


Abstract
Background: Eribulin is a pharmaceutically and structurally optimized analog of the marine sponge natural product halichondrin B. Its salt form, eribulin mesylate (Halaven®) is clinically used in the United States, the European Union, and Japan for the treatment of heavily pretreated patients with metastatic breast cancer, who previously received an anthracycline and a taxane. Early preclinical studies of this new inhibitor of microtubule dynamics showed high antitumor potency towards several human cancer types in vitro and in vivo. Here we extend those early studies by examining the effects of eribulin against a wider spectrum of human tumor xenografts in vivo, and by directly comparing the in vivo effectiveness of different dosing administration schedules. Materials and Methods: In single-schedule studies, in vivo activity of eribulin against HT-1080 fibrosarcoma, U251 glioblastoma, SR-475 head and neck cancer, SK-LMS-1 leiomyosarcoma, NCI-H322M and NCI-H522 non-small cell lung cancer (NSCLC), PANC-1 pancreatic cancer, and NCI-H82 small cell lung cancer (SCLC) xenografts was examined at dose levels of 0.19-4.0 mg/kg using q2d×3(×3), q4d×3, q4d×4, and q7d×2 schedules. Administration schedule dependence was evaluated by directly comparing q1d×5, q2d×3(×3), q4d×3, and q7d×3 schedules in the MDA-MB-435 breast cancer xenograft model, using conditions of equivalent total dosing over the course of the experiment. Results: In single-schedule studies, maximum tolerated dose (MTD) values (or maximal ‘at or below MTD’ values) ranged from 0.8-1.7 mg/kg. In vivo antitumor responses at these dosing levels included tumor growth inhibition, stasis, and regression; several studies showing regression also yielded long-term tumor-free survivors. Effectiveness of eribulin showed model-to-model variability that appeared to be unrelated to dose level or administration schedule, suggesting that characterization of models with differing eribulin sensitivities may reveal potential biomarker strategies. Results of the dose schedule comparison study in the MDA-MB-435 model suggested the following order of effectiveness and tolerability: q2d×3(×3)>q4d×3≈q7d×3>> q1d×5. Moderately intermittent dosing thus shows optimal preclinical effectiveness, in good agreement with the approved intermittent clinical schedule for eribulin (days 1 and 8 of a 21-day cycle). Conclusion: The current results show that eribulin has broad spectrum preclinical antitumor activity against a wide variety of human cancer types, and indicate that maximum effectiveness and optimal tolerability are obtained using moderately intermittent dosing schedules.
- Eribulin
- E7389
- NSC 707389
- halichondrin B
- antimitotic
- microtubule modulators
- MDA-MB-435 breast cancer model
Eribulin (eribulin) or its mesylate salt (Halaven®, Eisai) have been variously referred to as B1939, ER-086526, E7389, or NSC 707389 (U.S. National Cancer Institute designation)) is a pharmaceutically and structurally optimized analog of the marine sponge natural product halichondrin B (1). As a first-in-class halichondrin-based cancer therapeutic (eribulin mesylate is approved in the United States for the treatment of patients with metastatic breast cancer who have previously received at least two chemotherapeutic regimens for the treatment of metastatic disease. Prior therapy should have included an anthracycline and a taxane in either the adjuvant or metastatic setting), eribulin is a novel inhibitor of microtubule dynamics, having a mode of action distinct from those of other tubulin-targeted agents (2-4). Preclinically, eribulin showed potent activity towards a variety of human cancer cell types in vitro and in vivo (1), exerting its anticancer effects by inducing irreversible mitotic blockade (5), which subsequently leads to cancer cell death via apoptosis (6).
Previous preclinical in vivo studies with eribulin have shown potent inhibition of human tumor xenograft growth, including frank regressions and cures, in human breast, colon, melanoma, and ovarian cancer xenograft models; these studies also showed that eribulin has an unusually wide therapeutic window for a cytotoxic agent (2). In this article, we extend previous in vivo studies by examining the activityof eribulin in a significantly wider spectrum of human cancer xenograft models, and by investigating the administration schedule dependence of its antitumor effects.
