


Abstract
Aim: The study aimed at the evaluation of the effects of radiotherapy on expression of metallothionein (MT) isoforms, both in the form of quantitative alterations in mRNA, and differences in expression of MTI/II proteins in rectal tumours. Materials and Methods: Material for the study originated from 21 patients with rectal cancer at stage II or III. Material for immunohistochemical studies [MTI/II, Minichromosome Maintenance Protein 3 (MCM3), Ki-67] and real-time polymerase chain reaction (PCR) (mRNA of MT1F, MT1X and MT2A) was sampled twice: during rectoscopic examination before the start of the preoperative radiotherapy (samples A) and from the post operative specimen, following radiotherapy (samples B). Results: The level of mRNA expression for each of the studied MT isoforms was higher in cancer cells subjected to irradiation. The most extensive differences were observed for the MT2A isoforms (p=0.09). No differences were disclosed between samples A and B in expression of MT I/II protein. The material sampled after radiotherapy manifested a tendency for reduced proliferative activity of the tumour cells: the decrease of MCM3 expression was significant (p=0.022), while in the case of Ki-67, the difference approached statistical significance (p=0.096). Conclusion: Application of radiotherapy to rectal adenocarcinoma cells is followed by an increase in MT mRNA expression level, affecting first of all the MT2A isoform. However, we failed to note an increased expression of MTI/II protein coded by the gene. Moreover, application of radiotherapy was followed by a decrease in expression of MCM3 protein. Our results cannot clearly confirm induction of MT after irradiation of human adenocarcinoma cells. The role of MT in radioprotection remains ambiguous.
In a significant proportion of patients with rectal carcinoma, application of radiotherapy is indispensable, frequently as a form of pre-surgical treatment. Therefore, from the clinical point of view, it is significant to identify factors with radioprotective activity.
The role of metallothionein (MT) as an antioxidative and a cytoprotective factor is generally recognized but its role in proliferation and cell differentiation still awaits clarification (1, 2). It is suggested that induction of MT represents an adaptive response to radiotherapy, in which MT may act as scavenger of free radicals, in this way alleviating the effects of radiotherapy (3).
MT and its isoforms. MT describes proteins of low molecular weight (6-7 kDa), with high content of sulphur, metals and cystein, but containing no aromatic amino acids (1). In humans, MT proteins manifest four basic isoforms, designated as MTI, II, III and IV (5). The best recognized isoforms include MTI and MTII. The proteins are encoded by genes located on chromosome 16q13 (5). Isoform MTI is encoded by genes MT1A, MT1B, MT1E, MT1F, MT1G, MT1H and MT1X, while the isoform MTII is encoded by a single gene, MT2A (6). The significance and specific function of each MT isoform is not known in detail.
Interactions between radiotherapy and MT expression. In several studies, tumours manifesting no expression of MT were noted to exhibit increased sensitivity to chemotherapeutic agents and to radiotherapy (8-12). Increased expression of MTI/II in tumour cells was found to increase their resistance to the effects of radiotherapy and chemotherapy (7). Some authors revealed that in humans, increased levels of MT were observed following application of radiotherapy or chemotherapy (14-16).
Since in many studies the relationship between MT and cell proliferation was documented, we decided to examine effects of radiotherapy on proliferation of rectal carcinoma cells and to correlate the obtained results with expression levels of selected MT isoforms (17-21). Expression of MT protein was evaluated using antibodies specific for MTI and II isoforms. For evaluation of mRNA levels we selected isoforms MT1X, - 1F and -2A, the expression of which is linked to proliferative activity of the tumour, its resistance to physical and chemical toxic agents and to progression of the tumour (7, 17, 20, 22-27). For evaluation of proliferation, Ki-67 antigen was selected, a widely applied marker of proliferation.
Another proliferation marker was also selected, minichromosome maintenance protein 3 (MCM3). This protein functions within the pre-replicative complex, which manifests activity of helicase and actively participates in the start of DNA replication (28).
The study aimed at the evaluation under clinical conditions of radiotherapy effects on the expression of MT isoforms, both in the form of quantitative changes in levels of mRNA expression, and differences in expression of MTI/II protein in rectal tumours. Changes in protein levels and in expression of mRNA for MT, as well as the proliferative activity of the carcinoma (appraised based on evaluation of Ki-67 and MCM3), were compared in preparations obtained from the tumour before and after radiotherapy.
