


Abstract
Background: Serum and plasma vascular endothelial growth factor (VEGF) were measured in children with a solid tumor to investigate which provides better prognostic information. Patients and Methods: Seventeen patients under treatment were divided into two groups: without (n 8) and with (n 9) detectable disease at radiological assessment (groups I and II). The control group consisted of 26 healthy children. VEGF was tested by enzyme-linked ELISA kit. Results: Serum VEGF concentrations in group II were statistically higher than those in group I (p<0.05) and those in controls (p=0.001), whereas the difference between group I and controls was not statistically significant (p=0.067). Plasma VEGF concentrations in group II were also statistically higher than those in group I (p<0.01) and those in controls (p=0.0001); the difference between group I and controls was also statistically significant (p=0.004). Conclusion: Plasma would be the more useful specimen for measurement of circulating VEGF in cancer childhood.
Angiogenesis, i.e. new blood vessel formation, is a prerequisite for the growth and metastasis of solid tumors (1-3). Angiogenesis is induced and maintained by angiogenic growth factor, secreted by the tumor cells. More than 20 angiogenic growth factors are known; out of these, vascular endothelial growth factor (VEGF) is one of the most potent (1-3). Thus, the angiogenic activity in cancer can be evaluated by the detection of VEGF expression in tumor tissue or by the measurement of VEGF concentrations in body fluids (3). Molecular biomarkers that are detectable in blood are especially intriguing because testing for them would be relatively low-cost and easily achievable. VEGF levels in cancer patients were significantly higher than in healthy individuals, as it was first reported in 1994 (4), and this finding was subsequently confirmed in patients with various types of tumor (5). In adults, circulating VEGF is elevated in a variety of malignant diseases, e.g. metastatic nasopharyngeal carcinoma, breast, colorectal, ovarian and renal carcinoma, and it has widely been used as a biomarker for cancer angiogenic activity (3, 5). It has been argued whether serum or plasma should be used for measuring circulating VEGF. In relation to the source of VEGF in the circulation, studies have shown that most of the VEGF in serum is derived from platelets during coagulation, and the plasma level of VEGF is much lower than the serum level (6, 7). There has been much debate whether the collection of serum (which causes the activation of platelets and VEGF release) is a true reflection of tumor angiogenic activity, or whether platelets, in fact act as scavengers of VEGF. Hence, some authors recommended that plasma instead of serum should be used in studies of circulating VEGF levels (9). However, the majority of studies about circulating VEGF were performed using serum samples and showed a positive correlation between serum VEGF and tumor stage or patient survival (5).
The pediatric malignancies differ markedly from adult type cancer in clinical and biological behavior. Few studies report on VEGF concentrations in pediatric solid tumor (10-17). Knowledge concerning circulating proangiogenic factors in children with solid tumors needs to be improved. The aim of the present study was to determine serum and plasma VEGF levels in children during treatment for a solid tumor and to investigate which would provide better prognostic information.
Patients and Methods
Patients and controls. This cross-sectional study was conducted over a period of 8 months at the Pediatric Oncology Day - Hospital of Sapienza University in Rome, Italy. During this period, consecutive patients admitted to the day-hospital for treatment of a solid tumor were enrolled after parental informed consent. Children with hematological malignancy and brain tumor, and/or documented infection were excluded from the study. The minimum values of blood counts required before VEGF measurements were: white blood cells >2,000/mm3 and platelets >150,000/mm3. Seventeen patients (9 males and 8 females) with extra central nervous system solid tumor were recruited. All the patients were under treatment for different solid tumors (Table I). Based on the extent of disease, patients were divided into group I, patients without detectable disease at radiological assessment, and group II, patients with detectable disease at radiological assessment. Eight cases (6 males, 2 females), with a median age of 147 months were enrolled in group I. Nine cases (3 males, 6 females), with a median age of 151 months were enrolled in group II. The circulating VEGF was tested three to four weeks after the last cycle of chemotherapy. Due to the absence of data on the normal value of circulating VEGF in healthy children, VEGF was analyzed in plasma and serum samples from healthy children and adolescents (matched for sex and age to the cancer patients) undergoing venopuncture in preparation for minor surgery. Informed consent was obtained from the child's or adolescent's parents. Children with a history of infectious disease during the month preceding the study were excluded. Twenty-six healthy children, 12 females and 14 males, with a median age of 153 months, were recruited. A population of 17 cancer patients with 34 blood samples, and a population of 26 healthy children with 52 blood samples were analyzed. Sixteen evaluations (8 in serum and 8 in plasma) were performed for group I patients, 18 evaluations (9 in serum and 9 in plasma) were performed for group II.