Materials and Methods
Test agents. Eribulin was synthesized by Eisai Inc. as described elsewhere (7), and was used in the current studies as its mesylate salt, eribulin mesylate (same salt form used in clinical formulation). Paclitaxel was obtained from Calbiochem (La Jolla, CA, USA) and InB:Hauser Pharmaceuticals Services Inc. (Denver, CO, USA). Gemcitabine, obtained as its clinical formulation Gemzar®, was from Eli Lilly (Indianapolis, IN, USA). Carmustine was obtained from Ben Venue Laboratories (Bedford, OH, USA).
Human cancer cell lines and tumor xenograft models. All studies using laboratory animals were approved by the appropriate Institutional Animal Care and Use Committees of Eisai Research Institute (Andover, MA, USA), Eisai–Tsukuba Research Laboratories (Tsukuba, Ibaraki, Japan), or the Southern Research Institute (Birmingham, AL, USA), and adhered to all applicable institutional and governmental guidelines for the humane care and use of laboratory animals.
In vivo anticancer effects of eribulin were evaluated in immunocompromised nu/nu mice using subcutaneous (s.c.) tumor xenograft models of the following human cancer types: breast cancer (MDA-MB-435), fibrosarcoma (HT-1080), glioblastoma (U251), head and neck cancer (SR-475), leiomyosarcoma (SK-LMS-1), non-small cell lung cancer (NSCLC; NCI-H322M and NCI-H522), pancreatic cancer (PANC-1), and small cell lung cancer (SCLC; NCI-H82). The HT-1080, NCI-H522, NCI-H82, PANC-1, and SK-LMS-1 cell lines were obtained from the American Type Culture Collection (ATCC; Manassas, VA, USA), while the MDA-MB-435, NCI-H322M, and U251 cell lines were from the NCI-Division of Cancer Treatment Tumor Repository (Frederick, MD, USA). The SR-475 cell line is a proprietary cell line of the Southern Research Institute; experiments using this line were performed there under contract from Eisai Inc. All cell lines were grown according to repository-recommended conditions.
At the time of the studies described in this article, MDA-MB-435 cells were considered to be of breast cancer origin. Subsequent genetic studies by several groups suggested this cell line was identical to M14 melanoma cells, prompting some researchers to conclude that MDA-MB-435 cells were actually M14 melanoma cells, not breast cancer cells. Still other studies have argued that although the two cell lines may be identical, M14 cells are actually MDA-MB-435 breast cancer cells. The history of this controversy, with references, is summarized online by the US NCI (http://dtp.nci.nih.gov/docs/misc/common_files/mda-mb-435-update.html; last accessed 22/03/2012). Since this is still an area of active controversy, in this article we refer to MDA-MB-435 as a breast cancer cell line, thereby using their accepted identity at the time our experiments were actually performed.
Subcutaneous human tumor xenografts were generated for all models except HT-1080 and SK-LMS-1 via inoculation of 5- to 8-week-old female nu/nu mice with serially passaged 30-40 mg tumor fragments using 12- or 13-gauge trocar needle insertion. For HT-1080 and SK-LMS-1 xenografts, 100 μl of 1×107 cells/ml cell suspensions in Hank's balanced salts solution (HT-1080) or Dulbecco's phosphate buffered saline (SK-LMS-1) were injected s.c. in flank areas of 5- to 8-week-old female nu/nu mice. All s.c. tumors were allowed to reach 75-200 mm3 volumes before randomization of mice into treatment groups and initiation of drug administration. All studies utilized 10 mice/group, except for the SK-LMS-1 leiomyosarcoma study, which used 6 mice/group.