Materials and Methods
Material for the studies originated from 21 patients suffering from rectal carcinoma, aged 47 to 80 years (mean=62 years, median=62.5 years). The group included 11 men and 10 women. In all the patients, imaging studies [computed tomography (CT) and transrectal ultrasonography (USG)] and physical examination allowed resectable rectal carcinoma at II or III stage (cTNM) to be diagnosed. The tumour was located at a depth of 3 to 12 cm from the anal verge (mean depth of 6.91 cm, median=6 cm). A team consisting of a surgeon and a radiotherapist allocated the patients to a combined treatment, consisting of preoperative radiotherapy and surgery. The radiotherapy included a dose of 25 Gy in five fractions to the rectal tumour region and the regional lymphatic drainage area. In most of the patients, the surgery was performed on the second day (between the first and the fourth day) following completion of radiotherapy and involved abdominal (AR) or abdominal-sacral (ASR) resection of the rectum, depending on the distance between the tumour and the anal verge. Special effort was made to perform the resection strictly according to the principles of the total mesorectal excision technique (TME). In the postoperative histopathological report the extent of pathological advancement was specified (pTNM) as stage I in two patients, stage II in 10 patients and stage III in nine patients.
Tumour material was sampled for immunohistochemical studies and real-time polymerase chain reaction (PCR) on two occasions: during rectoscopic examination before treatment (samples A) and from the postoperative material, following radiotherapy and resection of the rectum together with the tumour (samples B). In every case, the material sampled from tumour was divided into two parts. One part was fixed in 4% buffered formalin and subjected to further histopathological analysis [histological type of the tumour, grade of malignancy (G)] and to immunohistochemical studies while the other part, devoted to mRNA studies, was saved in RNA-Later solution (Invitrogen, Carlsbad, CA, USA) and frozen at −80°C. In a few cases, the sampled material proved to be insufficient to perform both studies and in some the obtained results were markedly different from median value. Therefore, the analysis included 17 cases examined by immunohistochemistry and 16 cases in which mRNA was estimated both before and after radiotherapy. All the patients included provided informed consent for participation in the studies and the study was approved by the Institutional Review Board.
Real-time PCR. Total RNA was isolated from tissues using RNeasy Mini Kit (Qiagen, Hilden, Germany), in line with the procedure described by the manufacturer. In order to remove genomic DNA, the samples were digested with DNaze (Qiagen). Reversible transcription reactions were performed using SuperScript III kit (Invitrogen).
Expression of mRNAs for MT isoforms MT1F, MT1X and MT2A was estimated using real-time PCR and 7900HT Fast Real-Time PCR System (Applied Biosystems, Carlsbad,CA, USA), applying primers and probes in the TaqMan system (Applied Biosystems). The results were standardized basing on expression of the reference gene β-actin. Primers and probes used in the reactions included Hs00744661_sH for MT1F, Hs00745167_sH for MT1X, Hs02379691_g1 for MT2A and Hs99999903_m1 for β-actin (Applied Biosystems). The reactions were conducted in defined conditions: activation of polymerase at 50°C for 2 min, preliminary denaturation at 94°C for 10 min, denaturation at 94°C for 15 s, annealing of primers and probes and synthesis at 60°C for 1 min, for 40 cycles.
Expressions of mRNAs for the examined isoforms of MT were appraised estimating the relative quantity (RQ) of mRNA using the ΔΔCt method.
Normal large intestinal mucosa as a calibrator was obtained from patients with a single focus of rectal carcinoma, not treated earlier by radiotherapy or chemotherapy, and isolated from unchanged proximal margin of resection, distant from the primary rectal tumour by at least 20 cm.
Immunohistochemistry (IHC). The tumour samples were fixed in 4% buffered formalin, dehydrated and embedded in paraffin blocks. All immunohistochemical reactions were conducted on paraffin sections. For the estimation of MTI/II, MCM3 and Ki-67 antigen expressions, mouse monoclonal antibodies were used (clone E-9, code M0639, dilution 1:100; clone 101, code M7263, dilution 1:50; and clone MIB-1, code M7240, dilution 1:50 respectively, all Dako, Glostrup, Denmark). All the reactions were accompanied by negative controls in which specific antibodies were substituted by the Primary Negative Control Kit (Dako). The studied paraffin sections were boiled in the Antigen Retrieval Solution in a microwave oven to unblock antigenic determinants for Ki-67 and MCM3. The investigated antigens were visualized using biotinylated antibodies, streptavidin-biotinylated peroxidase complex (LSAB2 kit, Dako) and diaminobenzidine (DAB) (Dako).
