


Abstract
Background: There is a clear correlation between proliferative activity and the biological behavior of cancer, which might have an impact on the patients' prognosis and consequences for the individual therapy concept. REPP86 (restrictedly expressed proliferation-associated protein 86) is a proliferation-associated protein expressed in S-, G(2)- and M-phases of the cell cycle, regarded as a promising proliferation marker and has not yet been examined in squamous cell carcinoma of the larynx (SCCL). Materials and Methods: REPP86 was analyzed retrospectively in 104 SCCL using the monoclonal antibody Ki-S2. Proliferative activity was correlated with tumor stage, histopathological grading, patients' survival and the results we recently published on Ki-67 staining in SCCL. Median follow-up time was 47 months. Results: A significant correlation (p<0.05) between histopathological grading, N-status and proliferation activity was observed. The patient group consisting of low proliferating laryngeal cancer showed a statistically longer absolute (p<0.05) and relapse-free (p=0.001) 5-year survival time than the group with a high proliferating tumor. Compared to the Ki-67 staining results, the REPP86 antibody better predicts the relapse-free 5-year-survival. Conclusion: Our results indicate that REPP86 staining of SCCL with Ki-S2 is a helpful prognostic indicator for SCCL and better predicts the relapse-free survival than Ki-67 staining in SCCL.
Head and neck malignancies account for approximately 4% of all malignancies, being mainly squamous cell carcinomas. In Europe, an estimated 63,000 patients with head and neck cancer die every year (1). Squamous cell carcinoma of the larynx (SCCL) (40,400 new cases and 21,100 deaths) predominantly occurs in men, in whom it comprises 2.1% of cases and 2.0% of deaths. The sex ratio (almost 10:1) is greater than for any other site; SCCL is a rare cancer in women, particularly in developed countries. Prognosis of patients with advanced tumor stages is not satisfactory (2) and has not improved during the last decades despite progress in therapy (3). Five-year survival rates are described as being between 52% and 94% of cases depending on tumor site, stage and tumor therapy (1, 4, 5). Often a varying clinical course under the same therapy regime is observed in patients with carcinoma of the upper aerodigestive tract with a comparable tumor staging (6, 7).
Regarding the patients' prognosis, the question arises whether there is a correlation between the biological behaviour of the tumor and any tumor biological parameter that may help the clinician to make therapeutical decisions (8). Anatomical localization of the primary tumor and tumor stage according to the TNM classification are known prognostic factors for survival and prognosis in laryngeal cancer patients (9), whereas histopathological grading is only valid with restrictions as it is not standardized and is regarded as a subjective marker (10, 11). During the past few years, there has been much progress in the development of proliferation associated antibodies and it has been shown that there is a clear correlation between proliferation activity and the biological behaviour of cancer, which might have impact on the patients' prognosis and consequences for the individual therapy concept (12-15).
In 1997, a newly developed monoclonal antibody, designated Ki-S2, was described, which recognizes the nuclear protein REPP86 (restrictedly expressed proliferation-associated protein; formerly termed p100) (16). This protein is encoded by a gene located on chromosome 20q11.2 (17). REPP86 is expressed in the cell cycle phases S/G2/M, but not in G1. During S and G2 phase, REPP86 is diffusely distributed throughout the nucleus, whereas in mitotic cells, it is strictly associated with the mitotic spindle. Immediately after completion of cytokinesis, REPP86 is rapidly degraded (16). Thus, it has now become possible to more accurately detect the fraction of proliferating tumor cells (18). Since we recently published a study about Ki-67 staining using the monoclonal antibody Ki-S11 in SCCL (12) which afforded good results for Ki-67 as a prognostic indicator, we tested a second antibody to assess the value of REPP86 as a prognostic marker. To this end, we compared both antibodies and determined the correlation between the proliferation activity of SCCL and the clinical course as well as further clinical parameters of the investigated patients.
