


Abstract
Background: The aim of the study was to assess the prognostic role of CD4 and CD8 expression and the type, density, localization and distribution of tumor infiltrating lymphocytes (TILs) in patients with breast cancer. Materials and Methods: Tissue samples were obtained from 88 breast cancer patients with operable disease and ductal histology. Forty-three women had pathologically confirmed axillary lymph node involvement. The TILs and expression of CD8 (cytotoxic T-cells) and CD4 (T-helper cells) were evaluated in the tumor samples using mouse monoclonal antibodies. Results: Thirteen patients relapsed; nine of them had strong expression of CD4 and CD8, which was statistically significant. The patients with high expression of CD4 or CD8 had distinctly worse cancer specific overall survival (OS). High correlations between CD4 and CD8 expression and lymph node status and intensity of lymphatic infiltrate as well as between both markers were found. Conclusion: The analysis of tumor-infiltrating immune cells may be a valuable prognostic tool and a marker of lymph node involvement.
Lymphocytes are mobile cells, continuously recirculating between the blood and tissues, returning to the blood through the lymphatic system. It has been stated that peripheral blood contains approximately 2% of all lymphocytes and the rest of the cells can be found in the lymphatic organs such as the tonsils, spleen, young thymus and especially in the lymph nodes (1). The correlation between the immune infiltrate and breast cancer has been widely investigated since the early work of Black (2). Several studies have stated that the tumors are infiltrated by a heterogeneous population of immune cells, such as T-cells, B-cells, natural killer (NK) cells and macrophages (3). Tumor infiltrating lymphocytes (TILs), a primary immune component infiltrating solid tumors, are considered to be the manifestation of the host antitumor reaction.
The majority of TILs in solid tumors are of the CD3+ T-cell phenotype, which includes CD4+ helper cells (Th1 and Th2 subtypes), CD4+ regulatory T-cells and CD8+ cytotoxic T lymphocytes (CTLs) (4). CTLs destroy tumor cells as a result of triggering apoptosis, therefore they may have an effect on tumor growth.
Evidence has suggested that the type, density and location of TILs may influence the prognosis. No definitive conclusion has been reached regarding the efficacy of T-cell-dependent immune mechanisms or the correlation between the extent, type of lymphocyte infiltration and the tumor progression in the carcinoma of the breast (5).
The aim of this study was to confirm the presence of an immune infiltrate in human breast cancer, characterize this infiltrate phenotypically and examine the type, density, localization and distribution of the TILs. The findings were compared with established markers of prognosis such as tumor size, grade, lymph node status, estrogen receptor alpha (ERα), progesterone receptor (PgR) and HER-2/neu (human epidermal growth factor receptor 2) expression.
Materials and Methods
Patients. Tissue samples were obtained from 88 breast cancer patients with invasive ductal breast carcinoma treated in the Lower Silesian Oncological Centre between May 2003 and December 2004. The median age of the patients was 62 years (range 29-79).
All the patients presented with operable disease, the tumors were strictly confined to the breasts, without distant metastasis; cases with involvement of the skin, hypodermis or pectoral muscles were excluded.
All the patients underwent curative surgery with axillary lymph node dissection, and none of these patients had received preoperative antitumor therapy.
In 59 patients (67.04%) adjuvant chemotherapy and in 38 (43.18%) radiotherapy were performed. The 57 patients (64.77%) with ER or PgR expression were subjected to hormonotherapy. In all the patients, invasive ductal cancer was diagnosed: 34 (38.64%) with stage I according to AJCC (American Joint Committee on Cancer), 29 (32.95%) with stage II and 25 (28.41%) with stage III. In 43 (48.86%) patients, metastases in the axillary lymph nodes were detected.
The clinical and pathological parameters of all the cases, including histological type, grade, lymph node status, tumor size, ER, PgR and HER2/neu expressions, clinical and pathological stage as well as data concerning treatment and follow-up were obtained from the archive and medical records of the hospital. The histological parameters and receptor status were reviewed by two pathologists based on material obtained from the archive of the Lower Silesian Oncological Centre Pathology Department.