Grade of histological malignancy of the tumour in samples obtained before (A) and after (B) radiotherapy.
Scoring of immunostaining results. The expression of MTI/II was graded using the semi-quantitative scale of the immunoreactive score (IRS), scoring the percentage of reactive cells (no staining =0, <10% = 1, 10-50% =2, 51-80% =3, >80% = 4) and the intensity (no staining=0, weak=1, intermediate=2, strong=3) of the colour reaction, with the final result being the product of both variables (29). Consequently, nine possible scores (0, 1, 2, 3, 4, 6, 8, 9 and 12) were obtained.
MCM3 and Ki-67 expression were evaluated taking into account the percentage of cells with expression (percentage on a five-grade scale of 0% scored as 0; 1-10% scored as 1 point; 11-50% scored as 2 points; 51-80% scored as 3 points; >80% scored as 4 points).
Statistics. Statistical analysis was performed using STATISTICA software, version 9 (StatSoft, Krakow, Poland). Analysis was performed on the data pertaining to the relative quantity mRNA of MT1F, -1X and -2A isoforms, cytoplasmic MT expression, proportion of cells manifesting nuclear MT expression, proportion of cells manifesting nuclear MCM3 and Ki-67 expression, degree of histological malignancy (G), gender, age, and pathological stage of cancer (pTNM). The association of all markers with clinical and pathological parameters was evaluated using the t-test for related variables, Wilcoxon test and Spearman correlation test. The level of significance was set at p<0.05.
Results
Histology. In all the patients, adenocarcinoma was diagnosed, in most of the cases demonstrating G2 grade of histological malignancy (Table I). Application of radiotherapy to rectal adenocarcinoma cells was not followed by a reduction of histological malignancy grade of rectal cancer in our material.
Immunohistochemistry. On IHC examination expression of MTI/II (Figure 1) did not exceed 4 IRS, neither in the material sampled before radiotherapy (samples A) nor that following it (samples B). No significant differences were found in expression of MTI/II protein between samples A and B (Table II).
Intensity of expression (immunohistochemical method) of metallothionein (MTI/II), Ki-67 and minichromosome maintenance protein 3 (MCM3) in carcinoma cells, A, -before, and B, -after radiotherapy.
Expression of Ki-67 antigen (Figure 2) was higher in the material sampled before radiotherapy, but the difference was not statistical significant (p=0.096; Table II).
In the case of MCM3 determinations (Figure 3), application of radiotherapy was associated with a significant (p=0.022) decrease in the proportion of cells manifesting expression of the protein (Table II). Moreover, a significant strongly positive correlation was detected between levels of Ki-67 and MCM3 in the material sampled before radiotherapy (in samples A) in the group of 21 patients (r=0.77; p<0.0001) and in the material sampled following radiotherapy (samples B) in the group of 17 patients (r=0.77; p<0.0001).