Materials and Methods
Patients. Tumor specimens of 104 patients with SCCL were investigated. The diagnosis of squamous cell carcinomas was confirmed at the Department of Pathology and Pathological Anatomy, Christian Albrechts University of Kiel. The gender ratio of 89 men to 15 women demonstrated the well-known male predominance in cases of SCCL. The patients' age at time of initial diagnosis ranged from 37 to 87 years, with a mean age of 62.4 years. Patients were treated between 1991 and 1998 at the Department of Otorhinolaryngology, Head and Neck Surgery, Christian Albrechts University of Kiel, Germany by primary surgery and, in most cases, with postoperative irradiation (n=67).
Four patients (3.8%) presented with a T1 tumor, 29 with a T2 tumor (27.9%), 32 patients (30.8%) with a T3 tumor, and 39 patients had a T4 tumor (37.5%). The tumors were classified as supraglottic in 44 (42.3%) cases, as glottic in 54 cases (51.9%), and as subglottic in 6 cases (5.8%). Histopathological grading resulted in only 3 (2.9%) well-differentiated (G1) tumors, 76 (73.1%) moderately differentiated (G2) tumors, and 25 (24.0%) tumors with a low differentiation (G3). Seventy-five patients (72.1%) did not have clinically evident cervical lymph node metastasis, whereas 8 patients (7.7%) suffered from metastases in one (N1), and 21 patients (20.2%) in more than one (N2) cervical lymph nodes. Only 2 patients (1.9%) showed distant metastasis at the time of first diagnosis.
Antibodies. Primary SCCL sections were reacted with the monoclonal antibody Ki-S2 which was developed at the Department of Hematopathology, University of Kiel, Germany (16). Ki-S2 is a monoclonal mouse anti-human antibody that detects the proliferation-associated nuclear antigen with a molecular mass of about 100 kDa. This antigen, p100, is specifically recognized by a mouse IgG1 MoAb, designated Ki-S2 (18).
Immunohistochemistry. Four-μm-thin sections from formalin-fixed, paraffin-embedded tissue samples were routinely deparaffinized and rehydrated. Endogenous peroxidase activity was blocked by incubation with 3% hydrogen peroxide in 97% methanol for 15 minutes. For antigen demasking slides were heated in a microwave oven in a 0.01 M citrate buffer at pH 6.0 for 4 minutes and 45 seconds at 750 W. After cooling in Tris-buffer, slides were incubated with the primary antibody Ki-S2 for 60 minutes. Immunoreaction was enhanced by means of the avidin biotin complex technique (19) using biotinylated rabbit anti-mouse antibody (E0354, Dako, Hamburg, Germany), an avidin-biotin complex (E377, Strept AB Complex/HRP; Dako, Hamburg, Germany) and diaminobenzidine as a chromogen (DAB; Sigma, Deisenhofen, Germany). The sections were counterstained with Meyer's hematoxylin (Merck, Darmstadt, Germany) (Figure 1). Tissue of a human tonsil was included in every staining procedure as a positive control. Negative controls were obtained by replacing the primary antibody by buffer to exclude non-specific reactions.
Microscopical evaluation. Evaluation and photo-documentation was performed with a regular microscope (Axioplan, Zeiss, Germany). Tissue sections were evaluated by two independent investigators without knowledge of the clinical data. In areas with intense staining reaction five view fields were evaluated with 400-fold magnification. In each field, 100 cells and the number of proliferating cells were counted. The number of positive cells as a percentage of all counted tumor cells was defined as proliferative activity index. Only clear nuclear staining was considered as positive. Nuclear staining of proliferating stromal cells was considered as false positive. In doubtful cases, staining was repeated.
Statistical analysis. For statistical analysis, SPSS PC+3.0 (Statistical Package for the Social Sciences, SPSS Inc., Chicago, IL, USA) and CSS:Statistica (StatSoft™ Inc., Tulsa, USA) were used. Survival curves were generated by Kaplan-Meyer analysis. Cause-specific survival was defined as the time elapsed between first tumor diagnosis and tumor related death. Differences in survival over time were checked by log-rank test and Gehans Wilcoxon test (20). All SCCL were divided into two groups. The borderline between low- and highly proliferating tumors was set at 25% of proliferating cells as cut-off point, because this represents the median of the proliferation index. Only tumor-related deaths were regarded as uncensored observations.