The median follow-up was 39 months (range 28 to 57). During the follow-up period 13 patients relapsed: 12 with distant metastases and 1 with local recurrence. Survival data included the disease-free survival (DFS) and cancer-specific overall survival (OS).
The key characteristics of the patients are summarized in Tables I and II. The use of the specimens and data for research purposes was approved by the Wroclaw Medical University Ethics Committee.
Immunohistochemistry. Formalin-fixed paraffin-embedded breast cancer tissue was freshly cut (4 μm). The sections were mounted on Superfrost slides (Menzel Gläser, Braunschweig, Germany), dewaxed with xylene and gradually rehydrated. The activity of endogenous peroxidase was blocked by 30 min incubation in 1% H2O2 (Peroxidase-Blocking Reagent, S2001; DakoCytomation, Glostrup, Denmark). Immunohistochemical reactions were performed using monoclonal mouse antibodies against CD4 (NCL-CD4-368, Clone 4B12; Novocastra, Wetzlar, Germany) at dilution 1:10, and monoclonal mouse antibodies against CD8 (NCL-CD8-295; Clone 1A5, Novocastra) at dilution 1:20. The antibodies were diluted in Antibody Diluent, Background Reducing (S0809; DakoCytomation). The sections were incubated with the antibodies for 1 hour at room temperature. Subsequently, incubations were performed with biotinylated antibodies (15 min, room temperature) and with streptavidin-biotinylated peroxidase complex (15 min, room temperature) (LSAB+, HRP, K0690; DakoCytomation). DAB (K3468; DakoCytomation) was used as a chromogen (10 min at room temperature). All the sections were counterstained with Meyer's hematoxylin. In every case, controls were included in which the specific antibody was substituted by Primary Mouse Negative Control (DakoCytomation).
The results of the immunohistochemical reactions were evaluated independently by two pathologists and appraised using a semiquantitative scale scored according to the percentage of positive stained cells as follows: 0=none, 1 = up to 33% cells in tumor were positive, 2 = 33-66% positive cells and 3=more than 66% cells positive.
The status of the TILs was also examined. The intensity of the lymphocytic infiltrate was scored according to the general intensity and density as: 1, low intensity; 2, moderate intensity and 3, high intensity infiltrate.
Clinical and pathological characteristics of patients with breast cancer.
The localization and distribution of the infiltrate in according to which region of tumor it dominated were recorded as: central part of the tumor (CE), on the tumor margins (MAR) or lymphocytic accumulation in the lymph nodes (LN). Addictionally, the type of lymphocytic infiltrate was estimated as: diffuse type (DT), nodule type (NT) or mixed of both types (MT).
Characteristics of treatment in the breast cancer patients.
Statistical analysis. The univariate significance of differences in marker expression was appraised by Student's t-test for binary or categorical covariates, or by Spearman's rank correlation for ordered covariates. The specific OS and DFS were estimated using the Kaplan-Meier method and comparison between study groups was performed with the log-rank test. The survival time was measured from the date of diagnosis to the date of death or date of last follow-up. In all the tests, the significance level was set at 0.05 and all were two-sided tests. The statistical analyses were performed using the Software StatSoft Inc. STATISTICA for Windows ver.7.0 A, Tulsa, OK, USA.