Blood collection and assay of VEGF. The originally isolated VEGF-A is part of a ligand family currently known to consist of six related proteins [VEGF-A, B, C, D, and E; and placental growth factor (PlGF)] (2-3). The predominant variant VEGF-A is usually measured and abbreviated as VEGF. The peripheral blood samples were collected in vacutainer collection tubes (Becton Dickinson, Rutherphord, NJ, USA) with sodium citrate (3.8%) as additive (plasma), or without additive (serum), after informed consent. Plasma samples were centrifuged (1,800 × g at 4°C, for 20 min) immediately after the aspiration, and the plasma was removed and stored at −80°C until analyzed. Serum samples were allowed to clot at room temperature for 30 min before centrifugation (1,800 × g at 4°C, for 20 min) and the serum was removed and stored at −80°C until analyzed. Blood samples from the healthy controls were obtained at the time of their routine examinations. VEGF measurement was carried out by utilizing a commercially available quantitative enzyme-linked immunoabsorbent ELISA kit (R&D Systems, Minneapolis, USA) according to the instructions given by the manufacturer. All samples were run in duplicate, the concentrations were interpolated from a VEGF standard curve. Concentrations were expressed as picograms per milliliter. The sensitivity of the test ranged from 5 pg/ml to 2000 pg/ml for the antibody determination. Samples with a higher concentration than 2000 pg/mL were diluted. Determinations of inter-assay and intra-assay variation coefficient reported by manufacturer varied from 6.2-8.8% and from 4.5 to 6.7%, respectively. Serum and plasma samples from 26 healthy children were used as VEGF normal controls.