Results
Proliferative activity. The percentage of proliferating cells was between 7% and 58% with a mean of 26.95% (+/-11.2%) and a median of 25%. The cut-off value between highly and low proliferating tumors was set at 25% of REPP86-positive cells. There were 49 (47,1%) low- and 55 (52,9%) highly-proliferating SCCL.
Proliferation activity and TNM classification. The proliferation activity indicated by REPP86 expression varied depending on the size of the tumor and amounted to 21.25% (±6.34%) for T1 tumors (n=4), 24.07% (±9.65%) for T2 tumors (n=29), 27.48% (±12.24%) for tumors of T3 category (n=32), and 29.26% (±11.47%) for T4 tumors (n=39). Although an increasing proliferative activity was clearly shown with a concomitant increasing T category, the results, however, were not statistically significant (p=0.1). On the other hand, correlating the proliferation activity with the nodal status demonstrated statistical significance (p=0.001). Patients (n=75) without nodal metastasis (N0) had a proliferative activity with an arithmetic mean of 23.95% (±9.04%). Patients (n=8) with N1 status showed a proliferative activity of 29.50% (±16.32%) on average, and those with N2 status (n=21) an arithmetic mean of 37.2% (±10.42%). Figure 2 illustrates the correlation of the proliferative activity with the nodal status. Furthermore, a clear difference in the average proliferative activity between M0 and M1 patients was observed. The correlation of proliferative activity and distant metastasis was statistically significant (p<0.05). The proliferation activity for the M0 stage (n=102) was 26.54%, and for the M1 stage (n=2) 47.5%.

Immunohistochemical staining of the nuclear REPP86 antigen by Ki-S2 antibody. Arrows indicate strong nuclear staining. (magnification ×200).
Proliferation activity and grading. A strong correlation between proliferative activity and histopathological grading was evident. According to the grading the mean proliferation index was as follows: 9.33% (±2.52%) for G1 (n=3), 23.91% (±8.34%) for G2 (n=76) and 40.2% (±10.9%) for G3 (n=25). All these correlations were statistically significant (p=0.001). Figure 3 illustrates the correlation of the proliferation activity with the grading.
Proliferation activity and survival. The overall five-year survival rate of all examined patients suffering from SCCL (n=104) was 49% and therefore somewhat lower than expected for a comparable study group. There were significant differences between the two distinct groups of tumors (p<0.05): patients with tumors demonstrating low proliferating activity in their carcinomas had a five-year survival rate of 95.83%, whereas patients with a highly proliferating carcinoma had a five-year survival rate of only 23.27% (p<0.05) (Figure 4). Regarding the relapse-free survival, a statistically significant difference was also observed for the five-year survival rate between the patient groups with low and highly proliferating tumors (p=0.001). Patients with a low proliferating carcinoma had a 5-year survival-rate of 87.5% in contrast to those with a highly proliferating carcinoma showing a 5-year survival rate of 42.73 % (Figure 5).
