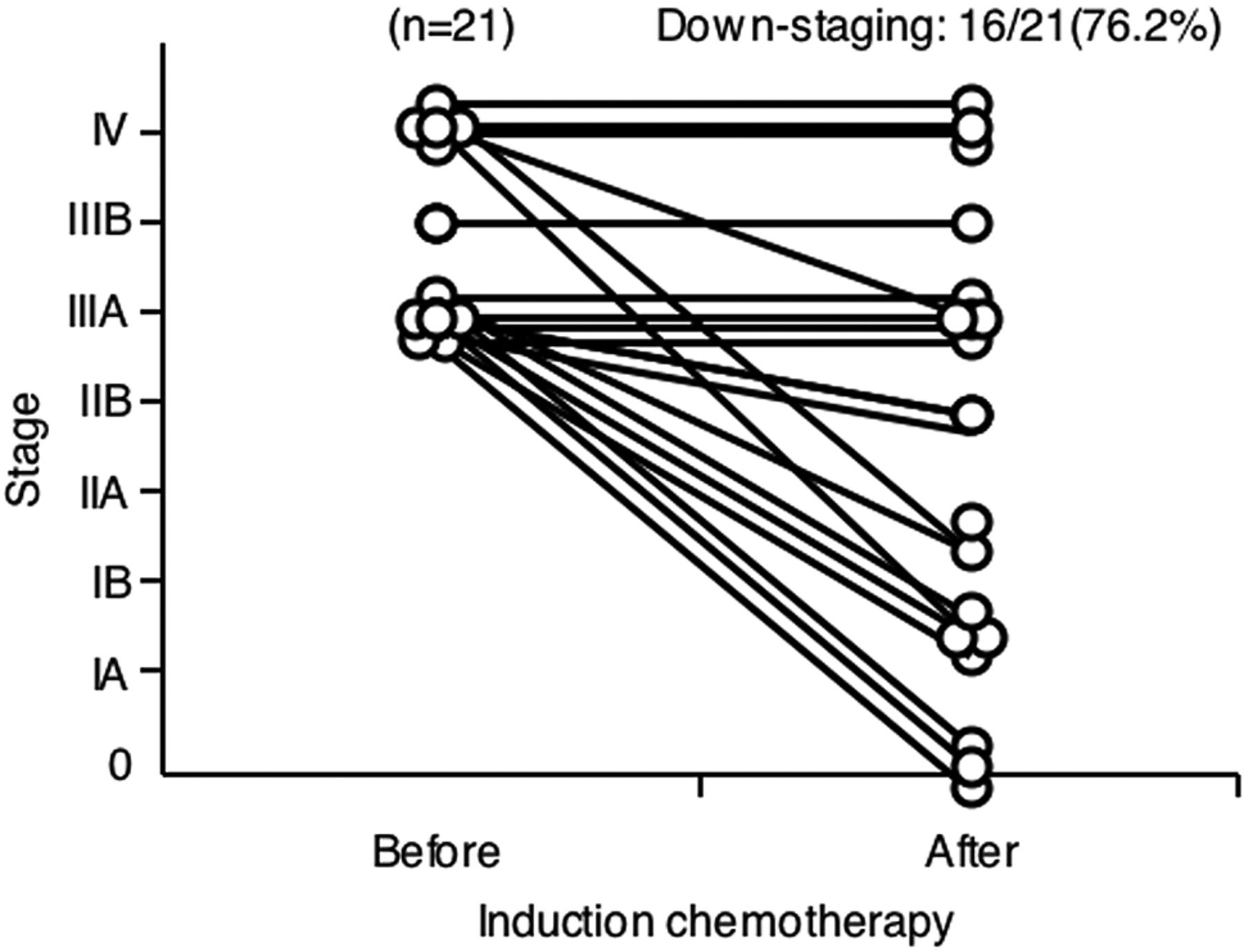
Stage change after induction chemotherapy in 21 patients who underwent surgery.