Drug administration. In the HT-1080 fibrosarcoma model, eribulin mesylate was dosed by intravenous (i.v.) tail vein injection at 1.27, 1.69, 2.25, 3.0 and 4.0 mg/kg on a q4d×3 schedule, and paclitaxel was dosed i.v. at 20 mg/kg on the same schedule. In the U251 glioblastoma model, eribulin mesylate was dosed i.v. at 0.45, 0.6, and 0.8 mg/kg on a q2d×3(×3) schedule, and carmustine was dosed intraperitoneally (i.p.) at 12 mg/kg on a q4d×3 schedule. In the SR-475 head and neck cancer xenograft model, eribulin mesylate was dosed i.v. at 0.47, 0.63, 0.84, 1.1, and 1.5 mg/kg on a q2d×3(×3) schedule, and paclitaxel was dosed i.v. at 20 mg/kg on the same schedule. In the SK-LMS-1 leiomyosarcoma xenograft model, eribulin mesylate was dosed i.v. at 0.19, 0.38, 0.75 and 1.5 mg/kg on a q7d×2 schedule. In the NCI-H322M NSCLC xenograft model, eribulin mesylate was dosed i.v. at 0.2, 0.4, 0.8 and 1.6 mg/kg on a q4d×4 schedule. In the NCI-H522 NSCLC xenograft model, eribulin mesylate was dosed i.v. at 0.2, 0.4, 0.8 and 1.6 mg/kg on a q4d×4 schedule. In the PANC-1 pancreatic cancer xenograft model, eribulin mesylate was dosed i.v. at 0.4, 0.53, 0.71, 0.95, 1.27, 1.69, 2.25, 3.0, and 4.0 mg/kg on a q4d×3 schedule, and gemcitabine was dosed i.v. at 180 mg/kg on a q3d×4 schedule. In the NCI-H82 SCLC xenograft model, eribulin mesylate was dosed i.v. at 0.54, 0.71, 0.96, 1.27, and 1.70 mg/kg on a q4d×3 schedule, and paclitaxel was dosed i.v. at 20 mg/kg on a q2d×3(×3) schedule.
The MDA-MB-435 breast cancer xenograft model was used to compare dosing administration schedules under conditions of equal total dosing intensity. In this experiment, eribulin mesylate was dosed i.v. at 0.9 mg/kg and 1.8 mg/kg on a q1d×5 schedule, at 0.5 mg/kg and 1.0 mg/kg on a q2d×3(×3) schedule, and at 1.5 mg/kg and 3.0 mg/kg on both q4d×3 and q7d×3 schedules. Using this strategy, animals in the corresponding ‘low dose’ and ‘high dose’ groups received either 4.5 mg/kg or 9 mg/kg total administered eribulin mesylate, respectively.
Measurements and evaluation of results. Tumor volumes of s.c. xenografts were determined on the days indicated by caliper measurements (mm) and were calculated using the formula V=(L×W2)/2, where L and W refer to the larger and smaller dimensions, respectively. Tumor regression was defined as at least 50% reduction in the mean group tumor volume relative to that measured on the first day of drug administration. Tumor stasis was defined as responses that fell between 50% reduction and 25% increase in mean group tumor volumes relative to that measured on the first day of drug administration. Tumor growth inhibition was defined as more than 25% increase in mean group tumor volumes relative to that measured on the first day of drug administration, but smaller than that of the corresponding control group.
Summary of eribulin in vivo activity studies in human cancer xenograft models (including previously published results).
The magnitude, consistency, and clear dose/response characteristics of the in vivo effects seen within and across tumor models, together with wide separations of standard error of the mean (SEM)-based error bars, all strongly argue that the effects seen in the current studies are not simply due to chance. Accordingly, statistical analyses of the studies reported in this article were deemed unnecessary.
Body weights of mice were measured individually using a tared platform balance on the same days that tumor volume measurements were obtained. The maximum tolerated dose (MTD) was considered to be the highest dose that resulted in no more than 20% reversible body weight loss or no more than 10% lethality.
For comparative purposes, previously published results from human tumor xenograft studies performed in MDA-MB-435 breast cancer, COLO 205 colon cancer, NIH:OVCAR-3 ovarian cancer, and LOX melanoma models (1) are summarized and presented in Table I, and are reproduced there with permission from the American Association for Cancer Research.