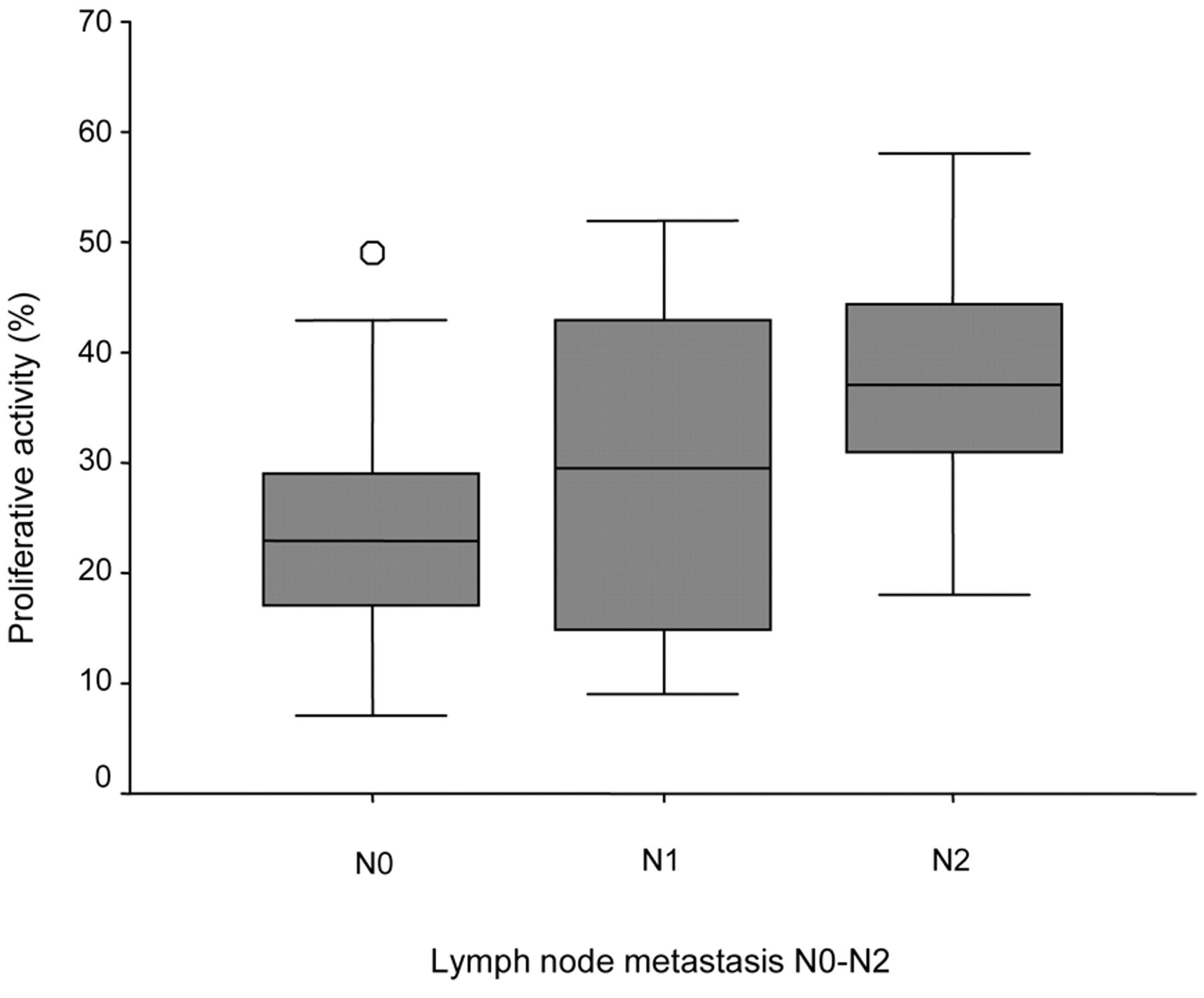
Percentage proliferation activity in different N categories of primary laryngeal carcinoma is shown (n=104). The arithmetic mean of the proliferative activity increases with the N status.

Graphical illustration showing significant correlation between REPP86 proliferation activity and grading in primary larynx carcinoma (n=104). The higher the proliferative activity, the higher the grading of the laryngeal carcinoma.
Comparison between Ki-S2 and Ki-S11 staining. Compared to the Ki-S11 antibody, the Ki-S2 antibody revealed a lower percentage of proliferating cells with a mean of 26.95% (±11.2%) and a median of 25%. The proliferative activity of both antibodies compared to the TNM classification showed similar results: An increasing proliferating activity with increasing T category for both antibodies, statistically significant (p=0.001) increase of the proliferative activity with increasing N status for both antibodies and a correlation between proliferative activity and distant metastasis, which was only statistically significant for Ki-S2 antibody but not for Ki-S11 antibody. Furthermore a strong correlation (p=0.001) between proliferative activity and histopathological grading was shown for both antibodies. Additionally, both antibodies showed similar results regarding the proliferative activity and the overall five-year survival rate (p<0.05 respectively), but regarding the relapse-free survival, the Ki-S2 antibody had a better predictive value, with p=0.001 compared to the Ki-S11 antibody (p<0.05).