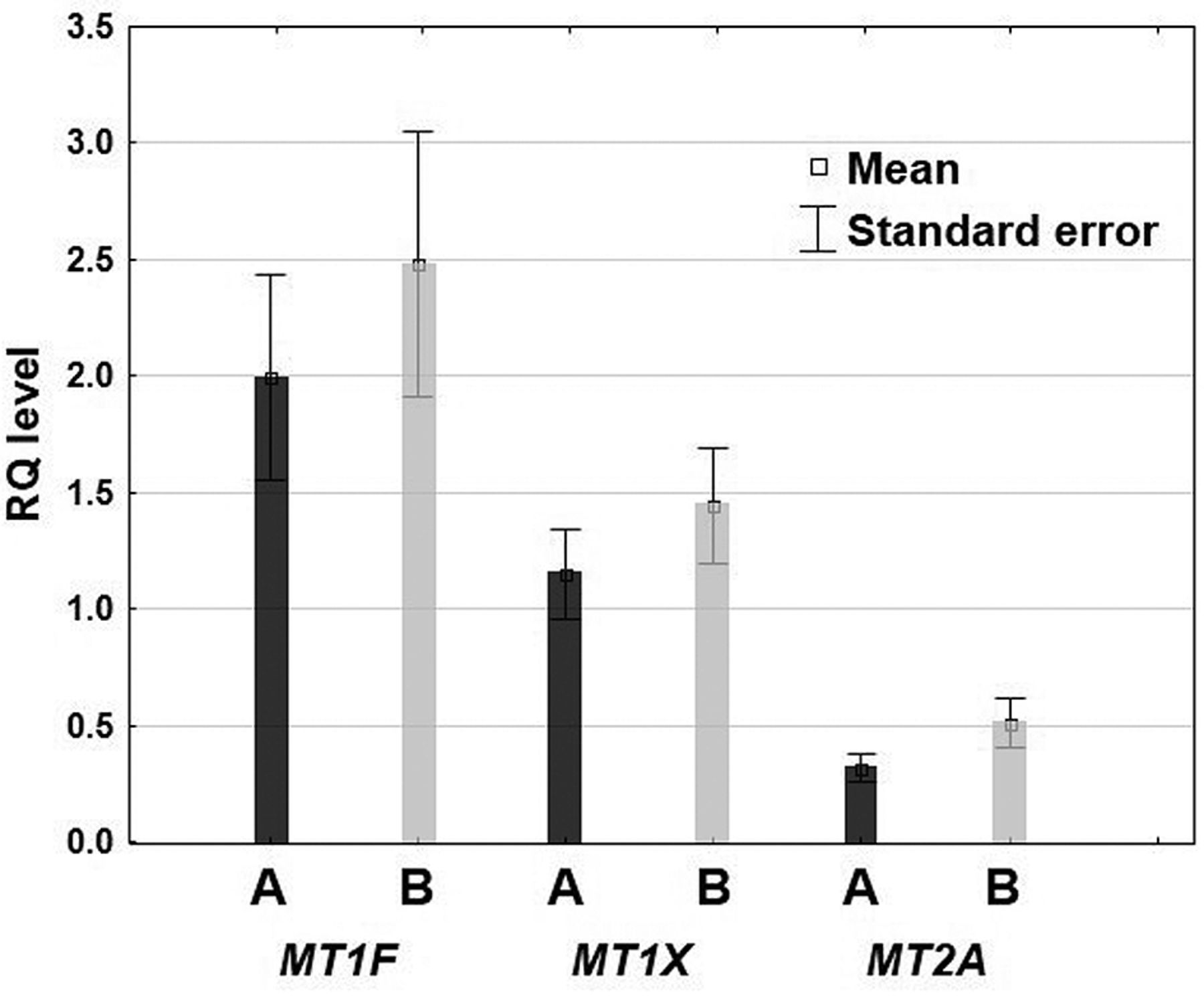
Real-time PCR. The RQ value was the highest (both in A and B samples) for the MT1F isoform, and lowest for the MT2A isoform (Table III; Figure 4). The level of mRNA expression for MT isoforms was found to be higher in carcinoma cells subjected to irradiation (Figure 4). The most extensive difference between mRNA expression in carcinoma cells sampled before radiotherapy (samples A) and those sampled after radiotherapy (samples B) was noted for the MT2A isoform but the difference was not statistically significant (p=0.09).
There was no signicant correlation between analysed markers and clinicopathological factors (age, gender, pTNM, G).