Results
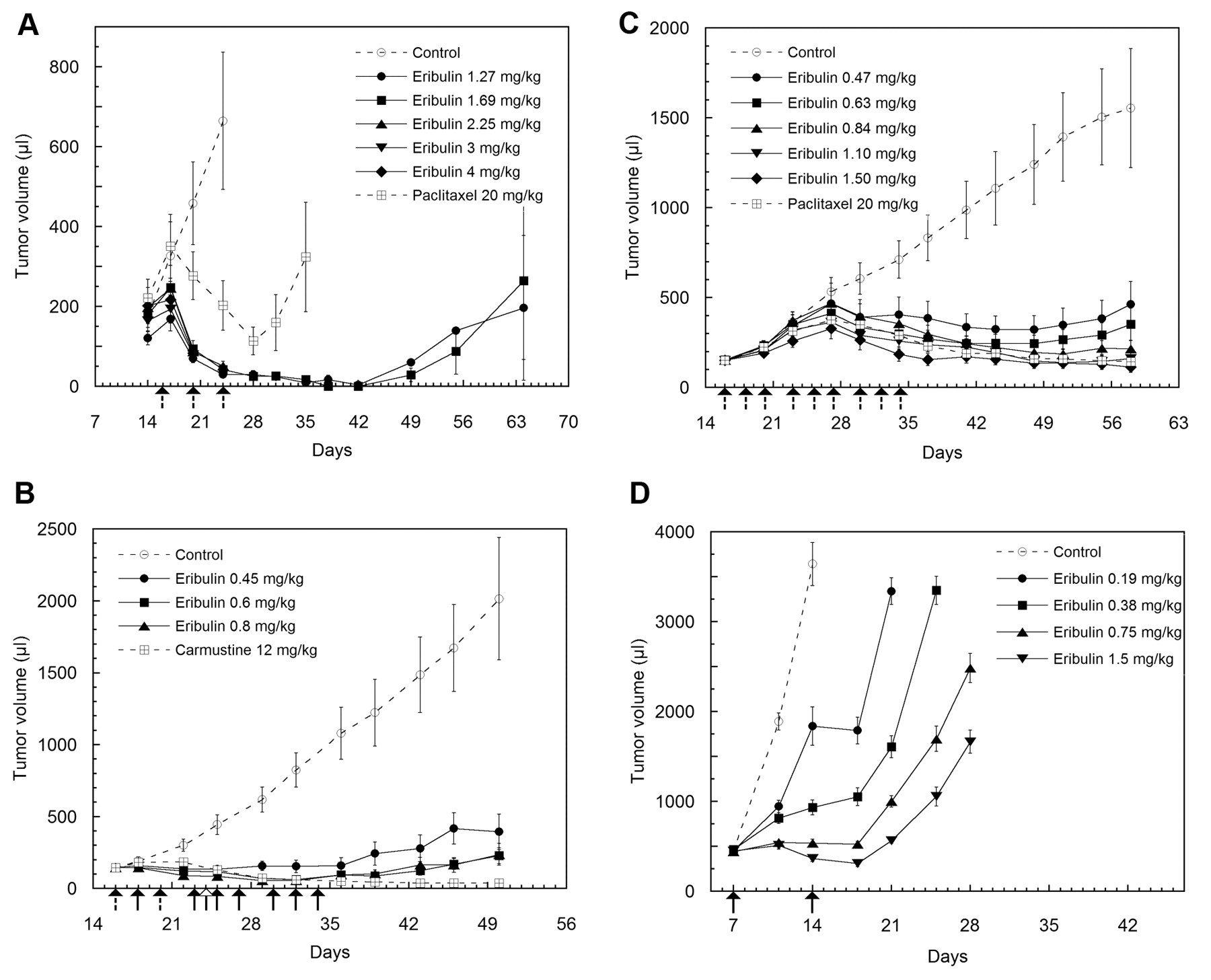
Studies using single-dosing schedules. In the present work, previous preclinical in vivo studies using eribulin in human breast, colon, melanoma, and ovarian cancer xenograft models (1; summarized in Table I) have been extended to a variety of other human xenograft types. In the s.c. HT-1080 fibrosarcoma model (Figure 1A), treatment with eribulin on a q4d×3 schedule at its MTD dose and below (1.69 mg/kg and 1.27 mg/kg, respectively) led to rapid regression of existing tumors, with all animals becoming tumor-free by day 42. Although some tumors in both groups began to recur after day 42, five mice in each group remained tumor-free up to day 64. In contrast to eribulin induced tumor regression in the 1.69 mg/kg and 1.27 mg/kg groups, treatment with positive control paclitaxel led to a maximal 49% reduction in mean tumor size (not quite meeting the 50% regression criterion), although three paclitaxel-treated mice became tumor-free by day 38 and remained so up to day 64.