Statistical analysis. Overall survival was defined as the time from treatment initiation to the date of death due to any cause. The Kaplan-Meier method was used to estimate the probability of overall survival as a function of time, and differences in the survival of patient subgroups were compared using Mantel's log-rank test. All p-values were based on two-tailed statistical analysis, and differences at p<0.05 were considered to be statistically significant.
Results
Response to induction chemotherapy and surgery. Docetaxel (n=12), pemetrexed (n=4), S-1 (n=4), docetaxel plus bevacizumab (n=3), and pemetrexed plus bevacizumab (n=2), were selected for the therapy on the basis of the biomarker status. Radiological evaluation of the response to induction therapy showed that 21 (84.0%) tumors had a partial response, whereas three (12.0%) exhibited stable disease (SD) and one (4.0%) exhibited progressive disease (PD) out of the 25 patients enrolled in this study (Table I). In patients with SD and PD, the findings of FDG-PET did not improve. There were no significant differences in the response rates when comparing different regimens.
All surgery was performed via open thoracotomy, and systematic mediastinal lymph node dissection was performed as well. In all cases, the bronchial stumps were covered with intercostal muscle or pericardial fat. Twenty-one patients with good partial response underwent R0 resection without major morbidities or mortalities. Lobectomy or bi-lobectomy was performed in 19 patients, and pneumonectomy was performed in two out of 21 patients. With regard to the pathological effect of induction therapy, complete response was observed in 4 patients (19.1%), major response was observed in 10 patients (47.6%), and minor response was observed in 7 patients (33.3%) out of the 21 who underwent surgery. There were no significant differences in the pathological response when comparing different regimens. With regard to the stage, 16 (76.2%) out of 21 patients achieved tumor downstaging after induction chemotherapy (Figure 2).
Changes in biomarkers in 17 patients with major or minor pathological response after chemotherapy.