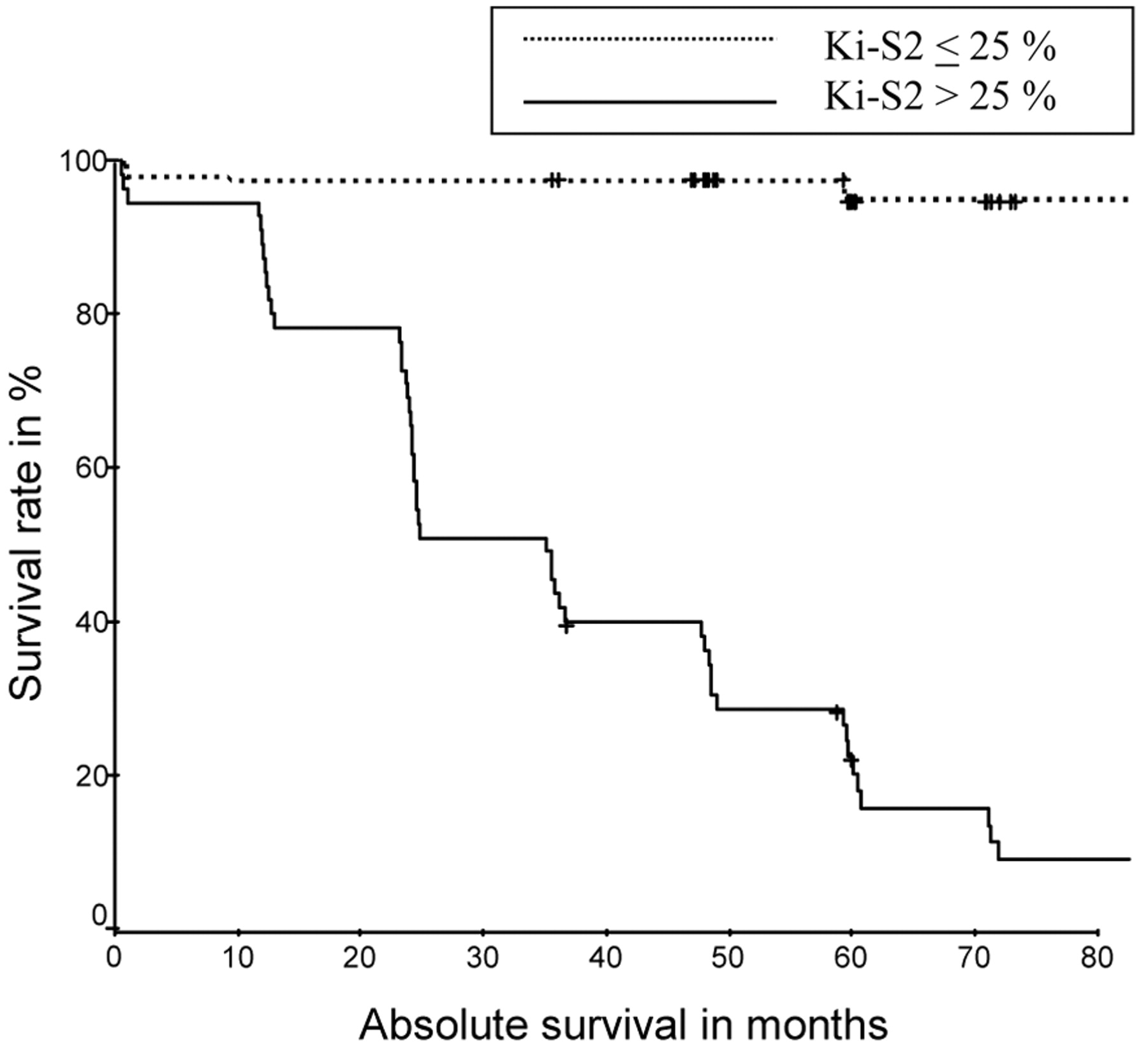
Significant difference (p<0.05) of the absolute survival rate according to Kaplan-Meyer analysis of 104 patients with SCCL, divided into low (<25%) and high (>25%) proliferative activity of tumors.