Statistical analysis. Results are presented as the median and range values. The differences in VEGF distribution between groups were analyzed using the nonparametric Mann-Whitney rank-sum test for independent samples, both for serum and plasma. One-tailed Wilcoxon rank-sum test was used for group I and group II, and for group II and control comparisons, whereas a two-tailed Wilcoxon rank-sum test was used to compare group I and controls. In the comparison between group I and group II, the results were obtained from statistical tables and p was not punctually determined; in the other comparisons p-values were obtained with Normal approximation of statistic U, due to the bigger sample size of controls. The results were considered statistically significant if p-value was <0.05.
Diagnoses in group I and group II patients.
Results
Both serum and plasma median values of VEGF were higher in patients than in controls.
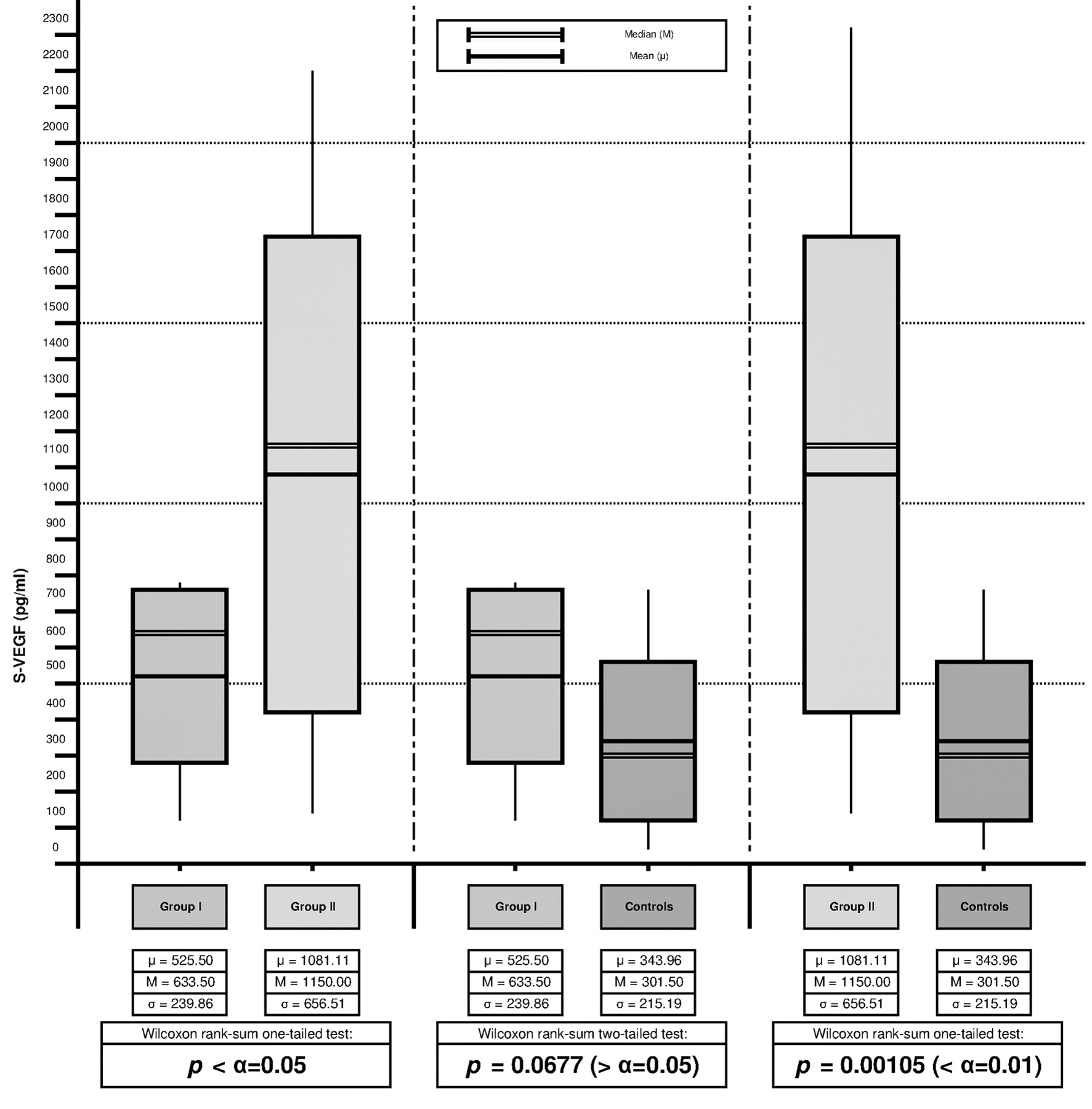
VEGF concentrations in serum. The median serum VEGF concentration was 301.50 pg/ml in the control group (range 41-757), 633.506 pg/ml (range 126-771) in group I patients and 1,150.00 pg/ml (range130-2202) in group II, respectively. Comparisons between group I and II and between group II and controls showed that in group II, the serum VEGF levels were statistically higher than those in group I and those in controls: 1,150.00 pg/ml vs. 633.50 pg/ml (p<0.05) and 1,150.00 pg/ml vs. 301.50 pg/ml (p=0.001), respectively. However, the difference in serum VEGF levels between group I and controls did not reach statistical significance: 633.50 pg/ml vs. 301.50 pg/ml (p=0.067) (Figure 1).
VEGF concentrations in plasma. The median plasma VEGF concentration was 18 pg/ml (range 6-91) in the control group, 48 pg/ml (range 6-72) in group I patients and 107 pg/ml (range 14-251) in group II, respectively. Plasma VEGF levels in group II were statistically higher than those in group I and those in controls: 107.00 pg/ml vs. 48.00 pg/ml (p<0.01) and 107.00 pg/ml vs. 18 pg/ml (p=0.0001), respectively. The difference in plasma VEGF levels between groups I and controls was also statistically significant: 48 pg/ml vs. 18 pg/ml (p=0.0047) (Figure 2).