Postoperative biomarker status. Postoperative biomarker status was markedly different in many cases. Among the 17 patients who underwent resection (except for four patients with pathologically complete response), the status of ERCC1, tubulin, TYMS, RRM1, and EGFR changed after chemotherapy in six, 11, eight, nine and one patient, respectively (Table II). Negative tubulin status changed to positive in five out of seven patients with an absolute indication for docetaxel therapy (tubulin-negative) after docetaxel chemotherapy. Negative TYMS status changed to positive in two out of three patients with an absolute indication for pemetrexed therapy (TYMS-negative and non-squamous cell carcinoma) after pemetrexed chemotherapy. Similarly, negative TYMS status changed to positive in two out of three patients with an absolute indication for S-1 therapy (TYMS-negative and squamous cell carcinoma) after S-1 chemotherapy. Among nine patients whose biomarkers changed from negative to positive, two cases of minor pathological effect and six of intratumoral lymphatic invasion were recorded.
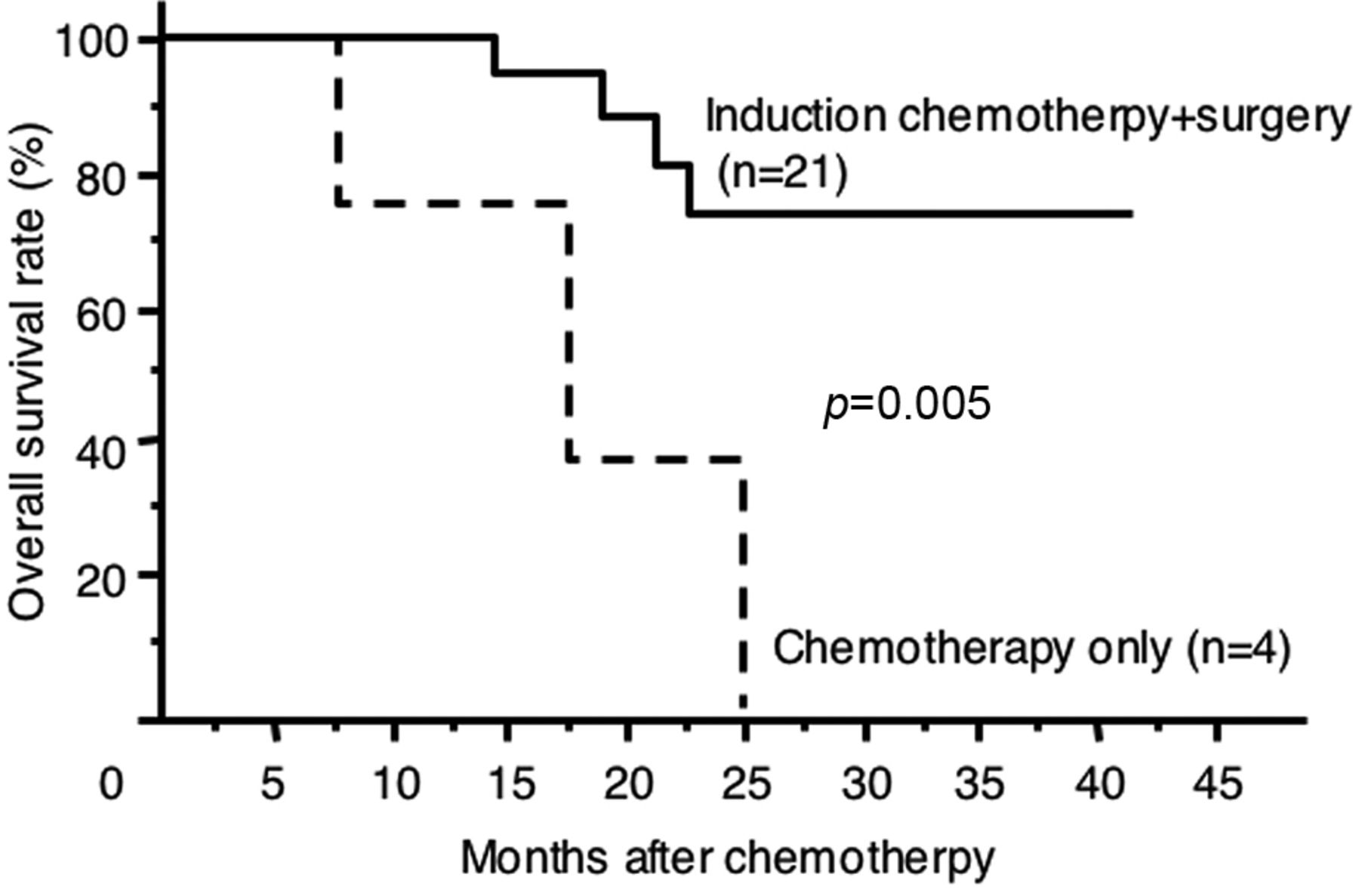
Overall survival of 25 patients with non-small cell lung cancer after induction chemotherapy.
Overall survival. The 3-year overall survival rate was 58.7% for the 25 patients. The 2-year overall survival was 73.6% for patients who underwent surgery after induction chemotherapy and was 37.5% for patients who did not undergo surgery. The overall survival rate of patients without surgery was significantly worse than that of patients who underwent surgery after induction chemotherapy (p=0.005, Figure 3). Thus far, 12 out of 21 patients have developed postoperative recurrence (four at the primary site, four with lung metastasis, two of brain metastasis and two with adrenal metastasis).
Discussion
We have reported that patients with cN2 or 3 NSCLC with low expression of both ERCC1 and tubulin are promising candidates for surgery after carboplatin-taxane chemoradiotherapy and that expression of ERCC1, tubulin, RRM1, and TYMS were significant prognostic factors in such patients (7). Previous studies demonstrated that there was no correlation between RRM1, ERCC1, and tubulin expression (7) and that the efficacy of new-generation cytotoxic agents for advanced NSCLC is equivalent to that of platinum-based chemotherapy (16). Furthermore, pemetrexed and S-1 are not inferior to first-line chemotherapy for advanced NSCLC (17, 18). Therefore, an appropriate chemotherapy can be selected for any individual on the basis of biomarker status, without any disadvantages in terms of outcomes.