Results
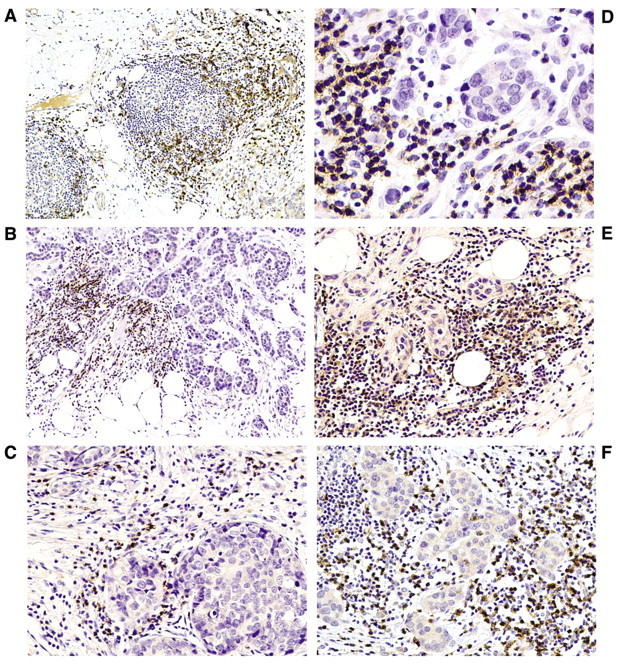
Staining with the monoclonal antibody against CD4 demonstrated an infiltrate in all except six of the tumors (6.82%). Level 1 expression was noted in 34 tumors (38.64%), level 2 in 38 (43.18%) and level 3 in 10 (11.36%). Staining with the monoclonal antibody against CD8 exhibited no expression in four tumors (4.54%), level 1 expression in 11 (12.50%), level 2 in 34 (38.64%) and level 3 in 39 (44.32%). A strong correlation (R Spearman's=0.69, Student's t-test=7.13) between expression intensity of CD4 and CD8 (p<0.001) was observed. The general intensity and density of the lymphocytic infiltrate was: in four tumors (4.54%) no infiltrate, in 39 (44.32%) low intensity, in 32 (36.36%) moderate and in 13 (14.78%) high intensity. A high correlation between the intensity of lymphatic infiltrate and CD4 expression (R Spearman's=0.71, Student's t-test=6.96, p<0.001) as well as CD8 expression (R Spearman's=0.62, Student's t-test=6.12, p<0.001) was also observed. In the majority of the tumors with lymphocytic infiltrate infiltration was observed on the tumor margins (MAR, 76; CE, 59; LN, 14). In 49 tumors, the lymphocytic infiltrate, was characterized by diffuse type and in 35 tumors it was mixed. Figure 1A to 1H shows the types of lymphocyte infiltrate and the results of CD8 and CD4 staining.
Correlation between CD4, CD8 expression and clinicopathological parameters.
A close relationship between CD4, CD8 expression and node status was found (CD4 vs. cN, p=0.016; CD4 vs. pN, p=0.037; CD8 vs. cN, p=0.005; CD8 vs. pN, p=0.0008). No correlations between CD4 or CD8 expression and established markers of prognosis such as tumor clinical and pathological size, histological grade, ER, PgR and HER-2/neu expressions were observed (details in Table III).
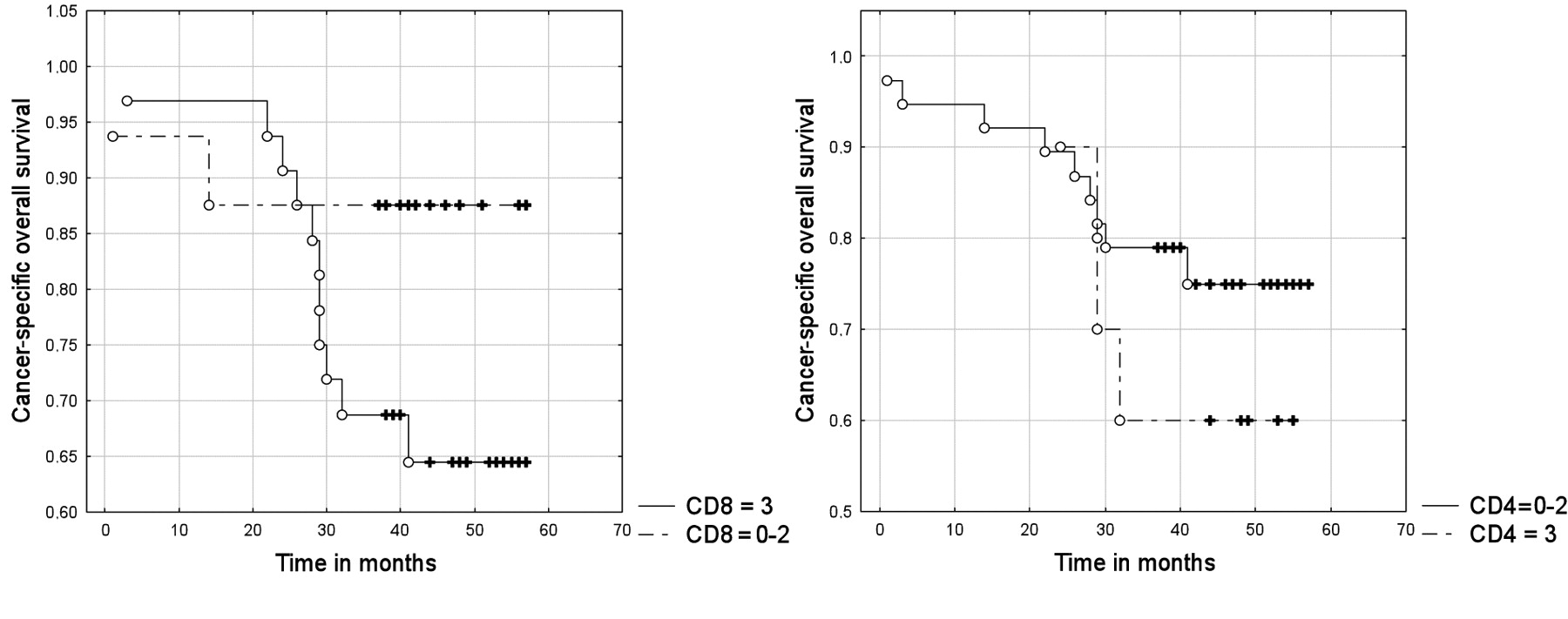
The prognostic value of the expression of both markers was also analyzed. The patients with high expression of CD4 or CD8 had distinctly worse cancer-specific OS (log-rank test: p=0.399 for CD4, p=0.151 for CD8, Figure 2) and DFS (log-rank test: p=0.297 for CD4 and p=0.131 for CD8). The differences were not statistically significant, probably because of the short follow-up (median 39 months) and the small group of relapsed patients.