Discussion
The state of the art treatment for SCCL is the surgical or laser-surgical resection and/or adjuvant (chemo-) irradiation (21, 22). Despite these appropriate treatment strategies, the five-year survival rates 49% as shown in this study for all tumor stages is disappointing and prognosis has improved little in the past 30 years (23). A five-year survival rate of 52%-97% is described in literature, depending on tumor stage and tumor therapy (4, 24). The even worse five-year survival in our SCCL patient group is explained by the predominance of rather advanced tumor stages (71/104 (68%) of patients presented with T3 and T4 tumors).
The prognostic indicators currently in common use are tumor size, lymph node invasion, and histopathological grading (25). Nevertheless it is still difficult to give an exact prognosis for the clinical course of SCCL with the established clinical parameters (6, 11). Moreover, these known parameters even show inhomogeneous results for head and neck cancer (26). Criteria for the histopathological grading are not standardized and therefore exact classification into a distinct group of differentiation is difficult (10). This is one of the reasons why histological differentiation in head and neck carcinoma has only low evidentiary value (26).
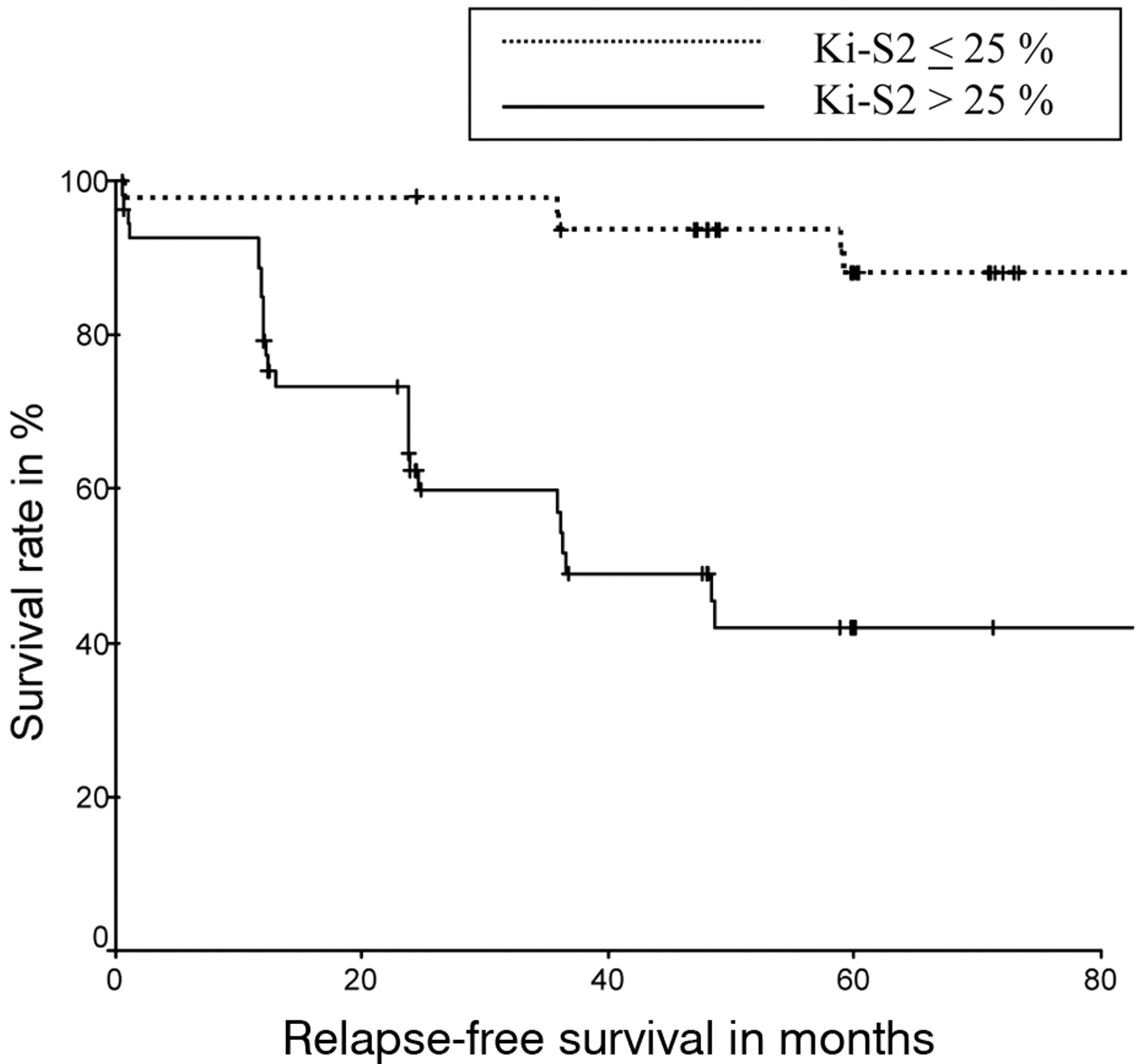
Significant difference (p=0.001) of the relapse-free-survival rate according to Kaplan-Meyer analysis of 104 patients with SCCL, divided into low (<25%) and high (>25%) proliferative activity of tumors.