Discussion
The present study confirms previously published studies, which found that circulating VEGF was higher in children with cancer than in healthy controls; in particular, a subgroup of patients with detectable disease at radiological assessment, was found to have higher plasma and serum VEGF levels compared to those of patients in complete remission. Additionally, the study indicated that plasma should be preferred as a specimen for VEGF measurements during treatment because it provides better prognostic information.

Comparison of vascular endothelial growth factor (VEGF) concentrations in serum of group I (n=8) and group II (n=9) patients and controls.
The available data in the literature suggest that in adults circulating VEGF is a useful marker of tumor status in most types of human cancer, and it is a useful predictor of patient survival (3-5). Moreover, the importance of serial measurements of VEGF during therapy has been underlined in the predict of disease progression (3-5).
Few studies report on VEGF concentrations in pediatric solid tumor. To the best of our knowledge, in childhood cancer, the data on circulating VEGF available so far, are those obtained in three published series investigating different childhood solid tumors (10-12) and in five studies investigating circulating VEGF in neuroblastoma, malignant lymphoma, Wilms tumor and rhabdomyosarcoma (13-17). Published data have shown that circulating VEGF levels tend to be higher in children with malignancies. In fact, serum VEGF levels were found to be elevated in 69 and in 40 children with different newly diagnosed cancer types (10, 12) and in 15 newly diagnosed and 30 treated patients (11). Moreover, Mizia-Malarz et al. described that high baseline serum VEGF levels were an unfavorable prognostic factor in 42 children with lymphoma and Okur et al. found serum VEGF levels increased in 36 children with lymphoma (13-14). In pre-treatment serum samples of 14 patients with Wilms' tumor, VEGF levels were three-fold higher than those in controls (15). More recently, serum VEGF was found to be significantly increased in 17 pediatric patients with newly diagnosed rhabdomyosarcoma (16). In these studies, VEGF levels were measured in the serum of childhood cancer patients, mostly at diagnosis. Only Skoldemberg et al. evaluated VEGF both in serum and plasma and found that serum, but not plasma VEGF concentrations were elevated in patients with newly diagnosed neuroblastoma as compared to controls (p<0.05). The authors concluded that since VEGF is thought to be transported in platelets, a platelet-free plasma sample might not properly reflect the VEGF content in the circulation (17). On the contrary, plasma was found to be the more useful specimen for measurement of circulating VEGF in our series of childhood cancer patients.

Comparison of vascular endothelial growth factor (VEGF) concentrations in plasma of group I (n=8) and group II (n=9) patients and controls.
There has been much debate on whether serum or plasma should be used for measuring circulating VEGF in patients with cancer. Several studies have indicated that serum is unsuitable for VEGF measurements since the significantly higher VEGF concentration in serum, compared to matched plasma concentrations, may be a reflection of degranulation of platelets and white blood cells during in vitro clotting, rather than a reflection of ongoing angiogenic activity in the tumor (18). In plasma, white cell and platelet degranulation is minimized by adding anticoagulatives to the blood samples, and as a consequence, plasma VEGF concentrations are up to 20-fold lower than the VEGF concentrations in matched serum (6). Therefore, it was suggested that plasma should be preferred as specimen for VEGF measurements (6). However, it has been shown that isolated platelets from patients with cancer contain more VEGF than isolated platelets from healthy controls (7). Moreover, the serum VEGF concentrations in patients with cancer with normal platelet counts were higher than in healthy controls with normal platelet counts (19). Further research should be conducted to clarify the source of VEGF in the circulation and the intriguing role of platelets in relation to circulating VEGF. In our study, although the information obtained from serum and plasma VEGF measurements were similar, plasma seems to reflect better the level of VEGF in the circulation, probably because VEGF measurements was performed in children during their oncological treatment. Since platelets and white cells in peripheral blood samples contribute to the concentration of VEGF in serum, serum VEGF levels probably do not reflect the actual circulating VEGF in children under chemotherapy due to decreased blood cell counts. Thus, plasma measurements of VEGF should be preferred in children during treatment for a solid tumor. However, further studies are needed in order to determine whether measurements of circulating VEGF might play a role in assessing prognosis and modulating treatment.
- Received April 16, 2012.
- Revision received June 21, 2012.
- Accepted June 22, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.