Inhibition of human fibrosarcoma, glioblastoma, head and neck cancer, and leiomyosarcoma xenograft growth by eribulin. Antitumor activity of eribulin was evaluated against HT-1080 fibrosarcoma (A), U251 glioblastoma (B), SR-475 head and neck cancer (C), and SK-LMS-1 leiomyosarcoma (D) xenografts using the dosing levels indicated. Dosing days for drugs are shown witharrows below the x-axes, as follows: eribulin alone, solid arrows with solid line; positive control alone, open arrows with solid line; both eribulin and positive control, solid arrows with dotted line. Results shown represent mean±standard error of the mean (SEM) tumor volumes measured as described in the Materials and Methods.
In the s.c. U251 glioblastoma xenograft model (Figure 1B), no dose of eribulin given on a q2d×3(×3) schedule exceeded the MTD based on body weights and lethality criteria, so defining a MTD for this study is not possible. Nevertheless, treatment with the two highest doses of eribulin (0.6 and 0.8 mg/kg) resulted in tumor regression, with four and five animals in the 0.6 and 0.8 mg/kg groups, respectively, becoming and remaining tumor-free through the end of the experiment. Treatment with the lowest eribulin dose (0.45 mg/kg) generally led to tumor stasis, although three mice in this group also became and remained tumor-free through the end of the experiment. Treatment with positive control carmustine led to tumor regression; four animals in this group became tumor-free and remained so until the end of the experiment.
In the s.c. SR-475 head and neck cancer xenograft model (Figure 1C), treatment with eribulin on a q2d×3(×3) schedule at 1.1 mg/kg (MTD) and 0.84 mg/kg led to tumor stasis, and lower doses led to tumor growth inhibition relative to tumor sizes measured at the start of dosing. Interestingly, in this model, onset of antitumor effects was seen only after about two weeks of dosing. Although mean tumor sizes did not reflect regression in any group, five tumors in the 1.1 mg/kg (MTD) eribulin group regressed below volumes originally measured at the start of dosing. Treatment with positive control paclitaxel led to mean group tumor stasis relative to the start of dosing, although tumors in seven individual animals did regress below starting volumes.

Inhibition of human non-small cell lung cancer (NSCLC), pancreatic cancer, and small cell lung cancer (SCLC) xenograft growth by eribulin. Antitumor activity of eribulin was evaluated against NCI-H322M NSCLC (A), NCI-H522 NSCLC (B), PANC-1 pancreatic cancer (C), and NCI-H82 SCLC (D) xenografts using the dosing levels indicated. Dosing days for drugs are shown with arrows below the x-axes, as follows: eribulin alone, solid arrows with solid line; positive control alone, open arrows with solid line; both eribulin and positive control, solid arrows with dotted line. Results shown represent mean±SEM tumor volumes measured as described in the Materials and Methods.
In the s.c. SK-LMS-1 leiomyosarcoma xenograft model (Figure 1D), no dose of eribulin given on a q7d×2 schedule exceeded the MTD based on body weights and lethality criteria, so defining a MTD for this study is not possible. Treatment with the two highest doses of eribulin, 0.75 and 1.5 mg/kg, led to tumor stasis, with mean 19% increase and 31% decrease in tumor sizes seen on day 18, four days after final dosing. Treatment of mice with the two lowest doses of eribulin, 0.38 and 0.19 mg/kg, led to diminishing but dose-dependent levels of tumor growth inhibition.
In the s.c. NCI-H322M NSCLC xenograft model (Figure 2A), no dose of eribulin given on a q4d×4 schedule exceeded the MTD based on body weights and lethality criteria, so defining a MTD for this study is not possible. However, treatment with the highest dose of 1.6 mg/kg eribulin led to stasis of tumor growth during the administration period and for about three weeks after cessation of dosing. Treatment with 0.8 and 0.4 mg/kg eribulin led to diminishing but dose-dependent inhibition of tumor growth during and after the dosing administration period. Tumors in animals treated with 0.2 mg/kg were essentially identical in size to those seen in the control group.