Discussion
The most important, independent prognostic factors in breast carcinoma are tumor size and number of histologically positive axillary lymph nodes (6-8). A direct relationship between the risk of distant recurrence and the number of involved axillary nodes has been established (9). Even patients with very small tumors and minimal involvement of a single axillary lymph node have a significantly worse prognosis compared with patients without nodal involvement (10). For years, the standard treatment for patients with operable breast carcinoma included the complete dissection of 10 -30 axillary lymph nodes. More than half of patients were found to have metastasis-free lymph nodes and thus had been subjected to unnecessary surgical risk and complications (11, 12). It is widely known that regional lymph nodes constitute an important immunological defense or barrier against tumor expansion (13). Several studies reported that the removal of uninvolved lymph nodes might have a devastating effect on the immunological defense of the host against systemic metastasis or tumor recurrence (14).


Invasive breast carcinoma. A, Follicular lymphoid infiltrate. Strong CD8 expression in peritumoral lymphocytes. Original magnification ×100. B, Dispersed lymphoid infiltrate. Strong immunopositivity for CD8 in peritumoral lymphocytes. Original magnification ×100. C, Intratumoral lymphoid infiltrate. Strong CD8 expression in lymphocytes dispersed throughout the tumor. Original magnification ×200. D, Intratumoral lymphoid infiltrate. Strong CD8 membrane staining in lymphocytes scattered within tumor. Original magnification ×400. E, Intratumoral lymphoid infiltrate. Strong CD4 membrane staining in lymphocytes scattered within tumor. Original magnification ×200. F, Follicular lymphoid infiltrate. Strong CD4 expression in peritumoral lymphocytes. Original magnification ×200. G, Dispersed lymphoid infiltrate. Strong immunopositivity for CD4 in peritumoral lymphocytes. Original magnification ×200. H, Intratumoral lymphoid infiltrate. Strong CD4 expression in lymphocytes dispersed throughout the tumor. Original magnification ×200. DAB staining.