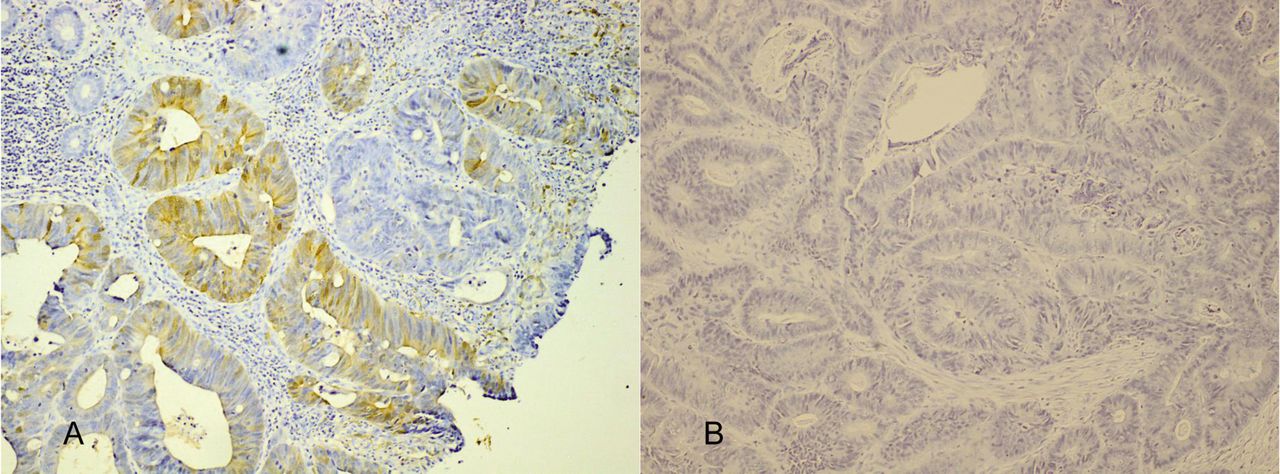
Immunohistochemical expression of metallothionein (MT) I/II protein in rectal cancer tissue in the material sampled before radiotherapy (sample A) and following it (sample B) from the same patient (no. 12). Original magnification, ×100.
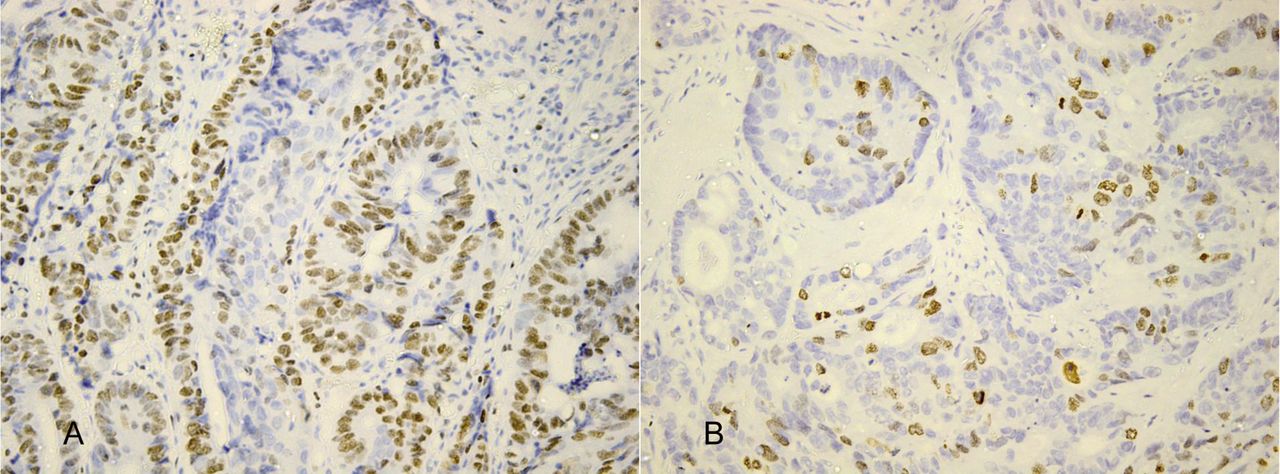
Immunohistochemical expression of Ki-67 antigen in rectal cancer tissue in the material sampled before radiotherapy (sample A) and following it (sample B) from the same patient (no. 9). Original magnification, ×200.

Immunohistochemical expression of minichromosome maintenance protein 3 (MCM3) in rectal cancer tissue in the material sampled before radiotherapy (sample A) and following it (sample B) from the same patient (no. 9). Original magnification, ×100.
Relative quantity (RQ) of mRNA for the studied metallothionein (MT) isoforms (1F, 1X, 2A) in carcinoma cells before (A) and after radiotherapy (B).
Discussion
We detected no correlation between the level of MTI/II examined by IHC and expression of mRNAs for the MT1X, -1F and -2A isoforms. The absence of correlation between MTI/II and MT mRNA levels was described previously and probably reflects regulation of MT protein level by a post-transcriptional mechanism (8).