Comparison of different dosing schedules in MDA-MB-435 human breast cancer xenograft model. Antitumor activity of eribulin was compared at high dose (9 mg/kg total) and low dose (4.5 mg/kg total) levels using q1d×5 (A), q2d×3(×3) (B), q4d×3 (C), and q7d×3 (D) administration schedules, with dosing days as indicated by vertical lines below the x-axes. E: Body weights for all schedules. Results shown represent mean ± SEM of tumor volumes (A-D) or body weights (E) measured as described in the Materials and Methods.
In the s.c. NCI-H522 NSCLC xenograft model (Figure 2B), no dose of eribulin given on a q4d×4 schedule exceeded the MTD based on body weights and lethality criteria, so defining a MTD for this study is not possible. Treatment with 1.6 mg/kg eribulin led to regression of tumors during the dosing period, followed by slow tumor regrowth starting about 10 days after cessation of dosing. Two animals in this group became and remained tumor-free through the end of the experiment. Administration of 0.8 mg/kg led to tumor growth stasis during the administration period, followed by regrowth of most tumors starting within one week after cessation of dosing. One animal in this group became and remained tumor-free through the end of the study. Treatment of animals with 0.4 mg/kg and 0.2 mg/kg eribulin led to lesser degrees of tumor growth inhibition in a dose-dependent manner, with one animal in the 0.4 mg/kg group becoming and remaining tumor-free through the end of the experiment.
In the s.c. PANC-1 pancreatic cancer xenograft model (Figure 2C), treatment with eribulin on a q4d×3 schedule at its MTD of 1.27 mg/kg led to reduction in size of tumors that had initially continued growing for about a week after the start of dosing. However, the minimum mean tumor size reached in this group on day 29 was still 51% larger than mean tumor sizes on the day of first dosing, indicating that eribulin at the MTD failed to meet the stasis criterion. Nevertheless, after achieving a minimum at day 29, tumor growth rates remained low for another 11 days before starting to accelerate at the end of the experiment. In contrast, while treatment with positive control gemcitabine did meet the tumor stasis criterion (22% larger tumors on day 29 relative to day of first dosing), regrowth rates in this group accelerated faster towards the end of the experiment compared to groups treated with MTD and sub-MTD of eribulin.
In the s.c. NCI-H82 SCLC xenograft model (Figure 2D), no dose of eribulin given on a q4d×3 schedule exceeded the MTD based on body weights and lethality criteria, so defining a MTD for this study is not possible. Treatment with 0.96 and 1.70 mg/kg eribulin led to tumor regression, which reached minimal values in both groups on day 34, nine days after cessation of dosing. Two and three mice in these 2 groups, respectively, became and remained tumor-free through the end of the experiment. Treatment with 0.71 and 1.27 mg/kg met tumor stasis criteria, with tumor volume minima occurring on day 34. Three and two mice in these 2 groups, respectively, became and remained tumor-free through the end of the study. Animals treated with 0.54 mg/kg eribulin exhibited tumor stasis both during the administration period and for about two weeks after dosing cessation; one mouse in this group became and remained tumor-free through the end of the experiment. Excepting tumor-free mice, tumors in all eribulin-treated groups regrew slowly, starting two to three weeks after cessation of dosing. Treatment with positive control paclitaxel led to tumor stasis during the administration period and for about 2-3 weeks after cessation of dosing. Three animals in the paclitaxel group became and remained tumor-free through the end of the study.
Comparison of different dosing schedules. Dosing schedule dependence of the in vivo anticancer activity of eribulin mesylate was assessed by comparing q1d×5, q2d×3(×3), q4d×3 and q7d×3 i.v. administration schedules in the s.c. MDA-MB-435 breast cancer xenograft model (Figure 3). In this study, each schedule was tested at two dosing levels (‘high dose’ and ‘low dose’), resulting in either 9 mg/kg or 4.5 mg/kg total delivered eribulin, respectively, during the course of the experiment. This strategy, thus, allowed direct comparison of different administration schedules at equal dosing intensity levels.