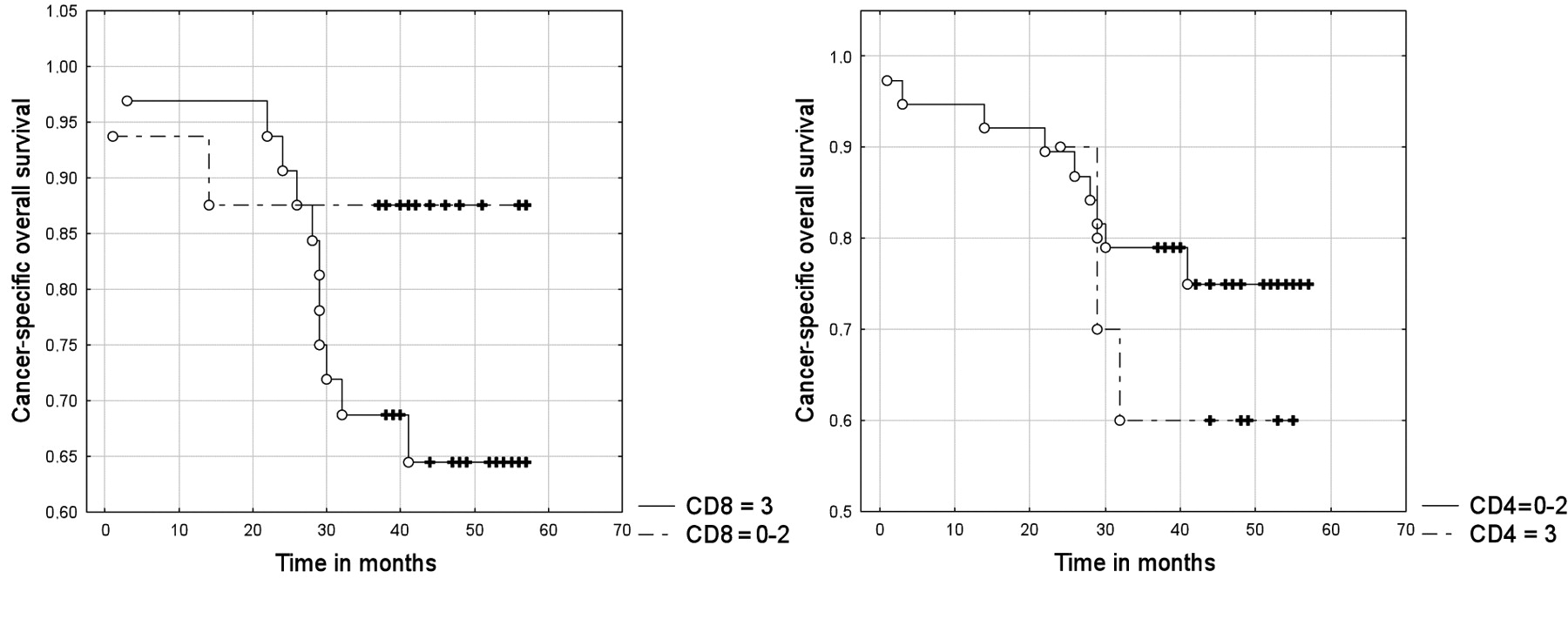
Cancer-specific overall survival in relation to expressions of CD4 and CD8.
Aaltomaa et al. (3) have studied the predictive value of lymphocyte infiltrates (LI) assessed as weak, moderate or dense in a group of 489 breast carcinoma patients and showed that dense lymphocyte infiltrate predicted axillary lymph node metastasis. Those results were comparable with those of the present study.