The absence of reliable prognostic parameters indicating the prognosis of the patients may be due to the heterogenic appearance of a variety of different head and neck carcinomas which are often investigated as a homogeneous group of cases. Berrino and Gatta (27) proposed a separate investigation of the different cancer entities according to their anatomical origin. Therefore, in this study 104 patients with SCCL only were analyzed to rule out this particular bias.
An important sign for malignant transformation is the deregulation of the cell cycle as indicated by a large number and a high proliferative rate of dividing cells. It has been shown that a high proliferative rate of the tumor cells correlates with aggressiveness, unsatisfactory clinical course and tendency to metastasize early (6). Many authors have reported that an abnormal proliferative activity of tumor tissue can predict the biological behavior of the tumors (12, 28, 29). This indicates that proliferative activity of tumors might be an important factor for prognosis and, therefore, proliferation markers may help to determine patients` survival (6, 12) and may influence therapy indications.
Immunohistochemical proliferation indices, although reported to be of relevance, have not become established prognostic indicators yet. Several basic approaches to determine the proliferation activity of tumor tissues have been achieved, such as the determination of the cell fraction in S-phase (30) by flow cytometry, determination of 3H-thymidine index, or by histone H3 mRNA in-situ hybridization (31). Further methods to measure proliferative activity are the determination of the mitotic index, the AgNOR method, and automatic microscopical picture analysis (30, 32, 33). In contrast to other tumor entities, data on the expression of proliferation markers have yielded ambiguous results in head and neck SCC (34, 35).
The most common immunohistochemical marker used to study cell proliferation is the Ki-67 antigen, which describes the global growth fraction, defined as the cell population in G1-, S-, G2-, and M-phases of the cell cycle (36). In contrast to Ki-67, REPP86 is exclusively expressed from the transition G1/S until the end of cytokinesis. REPP86 was described as p100 protein by Heidebrecht in 1997 (16). It is a protein of about 100 kDa apparent molecular mass encoded by a gene located on human chromosome band 20q11.2 (16, 17). Its expression is tightly cell cycle regulated as demonstrated by fluorescence-activated cell sorting (FACS) analysis, becoming detectable at the G1-S transit and vanishing at the completion of cytokinesis. During S and G2 phase, repp86 is diffusely distributed throughout the cell nucleus, whereas in mitotic cells, REPP86 is strictly associated with the mitotic spindle (18).
Rudolph et al. compared the positivity for the Ki-67 antigen with the positivity for p100 in normal and pathological tissue (37) in 1998. In normal human tissues, Ki-S2 immunolabeling hardly ever exceeded 40% of the Ki-67 positive cell fraction. Immunoreactive scores of the two antibodies exhibited a linear correlation, but statistically significant differences in the ratio of Ki-S2-positive to Ki-67-positive cells were nevertheless observed between different tissue types. In contrast, the ratio of Ki-S2 and Ki-67 immunoreactive scores varied widely in neoplastic cells and tissues, occasionally attaining a ratio of almost 1:1. The authors concluded that loss of growth regulatory mechanisms in malignant cells might result in an extreme reduction of the G1 phase fraction, which is seen as the major source of uncertainty in estimations of the growth fraction, and thus in a significantly shorter doubling time. Therefore, antibody Ki-S2 should allow a more precise evaluation of the cell fraction that will complete a division cycle and a more confident appraisal of the malignancy potential of a neoplastic process.