Our previous study had a number of limitations. For example, it was retrospective in nature, and it only investigated biomarkers after chemotherapy. Thus, it was not possible to identify any biomarkers that correlated with pathologically-complete response. Furthermore, all patients underwent carboplatin-taxane induction chemotherapy, and therefore the true significance of TYMS and RRM1 status for prediction of survival was unclear (7). As a result, we conducted the present prospective study.
Various biomarkers have been described that can predict for response to cytotoxic agents. A sub-analysis of data from The International Adjuvant Lung Cancer Trial (IALT) suggested that ERCC1 was an important biomarker of the response to platinum chemotherapy (1). The Lyon group reported that low expression of tubulin was associated with better survival in patients with advanced lung cancer who were treated with a paclitaxel-based regimen (2). The Spanish Lung Cancer Group reported that a low level of RRM1 mRNA was associated with better survival in patients with advanced lung cancer who received a gemcitabine/cisplatin regimen (3). We also reported that low expression of TYMS was associated with better survival in patients receiving adjuvant chemotherapy with a UFT-based regimen (4). A Korean group reported that low expression of TYMS was significantly associated with better clinical outcomes in patients with non-squamous NSCLC who received pemetrexed-based chemotherapy (5). The Memorial Sloan-Kettering Cancer Center group reported that induction chemotherapy with bevacizumab for non-squamous carcinoma was feasible and promising (19).
Based on this tailor-made treatment, 21 patients who exhibited good partial response were able to undergo R0 resection successfully without any major morbidity or mortality. With regard to pathological effects, a complete response or major response was achieved in 66.7% of patients who underwent surgery, and down-staging was observed in 76.2% of such patients. The 3-year survival rate was 58.7% for the 25 patients overall and was 73.6% for patients who underwent surgery after induction chemotherapy.
Chemoresistance can develop during treatment in many cases (9, 10). We unexpectedly found out that biomarker status changed markedly after chemotherapy. When using key cytotoxic agents according to biomarker status, the corresponding negative biomarker status changed to positive after chemotherapy, especially with regard to tubulin. This may be because innately-chemoresistant clones may survive after chemotherapy or because biological profiles may change during chemotherapy. In our limited experience, among 9 patients whose biomarker changed from negative to positive, two cases with minor pathological effect and six with intra-tumoral lymphatic invasion were recorded. Minor pathological effect and intra-tumoral lymphatic invasion are indicative of poor prognosis (13, 20). This change in biomarker status may be related to chemoresistance that develops during chemotherapy. Although we used platinum in all chemotherapy regimens, the change in ERCC1 status was minimal when compared with the markers' changes seen in other biomarkers. This suggests that platinum is a key cytotoxic agent. Change in EGFR mutation status was rare during conventional chemotherapy, suggesting that this mutation is fundamentally different from quantitative biomarkers, such as ERCC1 or tubulin.
This study had a number of limitations, particularly the small number of patients and the short observation time. Furthermore, the value of biomarker status remains inconsistent and controversial. The Canadian consensus recommendation on the use of biomarkers for treatment of NSCLC states there to be insufficient evidence that testing for ERCC1, breast cancer susceptibility gene (BRCA), tubulin, RRM1, and P53 influences clinical treatment decisions (21). Booton et al. reported that ERCC1 mRNA levels are not associated with response and survival of patients with advanced NSCLC after platinum-based chemotherapy (22). Gomez-Roca et al. reported differential expression of biomarkers between primary NSCLC and metastases (23). Despite this negative background, we have achieved promising early results in patients with advanced NSCLC.
In conclusion, our present prospective study, using a tailor-made treatment regimen according to the ERCC1, tubulin, TYMS and RRM1 status, achieved encouraging results in patiens with advanced NSCLC. Thus, chemotherapy followed by surgery on the basis of biomarker examination is a useful approach for patients with advanced NSCLC who otherwise have poor outcomes. Furthermore, as the post-chemotherapy biomarker status changed markedly in many cases, the biomarker status should be re-evaluated before starting new tailor-made treatment for adjuvant chemotherapy or treatment for recurrence.
Footnotes
-
Conflicts of Interest
None declared.
- Received September 19, 2013.
- Revision received October 29, 2013.
- Accepted October 30, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}