Georgiannos et al. (15) observed marked variation in intensity of the infiltrate between individual carcinomas and most of the tumors having a moderate or intense infiltrate. T helper (CD4+) and cytotoxic T-cells (CD8+) were found in all the primary tumors but without a recognizable pattern of distribution within the individual tumors and the infiltrate ranged from one that was CD4+ predominant to one that was CD8+ predominant. In the present study, there was a strong correlation between the expression intensity of CD4 and CD8 (p<0.001) and between both markers and TIL (p<0.001). Thus we believe that CD4 and CD8 are good indicators of the intensity of tumor-infiltration lymphocytes. Some authors found a significant connection between the intensity of the TILs (CD3+) and the number of positive lymph nodes, as well as the intensity of CD4 and CD8 expression with ER expression. La Rocca et al. (16) stated that the number of CD4-expressing cells as well as CD 8 cells was higher in N0 than in N+ invasive ductal breast lesions. Unfortunately, their study was conducted on a rather small and very differentiated group of patients, only 35 women in stages T1-T4 and N0-N2. Rubbert et al. (17) also showed a decline of CD8+ T-cells in regional lymph nodes, particularly in lymph nodes with cancer involvement in breast carcinoma patients. The data indicated that the draining lymph nodes of cancer patients may host specific or non-specific suppression of NK and CD8+ T-cells, which seemed to be responsible for their poor immunological activity. Those findings were opposite to those of the present study, in which very strong correlation between CD4 and CD8 expression and axillary lymph node metastasis (p<0.05 for CD4 and p<0.001 for CD8) was observed. Moreover, in these patients, no significant correlation with hormone receptor status was found.
Similar to the present results, Nakano et al. (18) found a positive correlation between the number of lymphocytes, more abundant infiltration of tumor tissue by CD8+ and CD4+ T-cells and shorter survival in 221 renal cell carcinoma patients.
Macchetti et al. (19) indicated the same trend using flow cytometry to analyze the TILs of 23 breast carcinoma patients with T1 to T2 tumors in an attempt to correlate the phenotypical markers of tumor-infiltrating leukocytes with axillary lymph node status. In the patients with lymph node metastasis, an increased mean percentage of tumor-infiltrating CD4+ T-cells, but not CD8+ T-cells was observed and was correlated with worse prognosis.
In contrast to the present study, Naito et al. (20) in colorectal carcinoma and Sato et al. (21) in ovarian carcinoma stated that a high intensity of TILs in the cancer stroma and epithelium or along the invasive margin correlated with improved survival. Moreover, the subgroup of patients with high intraepithelial CD8+/CD4+ ratios (>1.94) in ovarian carcinoma demonstrated improved survival. Eerola et al. (22) published similar results in patients with small cell lung carcinoma in whom a high number of TILs was associated with small tumor size, low clinical stage and therefore favorable prognosis. One possible explanation for these differences is that the tissue environments in breast, small cell lung, colorectal and ovarian carcinomas are different. Furthermore, the biology of these four kinds of cancer, the development of tumors and localization of metastases are entirely distinct. Due to differences in the histological construction of breast carcinoma, the stromal and epithelial distribution of TILs could not be assessed. Neither could the intratumoral and peritumoral differences of CD4+ and CD8+ be evaluated as was done by Nedergaard et al. (23) in squamous cell cervical carcinoma patients.
Another reason for the discrepancy between the present results and the studies of Zhang et al. (24) in ovarian carcinoma and Gao et al. (25) in hepatocellular carcinoma might have been due to different methods of assessing the TILs (flow cytometry, tissue microarrays) and the completely different tissue environment of the aforementioned tumors.
Conclusion
In early breast cancer, the presence of CD8+ and CD4+ cells correlates with lymph node involvement and unfavorable prognosis, suggesting that immune response has an influence on the behavior of malignant breast tumors. The analysis of tumor-infiltrating immune cells may predict lymph node involvement and higher risk of recurrence.
Footnotes
-
↵* Both authors contributed equally to this work.
- Received March 3, 2009.
- Revision received May 11, 2009.
- Accepted May 18, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Germline genetic variants associated with leukocyte-genes predict tumor recurrence in breast cancer patients
- A Standardized Evaluation Method for FOXP3+ Tregs and CD8+ T-cells in Breast Carcinoma: Association With Breast Carcinoma Subtypes, Stage and Prognosis
- Long-term Follow-up After Interstitial Laser Thermotherapy of Breast Cancer
- Tumoral Lymphocytic Infiltration and Expression of the Chemokine CXCL10 in Breast Cancers from the Ontario Familial Breast Cancer Registry