In the studied group of patients, no difference was detected between MTI/II expression estimated by IHC in the material obtained before radiotherapy (samples A) and in the material obtained following radiotherapy (samples B). The result is consistent with that obtained by Bouzourene et al., who were the only others to evaluate the effect of radiotherapy on MT level in patients with rectal carcinoma to our knowledge (4).
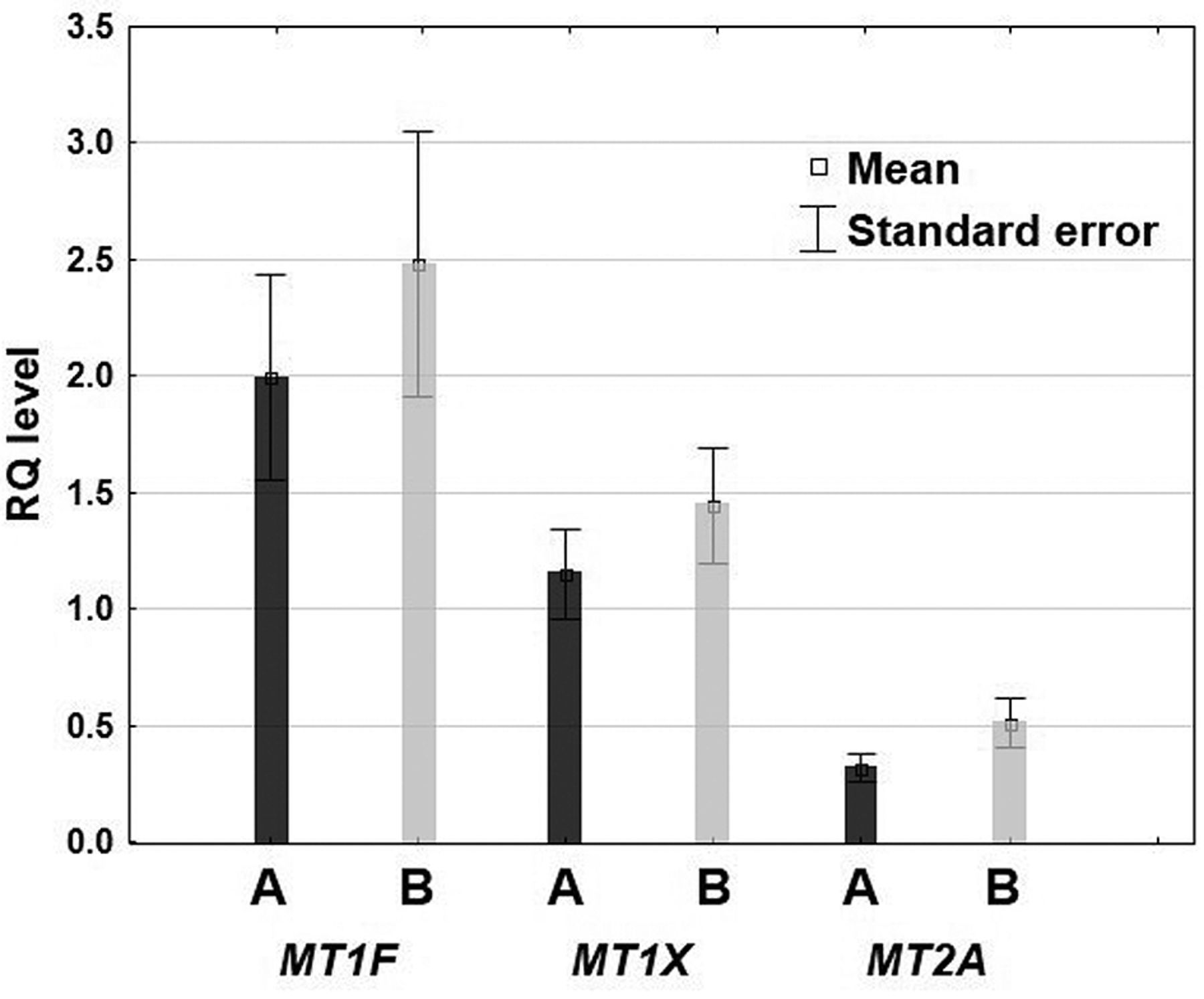
Analysis of real-time PCR results showed that tissue material sampled after radiotherapy manifested higher expression of mRNA for MT isoforms 1F, 1X and 2A than that in the material sampled before the treatment. The most extensive difference was found for the isoform 2A and the difference approached statistical significance. The result indicates that under clinical conditions, exposure of carcinoma cells to a therapeutic dose of fractionated ionizing radiation is followed by an increased activity of MT genes and an increased expression of mRNAs for MT isoforms 1X, 1F and, in particular, 2A. The observations corroborate results of several earlier studies performed in vitro on cell lines or animal models, confirming induction of MT synthesis in response to oxidative stress, including that induced by ionizing radiation (3, 13-16).