In the present study, the percentage of proliferating cells was between 7% and 58% with a mean of 26.95% (±11.2%). Compared to our previous Ki-67 study only 45.6% of the Ki-67 positive cells were stained with the Ki-S2 antibody. This result is in accordance with the remarks given above. Over several years the proliferative activity has been evaluated with REPP86 antibodies in a variety of tumors and correlated to clinical parameters. In 1999, Rudolph et al. (38) studied 371 Swedish women with lymph node-negative breast cancer. In this multivariate analysis, the Ki-S2 labeling index (percentage of antibody-stained tumor cell nuclei) emerged as the most statistically significant predictor of overall survival, disease-specific survival, and disease-free survival (all two-sided p<0.0001). In 2003, Krams et al. (39) investigated the REPP86 expression and outcome in patients with neuroblastoma. They noted that the REPP86 labeling index emerged as the most important predictor of survival. In a study from Schrader et al. (40) REPP86 expression turned out an as important prognostic factor in mantle cell lymphoma. Mohsenifar et al. (41) showed a statistical significant difference in the REPP86 labeling index of lymph node positive breast cancer patients compared to controls in 2007. In 2008, Taheri et al. (42) discovered REPP86 in combination with Ki-67 to be useful markers to distinguish between malignant mesothelioma and benign reactive mesothelial hyperplasia.
For the field of head and neck cancer Fenner et al. (43) showed in 2005 that the REPP86 labeling index differed significantly between normal tissue and squamous cell carcinoma of the oral cavity. REPP86 expression was not related to tumor size, lymph node invasion, or histopathological grading but was positively correlated with Ki-67 index.
REPP86 expression in SCCL as well as correlation of REPP86 to prognosis in HNSCC has not been investigated to date but correlation to prognosis has been shown in mantle cell lymphoma (40). The authors of the above named study found that patients with REPP86 expression of more than 10% showed the shortest survival. These results are in good accordance with the results of the present study except that the proliferation cut-off was much lower in the mantle cell lymphoma with 10% compared to the cut-off in our study of 25%, which was the median of proliferating cells in all SCCL.
We recently published a study showing Ki-67 as a good prognostic indicator for laryngeal squamous cell carcinoma (12). The study presented here shows similar results compared to the Ki-67 study regarding the proliferative activity in comparison to the TNM classification, however Ki-S2 was able to distinguish a significant difference between M0 and M1 stages, while Ki-S11 could not. A strong correlation (p=0.001) between proliferation activity and histopathological grading was also evident for both antibodies. Both antibodies showed similar results regarding the proliferative activity and the overall five-year survival rate (p<0.05 respectively). Regarding the relapse-free survival, the Ki-S2 antibody had a better predictive value with p=0.001 compared to the Ki-S11 antibody (p<0.05). Therefore Ki-S2 better predicts the relapse-free survival in our cohort of patients with SCCL than the Ki-S11 antibody.
In conclusion, the findings presented here using the Ki-S2 antibody on SCCL to determine proliferative activity seem to be in accordance with previously published data for head and neck tumors as well as for tumors derived from other tumor sites or even from other tissue entities. The results were the more comparable, the larger and homogeneous the patient groups were (33, 44). High proliferative activity seems to correlate with a worse clinical course and stronger metastatic potential. Finally, REPP86 proliferation activity stained with the Ki-S2 antibody is able to predict the overall-survival and the relapse-free survival of patients with SCCL. The relapse-free survival is even better predicted than by Ki-67 staining. However, both markers reveal statistically significant prediction of prognosis in SCCL and could be helpful tumor-biological markers in the clinical oncology for SCCL.
- Received March 17, 2010.
- Revision received June 2, 2010.
- Accepted June 7, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.