Treatment with eribulin on all four dosing schedules resulted in rapid and complete loss of previously measureable tumors. However, high-dose treatment (9 mg/kg total) resulted in 70-100% lethality on all schedules; this dose level was, thus, above the MTD for all schedules (Figure 3A-D). Low-dose treatment on the q1d×5 schedule was also above the MTD, with 50% lethality seen in this group (Figure 3A). In contrast, low-dose treatment (4.5 mg/kg total) was well-tolerated on the q2d×3(×3), q4d×3 and q7d×3 schedules (Figure 3B-D), with average maximum body weight losses in these groups of 2%, 16% and 8%, respectively (Figure 3E). Thus, based on lethality and body weight criteria, the following order of tolerability was observed: q2d×3(×3)>q7d×3>q4d×3>>q1d×5.
Marked antitumor efficacies were observed for low-dose level groups using q2d×3(×3), q4d×3 and q7d×3 schedules (Figure 3B-D). With dosing for all groups starting on day 14, previously measurable tumors were eliminated in all groups by day 31. Although tumors ultimately regrew in small numbers of mice, many animals in each group remained tumor-free through day 119. Thus, eight, seven, and seven mice each in the low-dose q2d×3(×3), q4d×3 and q7d×3 groups, respectively, were considered cured (one unrelated death (broken back) occurred on day 28 in the low dose q7d×3 group). Re-appearance of the small numbers of tumors in these groups was staggered according to dose schedule. Thus, the first of two recurring tumors in the low dose q7d×3 group was first seen on day 56, i.e. 28 days after cessation of dosing in that group (Figure 3D). In the low-dose q4d×3 group, the first of three recurring tumors was seen on day 73, i.e. 51 days after cessation of dosing in that group (Figure 3C). In the low-dose q2d×3(×3) group, the first of two recurring tumors was seen on day 92, i.e. 59 days after cessation of dosing in that group (Figure 3B). With the caveat that only small numbers of tumors recurred in any group, moderately intermittent dosing schedules appeared to produce the longest tumor-free intervals, whether based on days from initiation or cessation of dosing: q2d×3(×3)>q4d×3>q7d×3.
Discussion
The current in vivo studies with eribulin are summarized in Table I, which also includes summaries of results from previously-published preclinical studies in breast, colon, melanoma and ovarian cancer xenograft models (1). Similar to previous findings, in the current studies eribulin treatment at or below the MTD induced tumor regression in several human tumor xenograft models (HT-1080 fibrosarcoma, U251 glioblastoma, NCI-H522 NSCLC, NCI-H82 SCLC, MDA-MB-435 breast cancer) and tumor stasis in three others (SR-475 head and neck cancer, SK-LMS-1 leiomyosarcoma, NCI-H322M NSCLC). For studies where it was possible to unequivocally establish the MTD by the existence of at least one dose level above the MTD, MTD values ranged from 0.5 mg/kg on a q2d×3(×3) schedule (MDA-MB-435 schedule comparison study) to 1.69 mg/kg on a q4d×3 schedule (HT-1080 fibrosarcoma); both of these studies showed tumor regression at eribulin MTD levels, as did MTD dosing on q4d×3 and q7d×3 schedules (both 1.5 mg/kg) in the MDA-MB-435 schedule comparison study. MTD levels were also established in the SR-475 head and neck cancer (1.1 mg/kg, q2d×3(×3)) and PANC-1 pancreatic cancer (1.27 mg/kg, q4d×3) xenograft models, although these studies showed only stasis or tumor growth inhibition, respectively. MTD was not established in several cases, owing to the fact that dose levels above MTD were not reached in those experiments. In these cases, the highest dose levels used were thus considered at or below MTD; antitumor effects seen at these levels ranged from stasis (SK-LMS-1 leiomyosarcoma, 1.5 mg/kg, q7d×2; NCI-H322M NSCLC, 1.6 mg/kg, q4d×4) to regression (U251 glioblastoma, 0.8 mg/kg, q2d×3(×3); NCI-H522 NSCLC, 1.6 mg/kg, q4d×4; NCI-H82 SCLC, 1.7 mg/kg, q4d×3).