However, the results of this study indicate that radiotherapy in humans is accompanied by an increase in mRNAs, particularly for the MT2A isoform, in cancer cells. MTI/II expression remains unchanged. These contradictory results cannot unequivocally confirm induction of MT after irradiation of human adenocarcinoma cells.
Relative quantity (RQ) level of mRNAs for the studied metallothionein (MT) isoforms (1F, 1X, 2A) in adenocarcinoma cells before (A) and after radiotherapy (B).
In this study, we noted a significant decrease in expression of MCM3 protein following radiotherapy. We also demonstrated borderline statistical significance of a decrease in expression of Ki-67 antigen in cancer cells subjected to radiotherapy. The decrease in expression of proliferation markers was not accompanied by a decrease in expression of mRNAs for MT and MTI/II, which would be expected considering the hypothetical relationship between MT and cell proliferation.
No correlation was found between MT, evaluated either at the level of mRNA or protein and the proliferation markers, Ki-67 and MCM3. Correlation between MT level and proliferation markers, such as Ki-67 was examined in the past on several occasions but the results have frequently been contradictory (8, 17-19, 21, 31). In our earlier reports, we detected no correlation between MT and Ki-67 or MCM2 in oral squamocellular carcinoma (21). Some experimental studies also point to a relationship between MT and cell proliferative activity and tumour growth. Particular attention was paid to the 2A isoform of MT, demonstrating in an example of breast carcinoma cell line that a decreased amount of MT2A results in a cessation of growth in the studied cell line and a block of the cell cycle at the G-1 phase (17, 20).
The results of this study indicated a decrease in cell proliferation in response to radiotherapy, in line with the results of most published studies on this topic (32-34). It should be stressed that in the case of MCM3 protein, the decrease in expression was significant, but in the case of Ki-67, the decrease in expression only approached statistical significance. The result indicates that MCM3 may represent a potentially better proliferation marker than Ki-67. In parallel to experiments confirming involvement of MCM3 in cell proliferation, studies were published which demonstrated participation of MCM3 in blocking the cell cycle at the G-1 phase following exposure to radiotherapy (35, 36). This reflected double-strand breaks in DNA, which induced phosphorylation of MCM3 protein and probably lead to a block in the replication fork, which can cause even on-going DNA replication and the entire cell cycle to be stopped (35, 36). The decrease in MCM3 expression detected by us following radiotherapy unequivocally indicates inhibition of proliferative activity in rectal carcinoma cells.
Conclusion
Summing up our findings, the notion seems justified that application of radiotherapy to rectal adenocarcinoma cells is followed by an increase in expression of mRNAs for MT and, mainly the MT2A isoform. However, we failed to note an increased expression of MTI/II protein encoded by the gene. Moreover, application of radiotherapy was followed by a decrease in expression of MCM3 protein. Our results cannot clearly confirm induction of MT after irradiation of human adenocarcinoma cells. The role of MT in radioprotection remains ambiguous.
Interpreting our results, one should bear in mind the limitations of the study (the relatively low number of analyzed samples) but also the favourable elements, including selection of material (tumour samples were taken from the same patients before and after irradiation), as well as parallel estimations of mRNA and protein products. Further studies of the type, conducted on more numerous groups of patients may, hopefully, lead to a better understanding of the role of MT in oncologic therapy, and radiotherapy in particular.
Acknowledgements
This study was financed by grant no. 1510 (Wroclaw Medical University).
Footnotes
-
This article is freely accessible online.
-
Conflicts of Interest
The Authors declare that they have no conflict of interests.
- Received October 1, 2012.
- Revision received October 29, 2012.
- Accepted October 30, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.