Long-term tumor-free survivors (TFS) were also observed in all of the current experiments that showed regression at or below MTD dose levels (HT-1080 fibrosarcoma, U251 glioblastoma, NCI-H522 NSCLC, NCI-H82 SCLC, MDA-MB-435 breast cancer [dose comparison study]). In contrast, TFS were not observed in any that showed only tumor stasis or tumor growth inhibition (SR-475 head and neck cancer, SK-LMS-1 leiomyosarcoma, NCI-H322M NSCLC, PANC-1 pancreatic cancer). In the current studies, the terms regression, stasis, and tumor growth inhibition are defined based on mean results from the entire treatment groups; thus, it would have been theoretically possible for TFS to emerge from groups that, on average, only showed stasis or tumor growth inhibition. The fact that this was not seen suggests that the appearance of TFS might only occur if the overall magnitude of the antitumor effect of eribulin in a given model is sufficiently potent to be defined as regressive. This observation, together with the fact that some models at the MTD demonstrated regression (HT-1080 fibrosarcoma, MDA-MB-435 breast cancer) while others at the MTD only stasis or tumor growth inhibition (SR-475 head and neck cancer, PANC-1 pancreatic cancer), suggests that both the degree of antitumor activity (i.e. regression, stasis, tumor growth inhibition) and the ability to completely eradicate tumors resulting in TFS depends on tumor-specific characteristics. Thus, our results point to the existence of preclinical model- and/or tumor-type heterogeneity with respect to eribulin sensitivity, suggesting that further studies comparing characteristics of models as a function of eribulin sensitivity might illuminate potential biomarker approaches to defining eribulin sensitivity and resistance.
Considering the variable sensitivity of different models to eribulin just noted, as well as the fact that regressions and TFS were seen in different models on a variety of schedules, a comparative study of q1d×5, q2d×3(×3), q4d×3, and q7d×3 dosing schedules was performed for the MDA-MB-435 breast cancer model under conditions of equivalent ‘low dose’ and ‘high dose’ total drug loads for all schedules. In this experiment, body weight and lethality analyses established the order of tolerability as q2d×3(×3)>q7d×3>q4d×3>>q1d×5, while the order of tumor-free intervals after cessation of dosing was q2d×3(×3)>q4d×3>q7d×3 (q1d×5 not included since both dose levels were above the MTD). Overall, these results indicate that moderately intermittent dosing schedules are optimal based on both activity and tolerability. While combining ordered lists is necessarily subjective, the results of this schedule comparison experiment suggest that the order of overall preclinical effectiveness and tolerability is q2d×3(×3)>q4d×3≈q7d×3>>q1d×5. The finding that moderately intermittent eribulin dosing schedules are optimal under preclinical conditions is in good agreement with the approved clinical dosing schedule for eribulin mesylate, which is intermittent administration on days 1 and 8 of a 21-day cycle (8, 9).
Together with a previous study (1), our current results establish eribulin as a highly effective preclinical antitumor agent for a wide range of human tumor xenograft types. Dosing schedule comparisons establish intermittent dosing as an optimal approach, an observation in good alignment with current clinical use. Variations in the magnitude of maximal antitumor effects at the MTD suggest that different tumor types may have inherently different sensitivities to eribulin; follow-up preclinical studies comparing characteristics of such tumors may thus shed light on potential biomarker strategies for clinical patient pre-selection. Thus, although eribulin mesylate is already an approved clinical agent, continued investigation of its preclinical antitumor attributes may contribute significantly to future clinical approaches for this drug.
Acknowledgements
We are grateful to Ann Gordon and Haley Bennett from Complete Medical Communications, who provided medical writing support funded by Eisai Inc.
- Received February 21, 2012.
- Revision received March 22, 2012.
- Accepted March 23, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Molecular Biomarkers of Response to Eribulin in Patients with Leiomyosarcoma
- Therapeutic Application of Diverse Marine-derived Natural Products in Cancer Therapy
- Broad-spectrum Preclinical Antitumor Activity of Eribulin (Halaven(R)): Combination with Anticancer Agents of Differing Mechanisms
- Antimitotic and Non-mitotic Effects of Eribulin Mesilate in Soft Tissue Sarcoma
- Eribulin Mesylate: Mechanism of Action of a Unique Microtubule-Targeting Agent
- Gemcitabine with Paclitaxel Therapy Against Mesocolic Leiomyosarcoma: A Case Report